Download PDF - Applied Radiology Online
Download PDF - Applied Radiology Online
Download PDF - Applied Radiology Online

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Compression elasticity imaging of<br />
the breast: An overview<br />
Joseph R. Grajo, MD, and Richard G. Barr, MD, PhD<br />
One out of every 8 women will<br />
develop breast cancer during<br />
their lifetime. Currently, the<br />
best method of treating breast cancer involves<br />
early detection. Physicians have<br />
used palpation for many years as a way<br />
to detect lumps or nodules in the female<br />
breast. In fact, regular breast self-examinations<br />
(BSE) and clinical breast examinations<br />
(CBE) have long been used<br />
to detect breast nodules in their earliest<br />
stages of development. Although the<br />
effects of BSE on mortality rates from<br />
breast cancer are debatable, CBE still<br />
exists as a standard screening protocol<br />
for breast cancer in women. As an adjunct<br />
to direct manual palpation, physicians<br />
have utilized ultrasonography to<br />
visualize lesions in breast tissue. Lesion<br />
features are frequently characterized<br />
based on shape, echogenicity, shadowing,<br />
margin irregularity, and microlobulation.<br />
1-3 Ultrasound has been extremely<br />
important because of its ability to help<br />
differentiate cystic breast lesions from<br />
solid lesions. This provides the clinician<br />
with useful insight into the possible benignity<br />
or malignancy of a given lesion.<br />
Dr. Grajo is a Diagnostic <strong>Radiology</strong> Resident<br />
at the University of South Florida,<br />
Tampa, FL, and Dr. Barr is a Radiologist<br />
at Southwoods <strong>Radiology</strong>, <strong>Radiology</strong><br />
Consultants Inc., Youngstown, OH.<br />
18 n APPLIED RADIOLOGY ©<br />
Over the past two decades, various<br />
new methods have been developed to<br />
sonographically evaluate the stiffness<br />
of a lesion. 4-11 These methods offer<br />
the potential to quantify the formerly<br />
qualitative-only measurement of tissue<br />
stiffness; therefore, allowing for<br />
increased differentiation of cystic and<br />
solid breast lesions. With the use of<br />
standard ultrasound equipment and<br />
new “elasticity imaging” (EI) software,<br />
the trained clinician can now noninvasively<br />
differentiate benign and malignant<br />
breast lesions with high sensitivity<br />
and specificity. Although the standard<br />
of care for the diagnosis of breast cancer<br />
still involves biopsy, elastography<br />
has the potential to significantly reduce<br />
the number of biopsies of benign breast<br />
lesions. 12,13 This would help to alleviate<br />
anxiety in many patients and to decrease<br />
the related high healthcare costs<br />
in the United States (U.S.). This article<br />
will review the physics behind the elastographic<br />
technique, the utility of elasticity<br />
imaging in clinical practice, the<br />
implications of EI on patient care, and<br />
possible advances in elastography in the<br />
near future.<br />
Defining the technique<br />
Elasticity imaging, also referred to as<br />
elastography, offers great potential to<br />
characterize cystic and solid breast le-<br />
sions using a combination of standard<br />
ultrasound imaging and innovative<br />
software technology. There are 2 main<br />
categories of elasticity imaging: compression,<br />
or “strain,” elastography, and<br />
shear wave elastography. Strain elastography<br />
is a qualitative method that<br />
measures stiffness based on soft-tissue<br />
distortion caused by minimal manual<br />
compression. Conversely, shear wave<br />
elastography is a quantitative method<br />
that relies on the principles of Young’s<br />
modulus to measure the speed of lowfrequency<br />
shear wave transmission<br />
