Cystic neck masses: A pictorial review - Applied Radiology Online
Cystic neck masses: A pictorial review - Applied Radiology Online
Cystic neck masses: A pictorial review - Applied Radiology Online

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
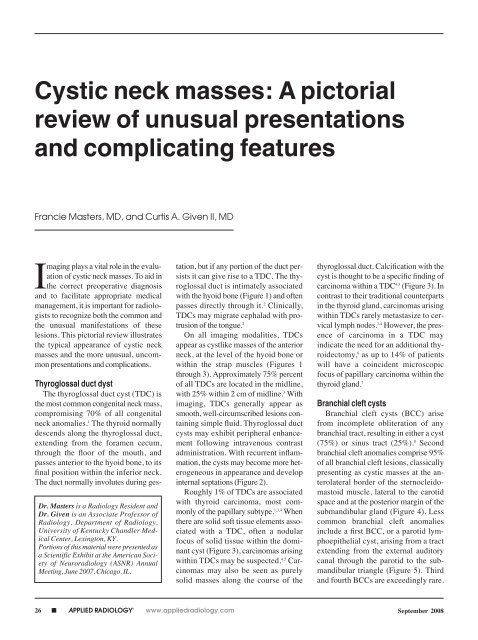
<strong>Cystic</strong> <strong>neck</strong> <strong>masses</strong>: A <strong>pictorial</strong><br />
<strong>review</strong> of unusual presentations<br />
and complicating features<br />
Francie Masters, MD, and Curtis A. Given II, MD<br />
Imaging plays a vital role in the evaluation<br />
of cystic <strong>neck</strong> <strong>masses</strong>. To aid in<br />
the correct preoperative diagnosis<br />
and to facilitate appropriate medical<br />
management, it is important for radiologists<br />
to recognize both the common and<br />
the unusual manifestations of these<br />
lesions. This <strong>pictorial</strong> <strong>review</strong> illustrates<br />
the typical appearance of cystic <strong>neck</strong><br />
<strong>masses</strong> and the more unusual, uncommon<br />
presentations and complications.<br />
Thyroglossal duct dyst<br />
The thyroglossal duct cyst (TDC) is<br />
the most common congenital <strong>neck</strong> mass,<br />
compromising 70% of all congenital<br />
<strong>neck</strong> anomalies. 1 The thyroid normally<br />
descends along the thyro glossal duct,<br />
extending from the foramen cecum,<br />
through the floor of the mouth, and<br />
passes anterior to the hyoid bone, to its<br />
final position within the inferior <strong>neck</strong>.<br />
The duct normally involutes during ges-<br />
Dr. Masters is a <strong>Radiology</strong> Resident and<br />
Dr. Given is an Associate Professor of<br />
<strong>Radiology</strong>, Department of <strong>Radiology</strong>,<br />
University of Kentucky Chandler Medical<br />
Center, Lexington, KY.<br />
Portions of this material were presented as<br />
a Scientific Exhibit at the American Society<br />
of Neuroradiology (ASNR) Annual<br />
Meeting, June 2007, Chicago, IL.<br />
26 ■ APPLIED RADIOLOGY ©<br />
tation, but if any portion of the duct persists<br />
it can give rise to a TDC. The thyroglossal<br />
duct is intimately associated<br />
with the hyoid bone (Figure 1) and often<br />
passes directly through it. 2 Clinically,<br />
TDCs may migrate cephalad with protrusion<br />
of the tongue. 2<br />
On all imaging modalities, TDCs<br />
appear as cystlike <strong>masses</strong> of the anterior<br />
<strong>neck</strong>, at the level of the hyoid bone or<br />
within the strap muscles (Figures 1<br />
through 3). Approximately 75% percent<br />
of all TDCs are located in the midline,<br />
with 25% within 2 cm of midline. 3 With<br />
imaging, TDCs generally appear as<br />
smooth, well-circumscribed lesions containing<br />
simple fluid. Thyroglossal duct<br />
cysts may exhibit peripheral enhancement<br />
following intravenous contrast<br />
administration. With recurrent inflammation,<br />
the cysts may become more heterogeneous<br />
in appearance and develop<br />
internal septations (Figure 2).<br />
Roughly 1% of TDCs are associated<br />
with thyroid carcinoma, most commonly<br />
of the papillary subtype. 1,3,4 When<br />
there are solid soft tissue elements associated<br />
with a TDC, often a nodular<br />
focus of solid tissue within the dominant<br />
cyst (Figure 3), carcinomas arising<br />
within TDCs may be suspected. 4,5 Carcinomas<br />
may also be seen as purely<br />
solid <strong>masses</strong> along the course of the<br />
thyroglossal duct. Calcification with the<br />
cyst is thought to be a specific finding of<br />
carcinoma within a TDC 4,5 (Figure 3). In<br />
contrast to their traditional counterparts<br />
in the thyroid gland, carcinomas arising<br />
within TDCs rarely metastasize to cervical<br />
lymph nodes. 1,4 However, the presence<br />
of carcinoma in a TDC may<br />
indicate the need for an additional thyroidectomy,<br />
6 as up to 14% of patients<br />
will have a coincident microscopic<br />
focus of papillary carcinoma within the<br />
thyroid gland. 7<br />
