

Airway Assessment
2cKbSEQ
2cKbSEQ

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
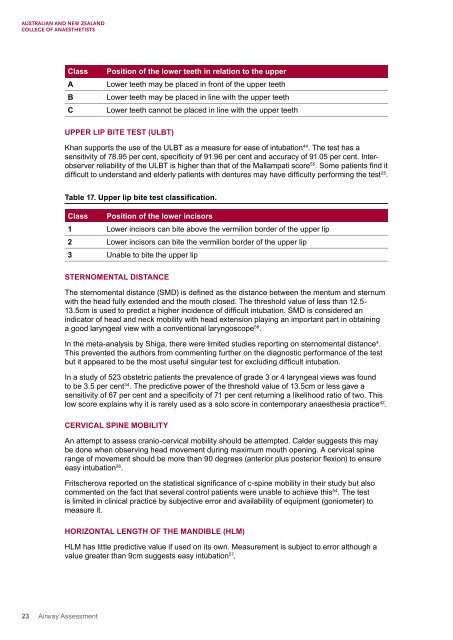
Class<br />
A<br />
B<br />
C<br />
Position of the lower teeth in relation to the upper<br />
Lower teeth may be placed in front of the upper teeth<br />
Lower teeth may be placed in line with the upper teeth<br />
Lower teeth cannot be placed in line with the upper teeth<br />
UPPER LIP BITE TEST (ULBT)<br />
Khan supports the use of the ULBT as a measure for ease of intubation 44 . The test has a<br />
sensitivity of 78.95 per cent, specificity of 91.96 per cent and accuracy of 91.05 per cent. Interobserver<br />
reliability of the ULBT is higher than that of the Mallampati score 55 . Some patients find it<br />
difficult to understand and elderly patients with dentures may have difficulty performing the test 25 .<br />
Table 17. Upper lip bite test classification.<br />
Class Position of the lower incisors<br />
1 Lower incisors can bite above the vermilion border of the upper lip<br />
2 Lower incisors can bite the vermilion border of the upper lip<br />
3 Unable to bite the upper lip<br />
STERNOMENTAL DISTANCE<br />
The sternomental distance (SMD) is defined as the distance between the mentum and sternum<br />
with the head fully extended and the mouth closed. The threshold value of less than 12.5-<br />
13.5cm is used to predict a higher incidence of difficult intubation. SMD is considered an<br />
indicator of head and neck mobility with head extension playing an important part in obtaining<br />
a good laryngeal view with a conventional laryngoscope 56 .<br />
In the meta-analysis by Shiga, there were limited studies reporting on sternomental distance 4 .<br />
This prevented the authors from commenting further on the diagnostic performance of the test<br />
but it appeared to be the most useful singular test for excluding difficult intubation.<br />
In a study of 523 obstetric patients the prevalence of grade 3 or 4 laryngeal views was found<br />
to be 3.5 per cent 34 . The predictive power of the threshold value of 13.5cm or less gave a<br />
sensitivity of 67 per cent and a specificity of 71 per cent returning a likelihood ratio of two. This<br />
low score explains why it is rarely used as a solo score in contemporary anaesthesia practice 42 .<br />
CERVICAL SPINE MOBILITY<br />
An attempt to assess cranio-cervical mobility should be attempted. Calder suggests this may<br />
be done when observing head movement during maximum mouth opening. A cervical spine<br />
range of movement should be more than 90 degrees (anterior plus posterior flexion) to ensure<br />
easy intubation 26 .<br />
Fritscherova reported on the statistical significance of c-spine mobility in their study but also<br />
commented on the fact that several control patients were unable to achieve this 54 . The test<br />
is limited in clinical practice by subjective error and availability of equipment (goniometer) to<br />
measure it.<br />
HORIZONTAL LENGTH OF THE MANDIBLE (HLM)<br />
HLM has little predictive value if used on its own. Measurement is subject to error although a<br />
value greater than 9cm suggests easy intubation 57 .<br />
23 <strong>Airway</strong> <strong>Assessment</strong>