

Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic
Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic
Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
indications for hemispherectomy:<br />
common disorders with hemispheric epilepsy<br />
common disorders for which hemispherectomy is indicated are<br />
congenital malformations such as hemimegalencephaly, hemispheric<br />
or extensive multilobar cortical dysplasias, perinatal or<br />
acquired ischemic strokes, Sturge-Weber syndrome and Rasmussen<br />
syndrome. congenital malformations may occur as isolated<br />
disorders or in association with certain sporadic or inheritable<br />
genetic conditions. Figures 1 to 3 show brain MRI findings in<br />
children who are candidates for hemispherectomy.<br />
A thorough clinical evaluation — assessing age of seizure onset,<br />
course of the neurological symptoms, family history, presence of<br />
neurocutaneous markers, dysmorphic features or congenital<br />
anomalies involving multiple organ systems, and abnormal<br />
<strong>Pediatric</strong> ePilePsy<br />
Hemispheric Epilepsy and Hemispherectomy in Children<br />
Ajay Gupta, MD, and William E. Bingaman, MD<br />
Figure 1<br />
certain epilepsies are caused by congenital or acquired disorders that extensively involve all or most of one<br />
cerebral hemisphere. these disorders usually present with catastrophic epilepsy during infancy and require urgent<br />
diagnostic evaluation and treatment. After careful consideration of several complicating factors, hemispherectomy<br />
may be the most effective treatment for these children.<br />
Figure 2<br />
neurological findings — helps in making a specific diagnosis,<br />
determining disease progression and planning treatment. video<br />
eeg monitoring is the initial key tool in establishing the diagnosis<br />
of epilepsy, localizing the seizure-onset zone, and planning surgical<br />
strategy. Brain MRI, supplemented by FDG-PET, helps in determining<br />
the underlying epilepsy substrate and extent of hemispheric<br />
involvement as well as the anatomical and functional integrity of<br />
the unaffected hemisphere. other tests required may include an<br />
eye examination, neuropsychological assessment and metabolic/<br />
genetic consultation.<br />
timing and Planning of hemispherectomy<br />
hemispherectomy in children with catastrophic epilepsy is<br />
challenging and requires careful analysis of several complex<br />
age-related issues.<br />
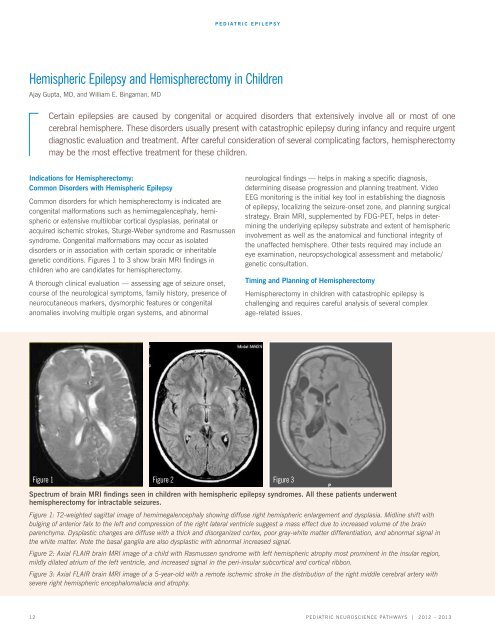
Spectrum of brain MRI findings seen in children with hemispheric epilepsy syndromes. All these patients underwent<br />
hemispherectomy for intractable seizures.<br />
Figure 1: T2-weighted sagittal image of hemimegalencephaly showing diffuse right hemispheric enlargement and dysplasia. Midline shift with<br />
bulging of anterior falx to the left and compression of the right lateral ventricle suggest a mass effect due to increased volume of the brain<br />
parenchyma. Dysplastic changes are diffuse with a thick and disorganized cortex, poor gray-white matter differentiation, and abnormal signal in<br />
the white matter. Note the basal ganglia are also dysplastic with abnormal increased signal.<br />
Figure 2: Axial FLAIR brain MRI image of a child with Rasmussen syndrome with left hemispheric atrophy most prominent in the insular region,<br />
mildly dilated atrium of the left ventricle, and increased signal in the peri-insular subcortical and cortical ribbon.<br />
Figure 3: Axial FLAIR brain MRI image of a 5-year-old with a remote ischemic stroke in the distribution of the right middle cerebral artery with<br />
severe right hemispheric encephalomalacia and atrophy.<br />
12 <strong>Pediatric</strong> NeuroscieNce <strong>Pathways</strong> | <strong>2012</strong> – 2013<br />
Figure 3