through soft tissue. In the authors’ lab,<br />
minimal manual compression is utilized,<br />
usually provided by the patient’s<br />
respiratory cycle and cardiac rebound,<br />
to produce strain images. This article<br />
describes this method.<br />
Like conventional B-mode sonographic<br />
imaging, EI differentiates cystic<br />
breast lesions from solid breast lesions.<br />
An artifact that occurs with some manufacturers’<br />
equipment has been reported<br />
to characterize cystic lesions with high<br />
accuracy. The technology can also<br />
further characterize solid lesions that<br />
contain both benign and malignant elements.<br />
In such cases, the clinician can<br />
aspirate or biopsy the various elements<br />
in a lesion with the guidance of the<br />
elasticity software. This allows for obtaining<br />
appropriate breast tissue more<br />
www.appliedradiology.com October 2012
A B<br />
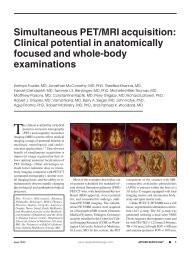
FIGURE 1. Real-time display. In our center, we display both the (A) B-mode image and the (B)<br />
strain image, or elastogram, side-by-side in real time. The strain image demonstrates “soft”<br />
areas as bright and “hard” areas as dark. The lesion is hypoechoic on B-mode but appears<br />
bright on the strain image, indicating that the lesion is “soft.” This lesion was biopsied and<br />
found to be a fat lobule.<br />
accurately and helps to provide the pathologist<br />
with information regarding<br />
the likely composition of the specimen.<br />
Besides characterizing the composition<br />
of breast lesions, EI offers the potential<br />
to differentiate benign lesions<br />
from malignant with high sensitivity and<br />
specificity. The technique is based on the<br />
differing physical properties of benign<br />
and malignant lesions, as described by<br />
clinicians throughout the literature. It has<br />
long been reported that benign lesions<br />
tend to be “softer,” with more mobility<br />
within the breast parenchyma, while malignant<br />
lesions tend to be “harder,” with<br />
a propensity for remaining firmly fixed<br />
within the tissue. 14,15 The theory behind<br />
elastography is that cancerous and noncancerous<br />
lesions will demonstrate differing<br />
amounts of tissue motion relative<br />
to the normal surrounding breast parenchyma<br />
when minimal pressure is applied.<br />
The ability to differentiate soft and<br />
hard lesions allows the clinician to utilize<br />
EI to predict the benignity or malignancy<br />
of breast lesions. This would potentially<br />
lead to a significant decrease in the number<br />
of benign breast biopsies and, therefore,<br />
reduce the overall cost of care.<br />
The physics of elastography<br />
Compression EI is performed with<br />
a standard high-frequency ultrasound<br />
probe. The returning radiofrequency<br />
signals are analyzed in real time with<br />
the standard B-mode algorithm and the<br />
October 2012<br />
COMPRESSION ELASTICITY IMAGING OF THE BREAST<br />
EI algorithm. The EI algorithm analyzes<br />
the stiffness of a lesion compared<br />
to the compressibility of its surrounding<br />
tissue, much like measuring the degree<br />
of stiffness of a marble suspended<br />
within a bowl of gelatin. In this model,<br />
external compression will cause the<br />
gelatin, and not the marble, to change<br />
shape. The computer analyzes this degree<br />
of deformation to determine if the<br />
lesion is soft or hard. Both the standard<br />
B-mode image and the EI image are<br />
displayed in real time. The EI algorithm<br />
is sensitive for a 0.1% strain and<br />
uses temporal persistency strategy to<br />
enhance the descriptive pattern in the<br />
elastogram. Using this technique in the<br />
breast, the elastography contrast for<br />
cancerous and noncancerous lesions<br />