Branchial cleft cysts<br />
Branchial cleft cysts (BCC) arise<br />
from incomplete obliteration of any<br />
branchial tract, resulting in either a cyst<br />
(75%) or sinus tract (25%). 8 Second<br />
branchial cleft anomalies comprise 95%<br />
of all branchial cleft lesions, classically<br />
presenting as cystic <strong>masses</strong> at the anterolateral<br />
border of the sterno cleidomastoid<br />
muscle, lateral to the carotid<br />
space and at the posterior margin of the<br />
submandibular gland (Figure 4). Less<br />
common branchial cleft anomalies<br />
include a first BCC, or a parotid lymphoepithelial<br />
cyst, arising from a tract<br />
extending from the external auditory<br />
canal through the parotid to the submandibular<br />
triangle (Figure 5). Third<br />
and fourth BCCs are exceedingly rare.<br />
www.appliedradiology.com September 2008
A B<br />
September 2008<br />
CYSTIC NECK MASSES<br />
FIGURE 1. Thyroglossal duct cyst. (A and B) Axial contrast-enhanced CT images show a cystic mass (arrows) associated with the hyoid bone<br />
(arrowhead in A) and embedded with the strap muscles.<br />
A B<br />
FIGURE 2. Infected thyroglossal duct cyst. (A) A transverse sonographic image reveals a midline cystic <strong>neck</strong> mass with internal septations<br />
(arrows). (B) An axial contrast-enhanced CT image shows the mass embedded within the strap muscles and depicts surrounding inflammatory<br />
change (arrowheads).<br />
A B<br />
FIGURE 3. Papillary carcinoma arising within a thyroglossal duct cyst. (A) Axial and (B) sagittal<br />
reformatted enhanced CT images reveal a complex cystic anterior <strong>neck</strong> mass associated<br />
with the hyoid bone and embedded within the strap muscles. Within the cystic mass, there is a<br />
soft tissue nodule that contains small areas of calcification (arrows).<br />
FIGURE 4. Second branchial cleft cyst. This<br />
axial contrast-enhanced CT image shows a<br />
cystic mass (arrow) with a thin rim of en hance -<br />
ment displacing the submandibular gland<br />
(arrowhead) anteriorly and the sternocleidomastoid<br />
muscle posteriorly (asterisk).<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
■ 27
CYSTIC NECK MASSES<br />
A B<br />
FIGURE 5. First branchial cleft cyst. (A and B) Axial short tau inversion recovery MR images show a cystic lesion within the posterior aspects of<br />
the parotid gland (arrowheads) with a small fistulous tract extending toward the external auditory canal (arrow in A).<br />
FIGURE 6. Infected second branchial cleft cyst. This<br />
axial contrast-enhanced CT image shows a cystic mass<br />
(arrow) with a thin rim of enhancement displacing the<br />
submandibular gland anteriorly with surrounding inflammatory<br />
change (arrowheads).<br />
A B<br />
28 ■ APPLIED RADIOLOGY ©<br />
FIGURE 7. Presumed primary carcinoma arising within a second branchial cleft<br />
cyst. An axial contrast-enhanced CT image reveals a cystic mass posterior to the<br />
submandibular gland with eccentric enhancing soft tissue (arrow) along the posterior/medial<br />
wall. After a 13-month follow-up period, no additional malignancies or<br />
sites of tumor have been identified.<br />
FIGURE 8. Plunging ranula. Axial contrast-enhanced CT images show a cystic mass centered within the submandibular space. A characteristic<br />
“tail sign” is present (arrow in A), with tapering of the lesion anteriorly into the sublingual space.<br />
www.appliedradiology.com September 2008
CYSTIC NECK MASSES<br />
FIGURE 9. Dissecting ranula. (A and B) Axial short tau inversion recovery MR images show a<br />
cystic mass centered within the left sublingual space with a small component tapering anteriorly<br />
into the sublingual space (tail sign). The ranula has dissected across the midline into the<br />
left sublingual space (arrow in A).<br />
A<br />
B<br />
A B<br />
FIGURE 10. Infected ranula extending into the parapharyngeal space. (A) Serial axial and<br />
(B and C) oblique sagittal reformatted contrast-enhanced CT images show a cystic mass<br />
