

Anthem Blue Cross Blue Shield PPO Plan - Teamworks at Home ...
Anthem Blue Cross Blue Shield PPO Plan - Teamworks at Home ...
Anthem Blue Cross Blue Shield PPO Plan - Teamworks at Home ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
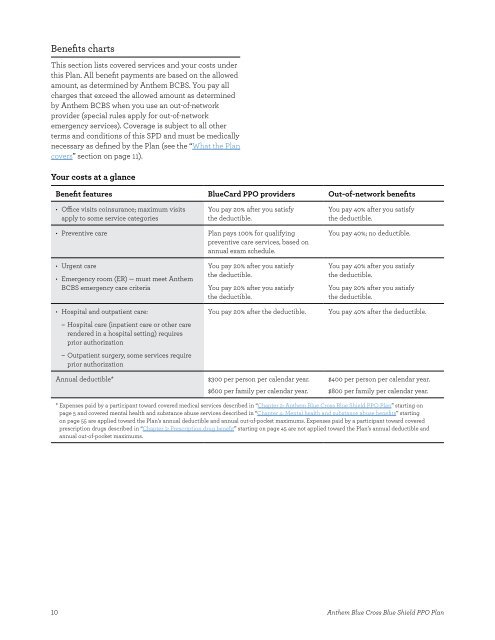
Benefts charts<br />
This section lists covered services and your costs under<br />
this <strong>Plan</strong>� All beneft payments are based on the allowed<br />
amount, as determined by <strong>Anthem</strong> BCBS� You pay all<br />
charges th<strong>at</strong> exceed the allowed amount as determined<br />
by <strong>Anthem</strong> BCBS when you use an out-of-network<br />
provider (special rules apply for out-of-network<br />
emergency services)� Coverage is subject to all other<br />
terms and conditions of this SPD and must be medically<br />
necessary as defned by the <strong>Plan</strong> (see the “Wh<strong>at</strong> the <strong>Plan</strong><br />
covers” section on page 11)�<br />
Your costs <strong>at</strong> a glance<br />
Beneft fe<strong>at</strong>ures <strong>Blue</strong>Card <strong>PPO</strong> providers Out-of-network benefts<br />
• Ofce visits coinsurance; maximum visits<br />
apply to some service c<strong>at</strong>egories<br />
You pay 20% after you s<strong>at</strong>isfy<br />
the deductible�<br />
• Preventive care <strong>Plan</strong> pays 100% for qualifying<br />
preventive care services, based on<br />
annual exam schedule�<br />
• Urgent care<br />
• Emergency room (ER) — must meet <strong>Anthem</strong><br />
BCBS emergency care criteria<br />
• Hospital and outp<strong>at</strong>ient care:<br />
– Hospital care (inp<strong>at</strong>ient care or other care<br />
rendered in a hospital setting) requires<br />
prior authoriz<strong>at</strong>ion<br />
– Outp<strong>at</strong>ient surgery, some services require<br />
prior authoriz<strong>at</strong>ion<br />
You pay 20% after you s<strong>at</strong>isfy<br />
the deductible�<br />
You pay 20% after you s<strong>at</strong>isfy<br />
the deductible�<br />
Annual deductible* $300 per person per calendar year�<br />
$600 per family per calendar year�<br />
10<br />
You pay 40% after you s<strong>at</strong>isfy<br />
the deductible�<br />
You pay 40%; no deductible�<br />
You pay 40% after you s<strong>at</strong>isfy<br />
the deductible�<br />
You pay 20% after you s<strong>at</strong>isfy<br />
the deductible�<br />
You pay 20% after the deductible� You pay 40% after the deductible�<br />
$400 per person per calendar year�<br />
$800 per family per calendar year�<br />
* Expenses paid by a participant toward covered medical services described in “Chapter 2: <strong>Anthem</strong> <strong>Blue</strong> <strong>Cross</strong> <strong>Blue</strong> <strong>Shield</strong> <strong>PPO</strong> <strong>Plan</strong>” starting on<br />
page 5 and covered mental health and substance abuse services described in “Chapter 4: Mental health and substance abuse benefts” starting<br />
on page 55 are applied toward the <strong>Plan</strong>’s annual deductible and annual out-of-pocket maximums� Expenses paid by a participant toward covered<br />
prescription drugs described in “Chapter 3: Prescription drug beneft” starting on page 45 are not applied toward the <strong>Plan</strong>’s annual deductible and<br />
annual out-of-pocket maximums�<br />
<strong>Anthem</strong> <strong>Blue</strong> <strong>Cross</strong> <strong>Blue</strong> <strong>Shield</strong> <strong>PPO</strong> <strong>Plan</strong>