is between 1000% and 5000%, as opposed<br />
to the tissue contrast of 1% to<br />
100% between cancerous and noncancerous<br />
lesions using conventional imaging<br />
techniques, such as ultrasound,<br />
mammography, and magnetic resonance<br />
imaging (MRI). 16 Motion is provided<br />
by patient breathing and cardiac<br />
rebound. If additional compression is<br />
required, slow minimal palpation with<br />
the probe can be applied. In patients<br />
with small breasts, the patient may have<br />
to hold her breath to limit motion. The<br />
sonographer must ensure that the lesion<br />
remains in the image plane during<br />
the compression cycle. It is important to<br />
have the probe and lesion perpendicular<br />
to the scanning table. We record a short<br />
clip that demonstrates both the compression<br />
and release stages. The best<br />
image is selected by cine review for<br />
subsequent measurements.<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
A<br />
B<br />
C<br />
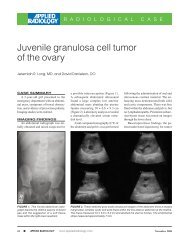
FIGURE 2. Benign fibroadenoma in an<br />
18-year-old woman with a palpable breast<br />
mass. The patient had had no previous<br />
mammograms. (A) B-mode imaging reveals<br />
a hypoechoic lesion with low-level internal<br />
echoes and (B) peripheral color flow. Measurements<br />
of lesion length demonstrated<br />
a smaller dimension on the elastogram.<br />
Based on the B-mode findings, this lesion<br />
was classified as BIRADS 4B; pathology<br />
revealed it to be a benign fibroadenoma.<br />
n 19
COMPRESSION ELASTICITY IMAGING OF THE BREAST<br />
A B<br />
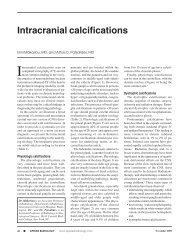
FIGURE 3. Fibroadenoma in a 42-year-old woman with dense breasts. (A) B-mode imaging<br />
revealed a hypoechoic lesion with some low-level internal echoes and no posterior acoustic<br />
enhancement. (B) The lesion appears smaller on real-time compression elasticity imaging.<br />
Based on B-mode, this lesion was characterized as BIRADS 4. This lesion was proven at<br />
biopsy to be a fibroadenoma.<br />
A B<br />
FIGURE 4. Fibrocystic change in a 72-year-old woman with an asymmetric density on mammography.<br />
(A) B-mode imaging demonstrates a mostly hypoechoic lesion with posterior acoustic<br />
enhancement. An additional lobulated hypoechoic area is seen adjacent to this lesion. (B)<br />
On elastography, the lesion appears smaller with a central bright spot surrounded by darker<br />
areas. This lesion was biopsied and was consistent with apocrine metaplasia.<br />
A B<br />
FIGURE 5. Simple cyst. (A) B-mode imaging demonstrates a simple cyst. (B) A manufacturer’s<br />
artifact on the strain image shows a dark lesion with bright spots centrally and posteriorly.<br />
This “bull’s-eye” artifact appears in both simple and complicated cysts.<br />
20 n APPLIED RADIOLOGY ©<br />
While performing an ultrasound on<br />
a patient with a known breast lesion(s),<br />
both the standard B-mode image and<br />
the elastogram are displayed side-byside<br />
(Figure 1). We can then directly<br />
compare the relative stiffness of a lesion<br />
based on its elastic properties in relation<br />
to the surrounding tissue. In our study,<br />
we set the ultrasound machine to display<br />
“soft lesions” as white and “hard<br />
lesions” as black. This gives us immediate<br />
insight into the relative stiffness<br />
of any lesion within the breast parenchyma.<br />
It is important to emphasize that<br />
the elastographic technique provides the<br />
clinician only with the relative stiffness<br />
of breast lesions within the surrounding<br />
tissue. Therefore, lesions will exhibit<br />
varying shades of gray in fatty breast<br />
tissue as opposed to dense breast tissue.<br />
To obtain an appropriate dynamic range<br />
for interpretation, we try to include<br />
fatty tissue, normal dense breast tissue,<br />
