

Airway Assessment
2cKbSEQ
2cKbSEQ

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
TONGUE ABNORMALITIES<br />
Direct laryngoscopy requires the tongue to be mobile and retracted from the line of vision.<br />
Problems arise when the tongue is abnormally large or poorly compliant. Rosenstock and<br />
Kristensen suggest that tongue mobility may be a sensitive indicator of difficult laryngoscopy 45 .<br />
MALLAMPATI<br />
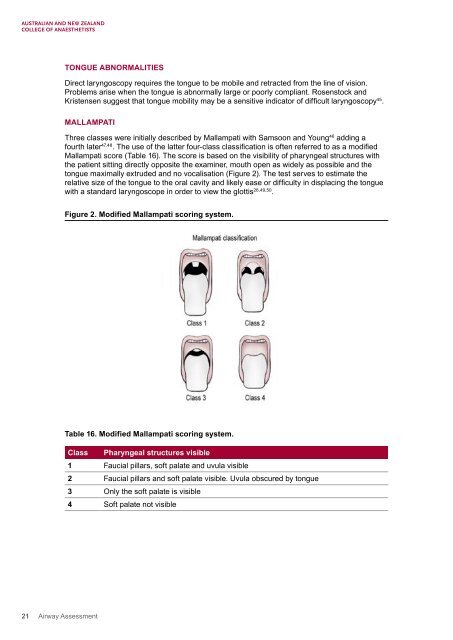
Three classes were initially described by Mallampati with Samsoon and Young 46 adding a<br />
fourth later 47,48 . The use of the latter four-class classification is often referred to as a modified<br />
Mallampati score (Table 16). The score is based on the visibility of pharyngeal structures with<br />
the patient sitting directly opposite the examiner, mouth open as widely as possible and the<br />
tongue maximally extruded and no vocalisation (Figure 2). The test serves to estimate the<br />
relative size of the tongue to the oral cavity and likely ease or difficulty in displacing the tongue<br />
with a standard laryngoscope in order to view the glottis 26,49,50 .<br />
Figure 2. Modified Mallampati scoring system.<br />
Table 16. Modified Mallampati scoring system.<br />
Class Pharyngeal structures visible<br />
1 Faucial pillars, soft palate and uvula visible<br />
2 Faucial pillars and soft palate visible. Uvula obscured by tongue<br />
3 Only the soft palate is visible<br />
4 Soft palate not visible<br />
21 <strong>Airway</strong> <strong>Assessment</strong>