

Airway Assessment
2cKbSEQ
2cKbSEQ

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
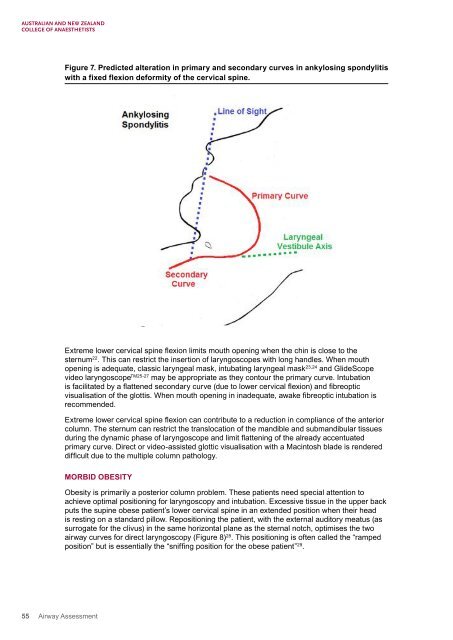
Figure 7. Predicted alteration in primary and secondary curves in ankylosing spondylitis<br />
with a fixed flexion deformity of the cervical spine.<br />
Extreme lower cervical spine flexion limits mouth opening when the chin is close to the<br />
sternum 22 . This can restrict the insertion of laryngoscopes with long handles. When mouth<br />
opening is adequate, classic laryngeal mask, intubating laryngeal mask 23,24 and GlideScope<br />
video laryngoscope TM25-27 may be appropriate as they contour the primary curve. Intubation<br />
is facilitated by a flattened secondary curve (due to lower cervical flexion) and fibreoptic<br />
visualisation of the glottis. When mouth opening in inadequate, awake fibreoptic intubation is<br />
recommended.<br />
Extreme lower cervical spine flexion can contribute to a reduction in compliance of the anterior<br />
column. The sternum can restrict the translocation of the mandible and submandibular tissues<br />
during the dynamic phase of laryngoscope and limit flattening of the already accentuated<br />
primary curve. Direct or video-assisted glottic visualisation with a Macintosh blade is rendered<br />
difficult due to the multiple column pathology.<br />
MORBID OBESITY<br />
Obesity is primarily a posterior column problem. These patients need special attention to<br />
achieve optimal positioning for laryngoscopy and intubation. Excessive tissue in the upper back<br />
puts the supine obese patient’s lower cervical spine in an extended position when their head<br />
is resting on a standard pillow. Repositioning the patient, with the external auditory meatus (as<br />
surrogate for the clivus) in the same horizontal plane as the sternal notch, optimises the two<br />
airway curves for direct laryngoscopy (Figure 8) 28 . This positioning is often called the “ramped<br />
position” but is essentially the “sniffing position for the obese patient” 29 .<br />
55 <strong>Airway</strong> <strong>Assessment</strong>