and the lesion in the field of view. This<br />
limits our ability to utilize EI in a mass<br />
screening protocol.<br />
By displaying the B-mode sonographic<br />
image and the elastogram sideby-side,<br />
we can also directly compare<br />
the relative dimensions of the lesions<br />
in both image displays. We then predict<br />
the benignity or malignancy of the<br />
breast lesion based on size of the lesion<br />
in the elasticity image compared<br />
to its size in the B-mode display. Either<br />
length or area of the lesion in the greatest<br />
dimension can be utilized to measure<br />
the magnitude of the lesion. If the<br />
lesion appears smaller on the elastogram<br />
based on direct measurement, it<br />
is characterized as benign. If the lesion<br />
measures equally or larger on the elastogram<br />
compared to the B-mode image,<br />
the lesion is deemed to be malignant. In<br />
our initial study, we determined that EI<br />
is able to correctly differentiate benign<br />
and malignant breast lesions with very<br />
high sensitivity and specificity. 17-19<br />
Clinical utility of breast<br />
elasticity imaging<br />
Elasticity imaging offers the potential<br />
to characterize various breast lesions<br />
in great detail and to provide the<br />
www.appliedradiology.com October 2012
A B<br />
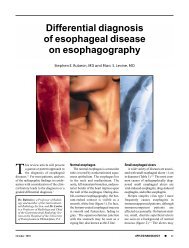
FIGURE 6. Recurrent invasive ductal carcinoma (IDC) in a 52-year-old woman with history<br />
of left breast lumpectomy for IDC. The patient presented with a new mass at the edge of her<br />
surgical scar. (A) B-mode imaging demonstrates a mostly hypoechoic lesion with some posterior<br />
acoustic enhancement. (B) Real-time strain imaging shows a uniformly dark lesion, which<br />
appears larger on the elastogram.<br />
A<br />
FIGURE 7. Invasive ductal carcinoma in a 50-year-old woman. (A) On B-mode imaging, the<br />
lesion appeared suspicious and was classified as BIRADS 5, requiring biopsy. (B) The lesion<br />
appeared noticeably larger on elastography, even with the naked eye.<br />
A<br />
FIGURE 8. Lobular carcinoma in situ. Sonography was performed on this 74-year-old woman<br />
with a palpable lump in the left breast. (A) B-mode imaging shows a hypoechoic mass with<br />
ill-defined borders. (B) Compression elastography demonstrates a mostly dark structure that<br />
appears larger on the strain image relative to the B-mode image. This suspicious lesion was<br />
biopsied and found to be a lobular carcinoma in situ (LCIS).<br />
October 2012<br />
B<br />
B<br />
COMPRESSION ELASTICITY IMAGING OF THE BREAST<br />
sonographer with an extremely helpful<br />
adjunct to the standard ultrasound examination.<br />
The elastographic technique<br />
is entirely noninvasive and adds only a<br />
few minutes to the conventional sonographic<br />
exam. It augments the value of<br />
the sonogram and allows for immediate<br />
interpretation of results. In addition,<br />
elastography provides the clinician with<br />
detailed characterization of the cystic or<br />
solid breast lesion that may not be readily<br />
appreciated on B-mode imaging.<br />
For example, lesions that appear to be<br />
solid on B-mode imaging may actually<br />
be complicated cysts when imaged with<br />
elastographic software. In the authors’<br />
clinical study, 4% of all lesions that appeared<br />
solid on B-mode were actually<br />
complicated cysts when viewed as a<br />
strain image. 20 These lesions can be easily<br />
aspirated, negating the need for subsequent<br />
biopsy.<br />
The clinician can rapidly predict the<br />
benignity or malignancy of breast lesions<br />
with EI software and standard B-mode<br />
imaging techniques. In the authors’ clinical<br />
study, the size of the breast lesion on<br />
the B-mode and the elasticity image was<br />
directly compared. The lesion was determined<br />
