

Airway Assessment
2cKbSEQ
2cKbSEQ

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
RE-EXAMINING THE FOUNDATIONS OF AIRWAY ASSESSMENT AND MANAGEMENT<br />
In airway assessment, the discovery of abnormal signs and symptoms often leads to the<br />
presumption of the “difficult airway”. The determination of an abnormality during the assessment<br />
phase is only the first step towards a working diagnosis. Unless we understand the fundamentals<br />
of airway anatomy, laryngoscopy and intubation, evaluation of an airway is fruitless.<br />
With the advent of supraglottic airway devices, more intuitive video laryngoscopes and other<br />
developments in airway equipment, airway management is becoming easier. This trend could<br />
lead to the incorrect assumption that airway assessment is less important. This is far from the<br />
truth.<br />
There is a disconnect between assessment and its application. There is a divergence in<br />
teaching between pattern recognition and conceptual understanding. This article presents an<br />
anatomical foundation for successful direct laryngoscopy and tracheal intubation and a model<br />
for structured airway assessment.<br />
I) THE TWO-CURVE THEORY<br />
In 1944, Banister and Macbeth explored the anatomical basis of direct laryngoscopy via the<br />
description of the “three-axis alignment theory” 1 . The three-axis theory was a refinement<br />
of Magill’s formal description of the “sniffing position” as the preferred intubating position 2 .<br />
Although contentious, the theory has been a mainstay of airway teaching 3-8 .<br />
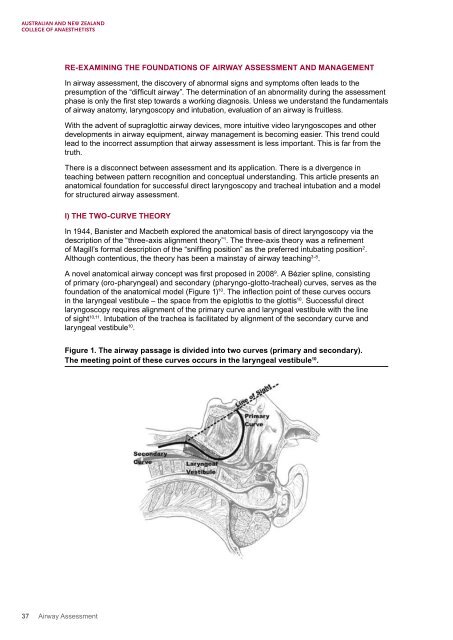
A novel anatomical airway concept was first proposed in 2008 9 . A Bézier spline, consisting<br />
of primary (oro-pharyngeal) and secondary (pharyngo-glotto-tracheal) curves, serves as the<br />
foundation of the anatomical model (Figure 1) 10 . The inflection point of these curves occurs<br />
in the laryngeal vestibule – the space from the epiglottis to the glottis 10 . Successful direct<br />
laryngoscopy requires alignment of the primary curve and laryngeal vestibule with the line<br />
of sight 10,11 . Intubation of the trachea is facilitated by alignment of the secondary curve and<br />
laryngeal vestibule 10 .<br />
Figure 1. The airway passage is divided into two curves (primary and secondary).<br />
The meeting point of these curves occurs in the laryngeal vestibule 10 .<br />
37 <strong>Airway</strong> <strong>Assessment</strong>