(arrows) within the left sublingual space extending posteriorly and superiorly through the parapharyngeal<br />
space. There is extensive inflammatory change and reactive lymphadenopathy.<br />
30 ■ APPLIED RADIOLOGY ©<br />
C<br />
FIGURE 11. <strong>Cystic</strong> hygroma. Axial (A) T1weighted<br />
and (B) short tau inversion recovery<br />
images show an infiltrative, multiseptated<br />
lesion throughout the deep fascial planes of<br />
the <strong>neck</strong>. (A) The variable signal seen on the<br />
T1-weighted image is indicative of prior hemorrhage.<br />
Third BCCs are posterior to the common<br />
or internal carotid artery and the sternocleidomastoid<br />
muscle, between the<br />
hypoglossal nerve below and the glossopharyngeal<br />
nerve above. 9 Fourth BCCs<br />
are generally sinus tracts or fistulas and<br />
arise from the pyriform sinus, pierce the<br />
thyrohyoid membrane, and descend<br />
along the tracheoesophageal groove.<br />
Branchial cleft cysts may become<br />
infected and exhibit thickening and<br />
enhancement of the cyst wall (Figure 6),<br />
mimicking a suppurative lymph node.<br />
www.appliedradiology.com September 2008<br />
A<br />
B
A B<br />
September 2008<br />
CYSTIC NECK MASSES<br />
FIGURE 12. Infected lymphangioma. (A and B) Axial contrast-enhanced CT images of the <strong>neck</strong> reveal an infiltrative, multilocular cystic lesion of the<br />
left posterior triangle. The significant surrounding edema and inflammatory change (arrows) indicate a superimposed infection.<br />
A B C<br />
FIGURE 14. Mixed laryngocele. This axial<br />
contrast-enhanced CT image shows a dilated,<br />
air-filled sac with a small air-fluid level. There<br />
is both a dilated internal component (saccule,<br />
arrowhead) and a dilated extralaryngeal component<br />
(arrow) extending through the thyrohyoid<br />
membrane.<br />
The existence of a primary carcinoma<br />
(Figure 7) arising within a BCC<br />
remains controversial. Most suspected<br />
cases are likely metastatic lesions from<br />
occult primaries. Imaging is generally<br />
insufficient to differentiate cystic nodal<br />
metastases from primary branchiogenic<br />
A<br />
carcinomas, with both exhibiting soft<br />
tissue components associated with a<br />
cystic lesion. Khafif 10 proposed that to<br />
make a diagnosis of a primary carci-<br />
FIGURE 13. Floor of mouth dermoid cyst. (A and B) Axial<br />
and (C) sagittal reformatted contrast-enhanced CT<br />
images reveal a cystic midline floor-of-mouth mass with<br />
several discrete foci of fat density (arrows) layering in the<br />
nondependent portion of the lesion, giving a “sac of marbles”<br />
appearance.<br />
FIGURE 15. Bilateral laryngoceles associated with laryngeal carcinoma. (A and B) Axial<br />
contrast-enhanced CT images show bilateral laryngoceles (mixed on the left side) associated<br />
with a bulky left-sided supraglottic squamous cell carcinoma (arrows in B).<br />
B<br />
noma within a BCC there must be no<br />
identifiable primary carcinoma elsewhere,<br />
and that the cystic lesion must<br />
show transition from normal epithelium<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
■ 31
CYSTIC NECK MASSES<br />
A B<br />
FIGURE 16. Laryngopyocele. (A) Serial axial and (B) coronal reformatted contrast-enhanced CT images of the <strong>neck</strong> show a large cystic mass<br />
(arrowheads) with an irregular rim of enhancement and surrounding inflammatory change. The mass is centered within the paraglottic space,<br />
with extra laryngeal extension through the thryohyoid membrane. A small “<strong>neck</strong>” of the lesion that can be seen coursing through the paraglottic<br />
fat represents the nondilated saccule (arrows).<br />
A B<br />
FIGURE 17. Thymic cyst. (A) Axial and (B) coronal reformatted noncontrastenhanced<br />
CT images of the <strong>neck</strong> show a large cystic mass (arrows) that is posterior<br />
to the sternocleidomastoid muscle and extends from the left anterior <strong>neck</strong> into<br />
the upper mediastinum. There is mass effect and displacement of the airway.<br />
to invasive carcinoma (transitional zone)<br />
