

Airway Assessment
2cKbSEQ
2cKbSEQ

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
BEDSIDE PREDICTORS OF DIFFICULTY WITH INTUBATION VIA DIRECT LARYNGOSCOPY<br />
A variety of features on external examination suggest difficult laryngoscopy: small or recessed<br />
mandible, poor dentition, a short neck, facial disruption, presence of a halo-thoracic brace<br />
or cervical spine collar and a large tongue are just some features that suggest difficult direct<br />
laryngoscopy. Mallampati class one and two patients are associated with low intubation failure<br />
rates. Class three patients, however, have an intubation failure rate greater than 10 per cent.<br />
Signs of impending obstruction include stridor, voice changes and failure to swallow secretions.<br />
Presence of stridor indicates that the airway diameter has been reduced to 4.0mm or less.<br />
Positioning of the head and neck is vital for successful direct laryngoscopy. Classic positioning<br />
advice is to place the patient in the “sniffing the morning air” position – that is neck flexion<br />
and head extension. Practitioners should beware in patients with limited neck extension – for<br />
example, patients with cervical spine injuries, pathologies such as ankylosing spondylitis,<br />
radiation changes or patients in cervical spine immobilisation collars.<br />
CORMACK AND LEHANE<br />
Cormack and Lehane defined laryngoscopy in terms of the best view of the glottis during<br />
conventional laryngoscopy with a direct view and performed as a best attempt 29 . The optimal<br />
laryngeal view includes external manipulation. Yentis and Lee 30 added a modified version that<br />
subdivided grade 2 into grade 2a and 2b. This is known as the modified Cormack and Lehane<br />
classification. Cook’s modification 31 subdivided grade 3 depending on whether the epiglottis<br />
could be elevated from the posterior pharyngeal wall using a bougie or introducer (Table 7).<br />
The Cormack and Lehane laryngoscopic grading has been used to define difficult intubation with<br />
grade 3 and grade 4 equated with difficulty, although it was never intended for this purpose 30 .<br />
Benumof 32 defined the best attempt at laryngoscopy as that performed by a reasonably skilled<br />
and experienced practitioner, using the optimum type and length of laryngoscope blade and the<br />
patient in the optimal “sniffing” position with no significant muscle tone together with the use of<br />
external laryngeal manipulation as appropriate. When confronted with the unexpected difficult<br />
intubation it is necessary to ensure that laryngoscopy conditions as above are optimal.<br />
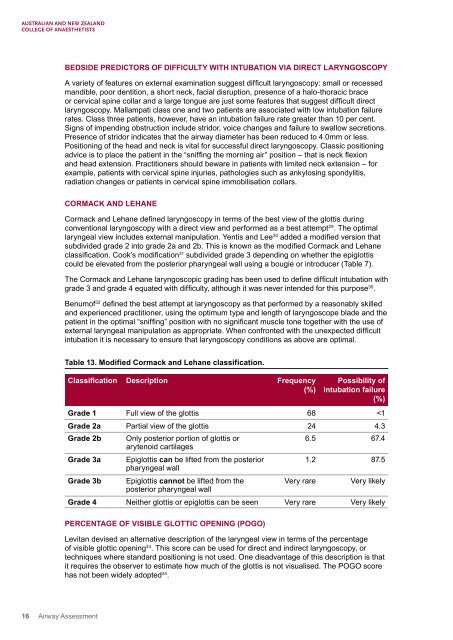
Table 13. Modified Cormack and Lehane classification.<br />
Classification Description Frequency<br />
(%)<br />
Possibility of<br />
intubation failure<br />
(%)<br />
Grade 1 Full view of the glottis 68