Juvenile granulosa cell tumor of the ovary - Applied Radiology Online
Juvenile granulosa cell tumor of the ovary - Applied Radiology Online
Juvenile granulosa cell tumor of the ovary - Applied Radiology Online

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
R A D I O L O G I C A L C A S E<br />
<strong>Juvenile</strong> <strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong><br />
<strong>of</strong> <strong>the</strong> <strong>ovary</strong><br />
Jeremiah R. Long, MD, and David Danielson, DO<br />
CASE SUMMARY<br />
A 3-year-old girl presented to <strong>the</strong><br />
emergency department with an abdominal<br />
mass, symptoms <strong>of</strong> bowel obstruction,<br />
and evidence <strong>of</strong> precocious pu berty.<br />
Imaging studies were ordered.<br />
IMAGING FINDINGS<br />
An abdominal radiograph was initially<br />
obtained and raised suspicion for<br />
a possible intussusception (Figure 1).<br />
A subsequent abdominal ultrasound<br />
found a large complex low anterior<br />
abdominal mass abutting <strong>the</strong> uterine<br />
fundus measuring 10 × 6.6 × 9.3 cm<br />
(Figure 2). Laboratory analysis revealed<br />
a dramatically elevated serum estradiol<br />
level.<br />
Axial computed tomography (CT) <strong>of</strong><br />
<strong>the</strong> abdomen and pelvis was performed<br />
following <strong>the</strong> administration <strong>of</strong> oral and<br />
intravenous contrast material. The enhancing<br />
mass demonstrated both solid<br />
and cystic components. There was free<br />
fluid within <strong>the</strong> abdomen and pelvis, but<br />
no lymphadenopathy. Prominent subareolar<br />
breast tissue was noted on images<br />
through <strong>the</strong> lower chest.<br />
Based upon <strong>the</strong>se findings, <strong>the</strong> patient<br />
underwent laparotomy for <strong>tumor</strong><br />
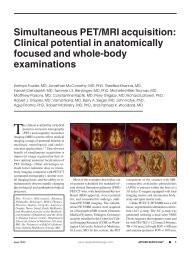
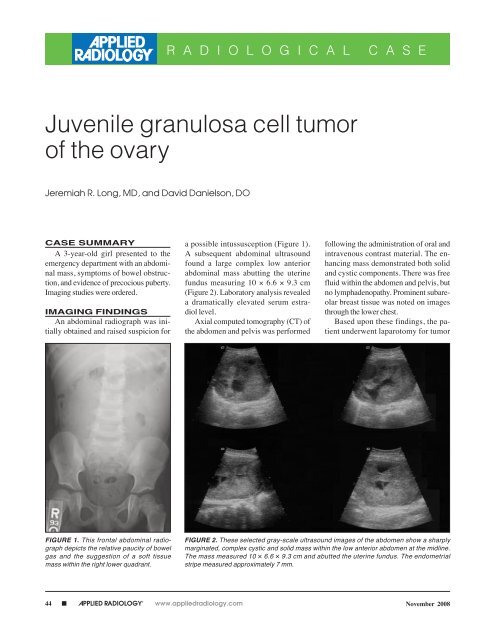
FIGURE 1. This frontal abdominal radiograph<br />
depicts <strong>the</strong> relative paucity <strong>of</strong> bowel<br />
gas and <strong>the</strong> suggestion <strong>of</strong> a s<strong>of</strong>t tissue<br />
mass within <strong>the</strong> right lower quadrant.<br />
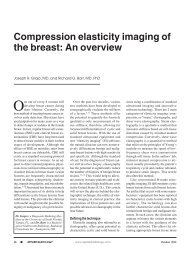
FIGURE 2. These selected gray-scale ultrasound images <strong>of</strong> <strong>the</strong> abdomen show a sharply<br />
marginated, complex cystic and solid mass within <strong>the</strong> low anterior abdomen at <strong>the</strong> midline.<br />
The mass measured 10 × 6.6 × 9.3 cm and abutted <strong>the</strong> uterine fundus. The endometrial<br />
stripe measured approximately 7 mm.<br />
44 ■ APPLIED RADIOLOGY © www.appliedradiology.com November 2008
R A D I O L O G I C A L C A S E<br />
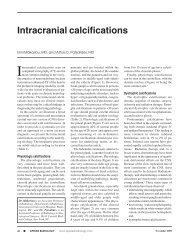
FIGURE 3. Selected CT images <strong>of</strong> <strong>the</strong> abdomen and pelvis following <strong>the</strong> administration <strong>of</strong> oral and intravenous contrast material depict <strong>the</strong><br />
well-circumscribed, heterogeneous, enhancing mass. The mass contained both cystic and solid components but no calcifications. There<br />
was free fluid within <strong>the</strong> abdomen and pelvis. No lymphadenopathy was present. Prominent subareolar breast tissue was noted on images<br />
through <strong>the</strong> lower chest.<br />
resection and unilateral salpingooophorectomy.<br />
DIAGNOSIS<br />
<strong>Juvenile</strong> <strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong> <strong>of</strong> <strong>the</strong><br />
<strong>ovary</strong><br />
DISCUSSION<br />
Ovarian cancer is <strong>the</strong> third most common<br />
neoplasm <strong>of</strong> <strong>the</strong> female genital<br />