on cytopathologic analysis.<br />
Ranulas<br />
Ranulas represent cystic lesions of the<br />
floor of mouth, usually occurring secondary<br />
to obstruction of the sublingual<br />
duct. Ranulas are classified as either<br />
“simple” and confined to the sublingual<br />
32 ■ APPLIED RADIOLOGY ©<br />
space, or as “plunging” with extension<br />
through the floor of mouth and below the<br />
mylohyoid muscle. The plunging variety<br />
presents as a cystic mass centered within<br />
the submandibular space (Figure 8).<br />
Rarely, ranulas can dissect across the<br />
midline between the mylohyoid and<br />
geniohyoid muscles to present as a bilateral<br />
mass (Figure 9). Ranulas may<br />
become infected and demonstrate a<br />
thick, irregular rim of enhancement<br />
with surrounding inflammatory change<br />
(Figure 10). Because of the lack of a fascial<br />
boundary between the sublingual/<br />
submandibular and the parapharyngeal<br />
spaces, plunging ranulas may uncommonly<br />
extend into the parapharyngeal<br />
space 11 (Figure 10).<br />
www.appliedradiology.com September 2008
CYSTIC NECK MASSES<br />
<strong>Cystic</strong> hygroma<br />
<strong>Cystic</strong> hygromas represent the most<br />
common form of a lymphangioma.<br />
These lesions are thought to arise from<br />
an early sequestration of embryonic<br />
lymphatic channels, 12 most commonly<br />
occurring along the developing jugular<br />
chain. <strong>Cystic</strong> hygromas typically appear<br />
as a multilocular cystic mass with septations<br />
of variable thickness, usually centered<br />
in the posterior triangle or submandibular<br />
space. These lesions are<br />
characteristically infiltrative in nature<br />
and do not respect fascial planes (Figure<br />
11). Fluid-fluid levels may be present<br />
when the lesions are complicated by<br />
hemorrhage, and large lesions may cross<br />
the midline (Figure 11). <strong>Cystic</strong> hygromas<br />
may become infected and increase<br />
in size (Figure 12).<br />
Dermoid and epidermoid cysts<br />
Dermoid and epidermoid cysts may<br />
occur anywhere in the body, with 7% presenting<br />
as head and <strong>neck</strong> lesions, most<br />
commonly lateral to the eyebrow. 9 Approximately<br />
11% of the head and <strong>neck</strong><br />
lesions are located within the floor of the<br />
mouth. 9 The floor-of-the-mouth lesions<br />
typically present as thin-walled, unilocular<br />
<strong>masses</strong> located in the submandibular<br />
or sublingual space. There may be coalescence<br />
of fat into small nodules within the<br />
cystic lesion, giving a “sac-of-marbles”<br />
appearance (Figure 13). The rim of the<br />
cyst may show contrast enhancement. It<br />
has been noted that 5% of lesions may<br />
undergo malignant degeneration into<br />
squamous cell carcinomas. 13<br />
Laryngocele<br />
The laryngeal ventricle is a slitlike<br />
cavity, with the orifice located between<br />
the true and false cords. A laryngocele<br />
is dilatation of the laryngeal saccule, a<br />
small pouch arising from the roof of<br />
the ventricle. 14 Laryngoceles confined<br />
to the larynx are known as internal<br />
34 ■ APPLIED RADIOLOGY ©<br />
laryngoceles. Those that extend through<br />
the thyrohyoid membrane, but with dilation<br />
of only the extralaryngeal component<br />
are termed external. Mixed<br />
laryngoceles have dilatation of the saccule<br />
on both sides of the thyro hyoid<br />
membrane (Figure 14).<br />
Laryngoceles generally present as<br />
round or oval lesions within the superior<br />
paralaryngeal space (Figure 14) and<br />
may have an extralaryngeal component<br />
(external and mixed). The laryngocele<br />
may be completely air-filled, fluid-filled,<br />
or have an air-fluid level (Figure 14).<br />
Fifteen percent of laryngoceles are associated<br />
with carcinoma, 15 with tumor<br />
occluding the orifice of the laryngeal<br />
ventricle (Figure 15). The presence of<br />
soft tissue within a laryngocele suggests<br />
an underlying neoplasm. In as many as<br />
8% to 10% of cases, 16 a laryngocele may<br />