as likely to be benign or malignant<br />
based on the ratio of the lesion’s size on<br />
the strain image compared to its size on Bmode<br />
image. If the ratio is
COMPRESSION ELASTICITY IMAGING OF THE BREAST<br />
on a large-scale, multicenter basis, it is<br />
hoped, then the initial determination<br />
of a breast lesion’s nature can lead to a<br />
decrease in the number of benign breast<br />
biopsies.<br />
Appearance of benign lesions<br />
In our experience with EI, benign<br />
lesions appear smaller on strain images<br />
compared to the corresponding<br />
B-mode image (Figures 2 and 3). This<br />
is based on the relative elasticity of a<br />
breast lesion within its surrounding<br />
parenchyma. If a lesion demonstrates<br />
stiffness similar to normal dense breast<br />
tissue, it is more likely to be benign<br />
(Figure 4). In our lab, we also display<br />
soft structures as white, which further<br />
demarcates areas of increased elasticity.<br />
Of particular interest is the easy identification<br />
of both simple and complicated<br />
cysts with compression elastography.<br />
We have shown that cystic lesions demonstrate<br />
a “bull’s-eye” artifact, featuring<br />
a dark structure with both central<br />
and posterior bright foci (Figure 5). 21<br />
The identification of lesions as benign<br />
cystic lesions on elastography can lead<br />
to direct aspiration of symptomatic lesions<br />
and avoidance of biopsy for complicated<br />
cysts, which may otherwise<br />
appear suspicious on standard B-mode<br />
imaging. In lesions with both cystic and<br />
solid components, elasticity can help<br />
guide biopsy to obtain the most useful<br />
specimen.<br />
Appearance of malignant lesions<br />
Due to their increased stiffness, malignant<br />
lesions appear the same or larger<br />
on the elastogram when compared to<br />
the B-mode image. In our center, these<br />
malignant lesions appear dark on the<br />
strain images and may demonstrate<br />
adjacent areas of tissue invasion that<br />
would not be appreciated on B-mode.<br />
In the authors’ experience, we can predict<br />
malignancy based on the real-time<br />
elastogram with high confidence. Furthermore,<br />
a recent retrospective review<br />
has shown the potential to determine<br />
the aggressiveness of malignant lesions<br />
and predict the grade of these<br />
tumors via EI. Limited data analysis<br />
22 n APPLIED RADIOLOGY ©<br />
has demonstrated that more aggressive<br />
malignancies, such as invasive ductal<br />
carcinomas (Figures 6 and 7) and invasive<br />
lobular carcinomas (Figure 8),<br />
will exhibit higher elasticity/B-mode<br />
(E/B) ratios compared to mucinous<br />
carcinomas or ductal carcinoma in situ<br />
(DCIS), for example. Moreover, initial<br />
results demonstrate that higher grades<br />
of IDC correlate with higher E/B ratios<br />
in a statistically significant fashion. 22<br />
This observation could have important<br />
implications for the radiologist’s ability<br />
to characterize breast lesions, such as in<br />
classification according to the BIRADS<br />
system. With the use of elastography,<br />
one may be able to downgrade or upgrade<br />
BIRADS 3 and 4A lesions. Further<br />
validation and standardization of<br />
this technique is required.<br />
Conclusion<br />
Elasticity imaging has demonstrated<br />
the ability to differentiate benign and<br />
malignant breast lesions with high<br />
sensitivity and specificity. Numerous<br />
imagers have utilized various forms of<br />
the elastographic technique, including<br />
color elastography, strain ratio measurements,<br />
and, most recently, shear<br />
wave technology, to characterize an<br />
array of breast lesions. In our practice,<br />
the authors have produced very favorable<br />