tract, after carcinoma <strong>of</strong> <strong>the</strong> cervix and<br />
endometrium. It accounts for 6% <strong>of</strong> all<br />
cancers diagnosed in females, and stands<br />
as <strong>the</strong> leading cause <strong>of</strong> gynecological<br />
cancer death. This is primarily because<br />
80% <strong>of</strong> women with ovarian cancer present<br />
with advanced-stage disease. 1<br />
Based upon <strong>the</strong>ir <strong>cell</strong> type <strong>of</strong> origin,<br />
primary ovarian malignancies are classified<br />
into surface epi<strong>the</strong>lium, germ<br />
<strong>cell</strong>, or sex cord <strong>tumor</strong>s. Sex cord <strong>tumor</strong>s<br />
account for 1% to 2% <strong>of</strong> ovarian<br />
malignancies. They may contain <strong>granulosa</strong><br />
<strong>cell</strong>s, <strong>the</strong>cal <strong>cell</strong>s, Sertoli <strong>cell</strong>s, or<br />
fibroblasts <strong>of</strong> gonadal stromal origin.<br />
While approximately two thirds occur<br />
in postmenopausal women, <strong>the</strong>y can<br />
occur at any age, with 5% occurring in<br />
prepubescent patients. Approximately<br />
70% <strong>of</strong> sex cord <strong>tumor</strong>s are <strong>granulosa</strong><br />
46 ■ APPLIED RADIOLOGY © www.appliedradiology.com November 2008
<strong>cell</strong> <strong>tumor</strong>s. These <strong>tumor</strong>s are <strong>of</strong>ten hormonally<br />
active. Thecal <strong>cell</strong>s (luteinized<br />
<strong>cell</strong>s within <strong>the</strong> stroma) produce estrogen,<br />
and if present in large enough<br />
quantities within a <strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong>,<br />
can cause elevated serum estradiol levels.<br />
Additionally, <strong>the</strong>se <strong>tumor</strong>s may also<br />
secrete inhibin. Ovarian <strong>granulosa</strong> <strong>cell</strong><br />
<strong>tumor</strong>s may also express unique <strong>cell</strong><br />
surface markers that can be detected by<br />
staining sample tissue with histological<br />
markers. Surface expression <strong>of</strong> inhibin<br />
appears to have <strong>the</strong> greatest pathologic<br />
diagnostic potential for this <strong>tumor</strong> type. 2<br />
Among <strong>the</strong> histologic subtypes <strong>of</strong><br />
<strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong>s, juvenile <strong>granulosa</strong><br />
<strong>cell</strong> <strong>tumor</strong>s are rare, and typically<br />
present early. In a study <strong>of</strong> 125 patients<br />
with juvenile <strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong>s,<br />
78% presented within <strong>the</strong> first 2 decades<br />
<strong>of</strong> life. 3 Clinically, <strong>the</strong>se patients typically<br />
present with signs <strong>of</strong> hyperestrogenism—precocious<br />
puberty in prepubertal<br />
patients, menstrual irregularities<br />
in women <strong>of</strong> reproductive age, and<br />
abnormal uterine bleeding in postmenopausal<br />
women. 3 In addition, patients<br />
may complain <strong>of</strong> abdominal pain<br />
or an abdominal mass.<br />
Management <strong>of</strong> <strong>granulosa</strong> <strong>cell</strong><br />
<strong>tumor</strong>s (including <strong>the</strong> juvenile subtype)<br />
begins with surgery for definitive tissue<br />
diagnosis, staging, and debulking. Surgical<br />
<strong>tumor</strong> removal typically includes<br />
ipsilateral salpingo-oophorectomy for<br />
patients wishing to retain fertility, and<br />
total hysterectomy for older patients or<br />
patients who no longer desire fertility.<br />
The role <strong>of</strong> chemo<strong>the</strong>rapy or radiation<br />