become infected, called a laryngopyocele<br />
(Figure 16).<br />
Thymic cyst<br />
Thymic cysts have a disputed etiology,<br />
but most favor the theory that these<br />
lesions arise from persistence of the thymo<br />
pharyngeal duct, 17 adjacent to the<br />
carotid sheath from the angle of the<br />
mandible to the thoracic inlet. 18 The<br />
cysts arise from the third and fourth<br />
branchial clefts, and, therefore, thymic<br />
cysts may have a similar appearance to<br />
third and fourth branchial cleft cysts,<br />
being differentiated only by the presence<br />
of thymic tissue within thymic cysts.<br />
The cysts usually present as a unilocular<br />
cystic mass extending inferiorly within<br />
the <strong>neck</strong>, paralleling the sternocleidomastoid<br />
muscle (Figure 17). There are<br />
no reports of myasthenia gravis or neoplasia<br />
associated with thymic cysts. 9<br />
Conclusion<br />
Patients with palpable <strong>neck</strong> <strong>masses</strong> are<br />
frequently sent for evaluation with crosssection<br />
imaging both for diagnosis and for<br />
www.appliedradiology.com<br />
planning biopsy or surgical resection. It is<br />
important for radiologists to not only recognize<br />
the common appearance of cystic<br />
<strong>neck</strong> <strong>masses</strong>, but to appreciate the more<br />
unusual manifestations of such <strong>masses</strong><br />
and potential complications that may alter<br />
therapy or surgical management.<br />
REFERENCES<br />
1. Allard RH. The thyroglossal cyst. Head Neck<br />
Surg. 1982;5:134-146.<br />
2. Filston HC. Common lumps and bumps of the<br />
head and <strong>neck</strong> in infants and children. Pediatr<br />
Ann. 1989;18:180-186.<br />
3. Telander RL, Filston HC. Review of head and<br />
<strong>neck</strong> lesions in infancy and childhood. Surg Clin<br />
North Am. 1992;72:1429-1447.<br />
4. Fernandez JF, Ordonez NG, Schultz PN, et al.<br />
Thyroglossal duct carcinoma. Surgery. 1991;110:<br />
928-934; discussion 934-935.<br />
5. Glastonbury CM, Davidson HC, Haller JR,<br />
Harnsberger HR. The CT and MRI imaging feature<br />
of carcinoma arising in thyroglossal duct remnants.<br />
AJNR Am J Neuroradiol. 2000;21:770-774.<br />
6. Kennedy TL, Whitaker M, Wadih G. Thyroglossal<br />
duct carcinoma: A rational approach to management.<br />
Laryngoscope. 1998;108(8 Pt 1):1154-1158.<br />
7. Wexler MJ. Surgical management of the thyroglossal<br />
duct carcinoma: Is an aggressive approach<br />
justified? Can J Surg. 1996;39:263-264.<br />
8. Deane SA, Telander RL. Surgery for thyroglossal<br />
duct and branchial cleft anomalies. Am J Surg.<br />
1978136:348-353.<br />
9. Koeller KK, Alamo L, Adair CF, Smirniotopoulos<br />
JG. Congenital cystic <strong>masses</strong> of the <strong>neck</strong>: Radiologicpathologic<br />
correlation. RadioGraphics. 1999; 19:<br />
121-146; quiz 152-153. Erratum in: Radio Graphics.<br />
1999;19:282.<br />
10. Khafif RA, Prichep R, Minkowitz S. Primary<br />
branchiogenic carcinoma. Head Neck. 1989;11:<br />
153-163.<br />
11. Kurabayashi T, Ida M, Yasumoto M, et al. MRI<br />
of rannulas. Neuroradiology. 2000;42:917-922.<br />
12. Smith D. Recognizable Patterns of Human<br />
Malformation: Genetic, Embryologic, and Clinical<br />
Aspects, 3rd ed. Philadelphia, PA: WB Saunders;<br />
1982:472-473.<br />
13. Som P. <strong>Cystic</strong> lesions of the <strong>neck</strong>. Postgrad<br />
Radiol. 1987;7:211-236.<br />
14. Delahunty JE, Cherry J. The laryngeal saccule.<br />
J Laryngol Otol. 1969;83:803-815.<br />
15. Canalis RF, Maxwell DS, Hemenway WG.<br />
Laryngocele—An updated <strong>review</strong>. J Otolaryngol.<br />
1977;6:191-199.<br />
16. Stell PM, Maran AG. Laryngocoele. J Laryngol<br />
Otol. 1975;89:915-924.<br />
17. Zarbo RJ, McClatchey KD, Areen RG, Baker SB.<br />
Thymopharyngeal duct cyst: A form of cervical thymus.<br />
Ann Otol Rhinol Laryngol. 1983;92:284-289.<br />
18. Mikal S. Cervical thymic cyst. Case report and<br />
<strong>review</strong> of the literature. Arch Surg. 1974;109:558-562.<br />
September 2008