results with compression elasticity<br />
images utilizing simple cardiac and<br />
respiratory cycles to provide the appropriate<br />
degree of compression for the<br />
production of strain images. The appropriate<br />
degree of compression is, in fact,<br />
a critical aspect of reproducing these<br />
favorable results. Applying excessive<br />
manual compression to breast tissue<br />
will compact the parenchyma and make<br />
fat appear harder, skewing the interpretation<br />
of the strain image. The concept<br />
of applying only minimal compression,<br />
termed “pre-compression,” is of vital<br />
importance in obtaining accurate and<br />
reproducible strain images.<br />
EI can be particularly helpful when<br />
working up complicated breast lesions.<br />
Some lesions may contain both benign<br />
and malignant-appearing components,<br />
making it difficult to decide where to<br />
biopsy within the lesion. Because of the<br />
distinction between “soft” and “hard”<br />
lesions provided by elastography, the<br />
clinician can direct the biopsy needle to<br />
the more suspicious components within<br />
a particular breast lesion. The hard component<br />
of the lesion can be biopsied,<br />
while the soft component can be aspirated<br />
with FNA. This will subsequently<br />
lead to direct needle placement and increased<br />
biopsy accuracy. It will also<br />
enhance pathologic diagnosis, as the radiologist<br />
can provide the pathology lab<br />
with more detailed information along<br />
with the specimen itself.<br />
Over the last several years, we have<br />
conducted both single-center and multicenter<br />
trials to demonstrate the effectiveness<br />
of compression elasticity<br />
imaging in differentiating benign and<br />
malignant breast lesions. With strain<br />
elastography, it is often difficult to interpret<br />
the elastogram in cases where a<br />
benign lesion (eg, fibroadenoma, fibrocystic<br />
change) lies within a background<br />
of dense breast tissue. The elastographic<br />
properties are similar and it is<br />
difficult to determine the boundaries of<br />
the lesion. Shear wave imaging will be<br />
helpful in these cases. We believe that<br />
strain elastography can have several implications<br />
for the future of breast imaging.<br />
These include a decrease in number<br />
of benign biopsies, a reduction in the<br />
costs of lesion work-up, incorporation<br />
into the BIRADS classification system,<br />
and possibly the prediction of breast<br />
cancer grade. Additionally, the elastographic<br />
technique can help direct needle<br />
biopsy and provide useful diagnostic information<br />
to the pathologist. As such,<br />
EI may prove to be an important adjunct<br />
to standard B-mode sonography in the<br />
evaluation of a breast lesion.<br />
references<br />
1. Stavros AT, Thickman D, Rapp CL, et al. Solid<br />
breast nodules: Use of sonography to distinguish<br />
between benign and malignant lesions. <strong>Radiology</strong>.<br />
1995;196:123-134.<br />
2. Velez N, Earnest DE, Staren ED. Diagnostic<br />
and interventional ultrasound for breast disease.<br />
Am J Surg. 2000;180:284-287.<br />
3. Dennis MA, Parker SH, Klaus AJ, et al. Breast<br />
biopsy avoidance: The value of normal mammograms<br />
and normal sonograms in the setting of a<br />
palpable lump. <strong>Radiology</strong>. 2001;219:186-191.<br />
www.appliedradiology.com October 2012
4. Chaturvedi P, Insana MF, Hall TJ. Ultrasonic<br />
and elasticity imaging to model disease-induced<br />
changes in soft-tissue structure. Med Image Anal.<br />
1998;2:325-338.<br />
5. Garra BS, Cespedes EI, Ophir J, et al. Elastography<br />
of breast lesions: Initial clinical results. <strong>Radiology</strong>.<br />
1997;202:79-86.<br />
6. Ophir J, Cespedes I, Ponnekanti H, et al. Elastography:<br />