<strong>the</strong>rapy in <strong>the</strong> treatment <strong>of</strong> <strong>granulosa</strong><br />
<strong>cell</strong> <strong>tumor</strong>s remains uncertain because<br />
<strong>of</strong> <strong>the</strong> lack <strong>of</strong> prospective randomized<br />
trials supporting <strong>the</strong>ir roles as adjuvant<br />
agents. 4 The paucity <strong>of</strong> extensive clinical<br />
trials reflects <strong>the</strong> overall rarity <strong>of</strong><br />
<strong>the</strong>se <strong>tumor</strong>s. Prognosis depends upon<br />
surgical stage at presentation. Fortunately,<br />
most patients are diagnosed at<br />
stage I, and enjoy a favorable prognosis.<br />
Patients diagnosed at stages II through<br />
IV tend to have poor clinical outcomes<br />
with a higher rate <strong>of</strong> disease recurrence.<br />
Granulosa <strong>cell</strong> <strong>tumor</strong>s in premenarchal<br />
girls appear to have a better outcome<br />
than those occuring in adult women. 5<br />
CONCLUSION<br />
<strong>Juvenile</strong> <strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong>s <strong>of</strong> <strong>the</strong><br />
<strong>ovary</strong> represent a small fraction <strong>of</strong> all<br />
primary ovarian malignancies. They<br />
typically present within <strong>the</strong> first 2 decades<br />
<strong>of</strong> life with signs <strong>of</strong> hyperestrogenism,<br />
and an abdominal mass. As <strong>the</strong><br />
majority <strong>of</strong> <strong>the</strong>se <strong>tumor</strong>s are diagnosed<br />
at stage I, <strong>the</strong>ir treatment remains surgical.<br />
The role <strong>of</strong> chemo<strong>the</strong>rapy and/or<br />
radiation <strong>the</strong>rapy remains unclear.<br />
Given <strong>the</strong> possibility for recurrence,<br />
long-term follow-up and surveillance is<br />
recommended for all patients.<br />
REFERENCES<br />
1. Funt SA, Hann LE. Detection and characterization<br />
<strong>of</strong> adnexal masses. Radiol Clin North Am.<br />
2002;40:591-608.<br />
2. McCluggage WG. Recent advances in immunohistochemistry<br />
in <strong>the</strong> diagnosis <strong>of</strong> ovarian neoplasms.<br />
J Clin Pathol. 2000;53:327-334.<br />
3. Young RH, Dickersin GR, Scully RE. <strong>Juvenile</strong><br />
<strong>granulosa</strong> <strong>cell</strong> <strong>tumor</strong> <strong>of</strong> <strong>the</strong> <strong>ovary</strong>. A clinicopathological<br />
analysis <strong>of</strong> 125 cases. Am J Surg Pathol.<br />
1984;8:575-596.<br />
4. Schumer ST, Cannistra SA. Granulosa <strong>cell</strong> <strong>tumor</strong><br />
<strong>of</strong> <strong>the</strong> <strong>ovary</strong>. J Clin Oncol. 2003;21:1180-1189.<br />
5. Lack EE, Perez-Atayde AR, Murthy AS, et al.<br />
Granulosa <strong>the</strong>ca <strong>cell</strong> <strong>tumor</strong>s in premenarchal girls:<br />
A clinical and pathologic study <strong>of</strong> ten cases. Cancer.<br />
1981;48:1846-1854.<br />
Prepared by Jeremiah R. Long, MD,<br />
Walter Reed Army Medical Center<br />
Department <strong>of</strong> <strong>Radiology</strong>, Washington,<br />
DC, and David M. Danielson, DO,<br />
Madigan Army Medical Center Department<br />
<strong>of</strong> <strong>Radiology</strong>, Tacoma, WA.<br />
The views expressed in this article are<br />
those <strong>of</strong> <strong>the</strong> authors and do not reflect<br />
<strong>the</strong> <strong>of</strong>ficial policy <strong>of</strong> <strong>the</strong> Department <strong>of</strong><br />
Army, Department <strong>of</strong> Defense, or U.S.<br />
Government.<br />
48 ■ APPLIED RADIOLOGY © www.appliedradiology.com<br />
November 2008