

Airway Assessment
2cKbSEQ
2cKbSEQ

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
POSTERIOR COLUMN<br />
The original descriptions of the “sniffing position” emphasised the importance of appropriate<br />
head and neck positioning prior to laryngoscopy 1,2 . The latter work by Greenland and<br />
colleagues reinforced the efficacy of the sniffing position in optimising direct laryngoscopy and<br />
intubating conditions 10 . Achieving the sniffing position is governed by the ability to flex the lower<br />
cervical spine and extend the occipito-atlanto-axial complex. Horton asserted the “ideal angle”<br />
for upper-neck extension and lower-neck flexion to be 15 degrees and 35 degrees, respectively<br />
(Figure 8) 16 . To achieve a true sniffing position in obese patients “ramping” may be required.<br />
The external auditory meatus (as a surrogate marker for the clivus or C1 vertebrae) and the<br />
sternal notch are aligned in the horizontal plane in the ramped position 17-19 .<br />
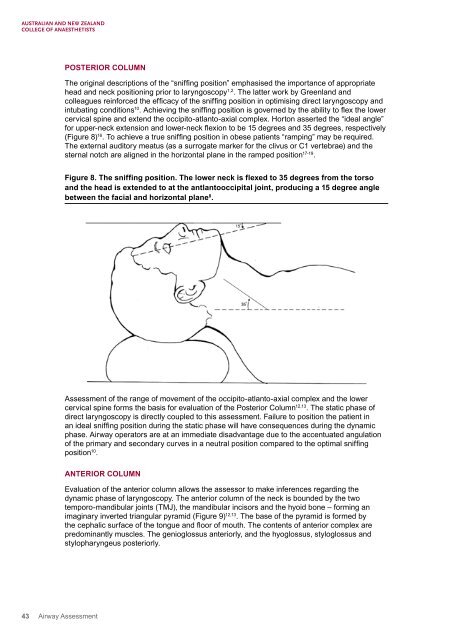
Figure 8. The sniffing position. The lower neck is flexed to 35 degrees from the torso<br />
and the head is extended to at the antlantooccipital joint, producing a 15 degree angle<br />
between the facial and horizontal plane 8 .<br />
<strong>Assessment</strong> of the range of movement of the occipito-atlanto-axial complex and the lower<br />
cervical spine forms the basis for evaluation of the Posterior Column 12,13 . The static phase of<br />
direct laryngoscopy is directly coupled to this assessment. Failure to position the patient in<br />
an ideal sniffing position during the static phase will have consequences during the dynamic<br />
phase. <strong>Airway</strong> operators are at an immediate disadvantage due to the accentuated angulation<br />
of the primary and secondary curves in a neutral position compared to the optimal sniffing<br />
position 10 .<br />
ANTERIOR COLUMN<br />
Evaluation of the anterior column allows the assessor to make inferences regarding the<br />
dynamic phase of laryngoscopy. The anterior column of the neck is bounded by the two<br />
temporo-mandibular joints (TMJ), the mandibular incisors and the hyoid bone – forming an<br />
imaginary inverted triangular pyramid (Figure 9) 12,13 . The base of the pyramid is formed by<br />
the cephalic surface of the tongue and floor of mouth. The contents of anterior complex are<br />
predominantly muscles. The genioglossus anteriorly, and the hyoglossus, styloglossus and<br />
stylopharyngeus posteriorly.<br />
43 <strong>Airway</strong> <strong>Assessment</strong>