ESC Textbook of Cardiovascular Imaging - sample
Discover the ESC Textbook of Cardiovascular Imaging 2nd edition
Discover the ESC Textbook of Cardiovascular Imaging 2nd edition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
standardized data acquisition in transthoracic echocardiography 9<br />
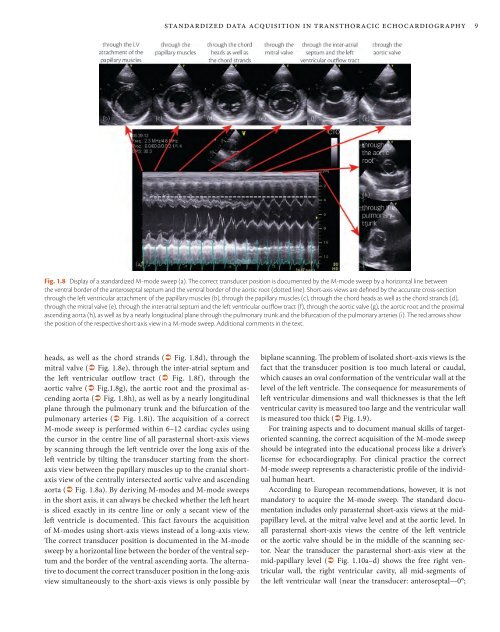
Fig. 1.8 Display <strong>of</strong> a standardized M-mode sweep (a). The correct transducer position is documented by the M-mode sweep by a horizontal line between<br />
the ventral border <strong>of</strong> the anteroseptal septum and the ventral border <strong>of</strong> the aortic root (dotted line). Short-axis views are defined by the accurate cross-section<br />
through the left ventricular attachment <strong>of</strong> the papillary muscles (b), through the papillary muscles (c), through the chord heads as well as the chord strands (d),<br />
through the mitral valve (e), through the inter-atrial septum and the left ventricular outflow tract (f), through the aortic valve (g), the aortic root and the proximal<br />
ascending aorta (h), as well as by a nearly longitudinal plane through the pulmonary trunk and the bifurcation <strong>of</strong> the pulmonary arteries (i). The red arrows show<br />
the position <strong>of</strong> the respective short-axis view in a M-mode sweep. Additional comments in the text.<br />
heads, as well as the chord strands ( Fig. 1.8d), through the<br />
mitral valve ( Fig. 1.8e), through the inter-atrial septum and<br />
the left ventricular outflow tract ( Fig. 1.8f), through the<br />
aortic valve ( Fig.1.8g), the aortic root and the proximal ascending<br />
aorta ( Fig. 1.8h), as well as by a nearly longitudinal<br />
plane through the pulmonary trunk and the bifurcation <strong>of</strong> the<br />
pulmonary arteries ( Fig. 1.8i). The acquisition <strong>of</strong> a correct<br />
M-mode sweep is performed within 6–12 cardiac cycles using<br />
the cursor in the centre line <strong>of</strong> all parasternal short-axis views<br />
by scanning through the left ventricle over the long axis <strong>of</strong> the<br />
left ventricle by tilting the transducer starting from the shortaxis<br />
view between the papillary muscles up to the cranial shortaxis<br />
view <strong>of</strong> the centrally intersected aortic valve and ascending<br />
aorta ( Fig. 1.8a). By deriving M-modes and M-mode sweeps<br />
in the short axis, it can always be checked whether the left heart<br />
is sliced exactly in its centre line or only a secant view <strong>of</strong> the<br />
left ventricle is documented. This fact favours the acquisition<br />
<strong>of</strong> M-modes using short-axis views instead <strong>of</strong> a long-axis view.<br />
The correct transducer position is documented in the M-mode<br />
sweep by a horizontal line between the border <strong>of</strong> the ventral septum<br />
and the border <strong>of</strong> the ventral ascending aorta. The alternative<br />
to document the correct transducer position in the long-axis<br />
view simultaneously to the short-axis views is only possible by<br />
biplane scanning. The problem <strong>of</strong> isolated short-axis views is the<br />
fact that the transducer position is too much lateral or caudal,<br />
which causes an oval conformation <strong>of</strong> the ventricular wall at the<br />
level <strong>of</strong> the left ventricle. The consequence for measurements <strong>of</strong><br />
left ventricular dimensions and wall thicknesses is that the left<br />
ventricular cavity is measured too large and the ventricular wall<br />
is measured too thick ( Fig. 1.9).<br />
For training aspects and to document manual skills <strong>of</strong> targetoriented<br />
scanning, the correct acquisition <strong>of</strong> the M-mode sweep<br />
should be integrated into the educational process like a driver’s<br />
license for echocardiography. For clinical practice the correct<br />
M-mode sweep represents a characteristic pr<strong>of</strong>ile <strong>of</strong> the individual<br />
human heart.<br />
According to European recommendations, however, it is not<br />
mandatory to acquire the M-mode sweep. The standard documentation<br />
includes only parasternal short-axis views at the midpapillary<br />
level, at the mitral valve level and at the aortic level. In<br />
all parasternal short-axis views the centre <strong>of</strong> the left ventricle<br />
or the aortic valve should be in the middle <strong>of</strong> the scanning sector.<br />
Near the transducer the parasternal short-axis view at the<br />
mid- papillary level ( Fig. 1.10a–d) shows the free right ventricular<br />
wall, the right ventricular cavity, all mid-segments <strong>of</strong><br />
the left ventricular wall (near the transducer: anteroseptal—0°;