A quantitative method for imaging the<br />
elasticity of biological tissues. Ultrason Imaging.<br />
1991;13:111-134.<br />
7. Lubinski MA, Emelianov Y, O’Donnell M. Adaptive<br />
strain estimation using retrospective processing.<br />
IEEE Trans Ultrason Ferroelect Freq Control.<br />
1999;46:97-107.<br />
8. Skovoroda AR, Emelianov Y, O’Donnell M. Tissue<br />
elasticity reconstruction based on ultrasonic<br />
displacement and strain images. IEEE Trans Ultrason<br />
Ferroelect Freq Control. 1995;42:747-765.<br />
9. Parker KJ, Fu D, Graceswki SM, et al. Vibration<br />
sonoelastography and the detectability of lesions.<br />
Ultrasound Med Biol. 1998;24:1437-1447.<br />
10. Taylor LS, Porter BC, Rubens DJ, Parker KJ.<br />
Three-dimensional sonoelastography: Principles<br />
and practices. Phys Med Biol. 2000;45:1477-1494.<br />
October 2012<br />
COMPRESSION ELASTICITY IMAGING OF THE BREAST<br />
11. Hall TJ, Zhu Y, Spalding CS, Cook LT. In vivo<br />
results of real-time freehand elasticity imaging. In:<br />
Ultrasonics Symposium. 2001;1653-1657.<br />
12. Liberman L, Feng TL, Dershaw DD, et al. USguided<br />
core breast biopsy: Use and cost-effectiveness.<br />
<strong>Radiology</strong>. 1998;208:717-723.<br />
13. Svensson WE et al. Elasticity imaging of 67<br />
cancers and 167 benign breast lesions shows that<br />
it could halve biopsy rates of benign lesions. Proceedings<br />
of the 4th International Conference on<br />
the Measurement and Imaging of Tissue Elasticity.<br />
2005:87.<br />
14. Emerson K. Diseases of the Breast. In: Wintrobe<br />
MM, Harrison TR, eds. Harrison’s Principles<br />
of Internal Medicine. Harrison’s Principles of Internal<br />
Medicine, 7th ed. New York: McGraw-Hill;<br />
1974:582-587.<br />
15. Pruthi S. Detection and evaluation of a palpable<br />
breast mass. Mayo Clin Proc. 2001;76:641-647.<br />
16. Krouskop TA, Wheeler TM, Kallel F, et al.<br />
Elastic moduli of breast and prostate tissue<br />
under compression. Ultrason Imaging. 1998;20:<br />
260-274.<br />
17. Barr RG. Initial results of real-time elasticity<br />
of the breast. Proceedings of the Radiological<br />
Society of North America, 92nd Scientific Assembly<br />
and Annual Meeting. 2006.<br />
18. Barr RG, Grajo JR. Initial results of real-time<br />
elasticity imaging in the evaluation of breast<br />
lesions. Proceedings of the Sixth International<br />
Conference on the Ultrasonic Measurement and<br />
Imaging of Tissue Elasticity. 2007.<br />
19. Grajo JR, Barr RG. Elasticity imaging of the<br />
breast: A clinical perspective. Proceedings of the<br />
Radiological Society of North America, 93rd Scientific<br />
Assembly and Annual Meeting. 2007.<br />
20. Barr RG, Lackey AE. The utility of the “bull’seye”<br />
artifact on breast elasticity imaging in reducing<br />
breast lesion biopsy rate. Ultrasound Quarterly<br />
2011;27:151-155.<br />
21. Barr RG, Grajo JR. Sensitivity and specificity of<br />
the “bull’s-eye” artifact on breast elasticity imaging<br />
to characterize cysts. Proceedings of the Radiological<br />
Society of North America, 94th Scientific<br />
Assembly and Annual Meeting. 2008.<br />
22. Grajo JR, Peterson CM, Barr RG. Does the<br />
EI/B-mode length ratio predict breast cancer tumor<br />
grade? Proceedings of the Ninth International<br />
Conference on the Ultrasonic Measurement and<br />
Imaging of Tissue Elasticity. 2010.<br />
WHERE RADIOLOGY PROFESSIONALS<br />
AND EMPLOYERS CONNECT<br />
CONNECT TODAY AT:<br />
RSNA.org/career<br />
• Access our growing resume database<br />
• Get added exposure through linked sites<br />
• Receive applicant e-mail notifications<br />
Great<br />
Low Rates!<br />
$225<br />
$325<br />
CAR142_CareerConnect-_8.125x5.4375_cmyk.indd 1 12-09-04 12:52 PM<br />
30-Day<br />
Posting<br />
60-Day<br />
Posting<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
n 23