

Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic
Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic
Pediatric Neuroscience Pathways Fall 2012 - Cleveland Clinic

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
MEG is a measure of the magnetic fields caused by neuronal<br />
activation. The instrument uses no X-ray radiation, generates no<br />
magnetic fields and requires no injections. The child simply lies<br />
quietly on a bed with his or her head resting in a special helmet.<br />
meg’s imaging capabilities offer a high spatial resolution along with<br />
a high temporal resolution — a combination that no other modality<br />
for studying the brain currently offers. The flow of electrical current<br />
through any conductor produces a magnetic field, which can then<br />
be recorded using sensitive magnetic sensors. Because the strength<br />
of the magnetic field produced by the brain is so small, very<br />
specialized instrumentation is required to pick up the signal. these<br />
sensing systems consist of small, high-resolution coils coupled to<br />
<strong>Pediatric</strong> ePilePsy<br />
Magnetoencephalography for Localization of Epileptogenic Sources in Children<br />
Patricia Klaas, PhD; Richard Burgess, MD, PhD; and John Mosher, PhD<br />
cleveland clinic began using magnetoencephalography (meg) in 2008 to aid in localizing epileptogenic sources.<br />
the procedure has been used with adults and children who have intractable epilepsy.<br />
Case Study: MEG Paves the Way for Successful Epilepsy Surgery<br />
A MEG was recorded at <strong>Cleveland</strong> <strong>Clinic</strong> of a 10-year-old boy with<br />
medically refractory epilepsy with daily seizures. video eeg evaluation<br />
suggested that the seizures arose from the left side of the brain<br />
but did not provide further localizing information. mri and neurological<br />
examination were normal. ictal sPect (single photon emission<br />
computed tomography) and interictal FDG-PET (fluorodeoxy-glucosepositron<br />
emission tomography) were not helpful.<br />
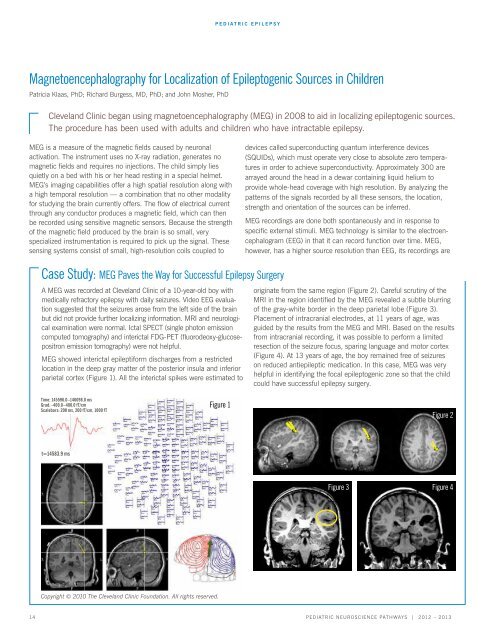
meg showed interictal epileptiform discharges from a restricted<br />
location in the deep gray matter of the posterior insula and inferior<br />
parietal cortex (Figure 1). all the interictal spikes were estimated to<br />
Time: 145596.0–146098.0 ms<br />
Grad: -400.0–400.0 fT/cm<br />
Scalebars: 200 ms, 200 fT/cm, 1000 fT<br />
t=14583.9 ms<br />
Copyright © 2010 The <strong>Cleveland</strong> <strong>Clinic</strong> Foundation. All rights reserved.<br />
Figure 1<br />
devices called superconducting quantum interference devices<br />
(SQUIDs), which must operate very close to absolute zero temperatures<br />
in order to achieve superconductivity. approximately 300 are<br />
arrayed around the head in a dewar containing liquid helium to<br />
provide whole-head coverage with high resolution. By analyzing the<br />
patterns of the signals recorded by all these sensors, the location,<br />
strength and orientation of the sources can be inferred.<br />
meg recordings are done both spontaneously and in response to<br />
specific external stimuli. MEG technology is similar to the electroencephalogram<br />
(EEG) in that it can record function over time. MEG,<br />
however, has a higher source resolution than EEG, its recordings are<br />
originate from the same region (Figure 2). careful scrutiny of the<br />
MRI in the region identified by the MEG revealed a subtle blurring<br />
of the gray-white border in the deep parietal lobe (Figure 3).<br />
Placement of intracranial electrodes, at 11 years of age, was<br />
guided by the results from the meg and mri. Based on the results<br />
from intracranial recording, it was possible to perform a limited<br />
resection of the seizure focus, sparing language and motor cortex<br />
(Figure 4). At 13 years of age, the boy remained free of seizures<br />
on reduced antiepileptic medication. In this case, MEG was very<br />
helpful in identifying the focal epileptogenic zone so that the child<br />
could have successful epilepsy surgery.<br />
14 <strong>Pediatric</strong> NeuroscieNce <strong>Pathways</strong> | <strong>2012</strong> – 2013<br />
Figure 2<br />
Figure 3 Figure 4














