Intracranial calcifications - Applied Radiology Online
Intracranial calcifications - Applied Radiology Online
Intracranial calcifications - Applied Radiology Online

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Intracranial</strong> <strong>calcifications</strong><br />
Erini Makariou, MD, and Athos D. Patsalides, MD<br />
<strong>Intracranial</strong> <strong>calcifications</strong> seen on<br />
computed tomography (CT) are the<br />
most common finding in the everyday<br />
practice of neuroradiology, because<br />
noncontrast-enhanced CT of the head is<br />
the preferred imaging modality worldwide<br />
for the initial evaluation of patients<br />
with acute or chronic neurological<br />
problems. The intracranial <strong>calcifications</strong><br />
may have no clinical importance<br />
or they may be critical findings in<br />
diagnosing the underlying pathology.<br />
In this article, we illustrate a broad<br />
spectrum of common and uncommon<br />
central nervous system (CNS) disorders<br />
associated with <strong>calcifications</strong>. In<br />
order to provide a systematic review<br />
and an approach to a more accurate<br />
diagnosis, we present the intracranial<br />
<strong>calcifications</strong> according to the underlying<br />
etiology. The neoplastic processes<br />
are subdivided according to location<br />
(Table 1).<br />
Physiologic <strong>calcifications</strong><br />
The physiologic <strong>calcifications</strong> are<br />
very common and have been welldescribed<br />
in the past decades. They are<br />
associated with aging and can be seen<br />
in the basal ganglia, pineal gland, falx,<br />
tentorium, arachnoid granulations,<br />
choroid plexus and the cerebellum.<br />
Physiologic <strong>calcifications</strong> are almost<br />
never clinically significant. The <strong>calcifications</strong><br />
in the basal ganglia are usually<br />
Dr. Makariou is an Associate Professor<br />
of <strong>Radiology</strong>, Department of <strong>Radiology</strong>,<br />
Georgetown University Hospital, Washington,<br />
DC. and Dr. Patsalides is an<br />
Assistant Professor of <strong>Radiology</strong> in Neurological<br />
Surgery, Weill Cornell Medical<br />
College, New York, NY.<br />
48 ■ APPLIED RADIOLOGY ©<br />
punctate and are located within the<br />
globus pallidus, the head of the caudate<br />
nucleus, and the putamen and are very<br />
common in middle-aged individuals<br />
and the elderly (Figure 1). However,<br />
basal-ganglia <strong>calcifications</strong> in persons<br />
Physiologic<br />
Posttraumatic and dystrophic<br />
Subdural/epidural hematoma<br />
Radiation/chemotherapy<br />
Ischemia/infarct<br />
Although radiation therapy and<br />
chemotherapy probably have a synergistic<br />
role in the pathogenesis, radiation<br />
is the dominant factor in mineralizing<br />
microangiopathy. Finally, ischemic and<br />
hemorrhagic infarcts, parenchymal hemorrhage<br />
from trauma, and prior surgery<br />
are also associated with dystrophic<br />
<strong>calcifications</strong>.<br />
Congenital disorders/phakomatoses<br />
The phakomatoses are a group of<br />
hereditary disorders that affect structures<br />
November 2009<br />
Table 1. <strong>Intracranial</strong> <strong>calcifications</strong><br />
Congenital disorders (phakomatoses)<br />
Neurofibromatosis I and II<br />
Tuberous sclerosis<br />
Basal cell nevus syndrome<br />
Sturge-Weber syndrome<br />
Vascular disorders<br />
Vascular malformations: AVM/AVF, cavernous angioma, venous angioma, and<br />
capillary telengiectasia<br />
Aneurysm<br />
<strong>Intracranial</strong> atherosclerosis<br />
Ischemia/infarct<br />
Vein of Gallen malformation<br />
Infections<br />
Congenital: CMV, toxoplasmosis, HIV, herpes<br />
Acquired: Cysticercosis, tuberculosis, HIV, cryptococcosis<br />
Inflammatory disorders<br />
Sarcoidosis<br />
Systemic lupus erythematosus<br />
Tumors<br />
Intra-axial: Astrocytomas, oligodendroglioma, medulloblastoma, ganglioglioma,<br />
DNET, metastases<br />
Extra-axial: Meningioma, pineal tumors, pituitary tumors, craniopharyngioma,<br />
epidermoid/dermoid, teratoma, colloid cyst, lipoma, metastases<br />
Intraventricular: Ependymoma, choroid plexus tumors, central neurocytoma,<br />
metastases<br />
Metabolic<br />
Hyperparathyroidism<br />
Hypoparathyroidism<br />
Hypothyroidism<br />
Fahr disease<br />
MELAS syndrome<br />
of ectodermal origin. Classically, <strong>calcifications</strong><br />
are described in tuberous sclerosis<br />
and Sturge-Weber syndrome but can<br />
also be seen in neurofibromatosis and<br />
basal-cell nevus syndrome.<br />
Calcified subependymal hamartomas<br />
are common findings in tuberous<br />
sclerosis, usually located along the<br />
ventricular surface of the caudate<br />
nucleus (Figure 6), just posterior to the<br />
foramen of Monro. The cortical<br />
hamartomas seen in tuberous sclerosis<br />
are usually supratentorial and can also<br />
INTRACRANIAL CALCIFICATIONS<br />
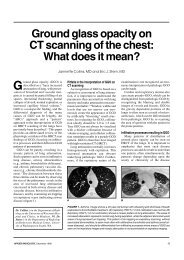
FIGURE 1. Physiologic <strong>calcifications</strong> in a<br />
51-year-old man with headache. Axial<br />
nonenhanced computed tomography (CT)<br />
image reveals physiologic <strong>calcifications</strong> of<br />
the basal ganglia bilaterally.<br />
Table 2. Basal ganglia<br />
<strong>calcifications</strong><br />
Physiologic/normal senescent<br />
(most common)<br />
Metabolic<br />
Hypoparathyroidism (including<br />
pseudo- and pseudopseudohypoparathyroidism)<br />
Hyperparathyroidism<br />
Hypothyroidism<br />
Lead toxicity<br />
Fahr disease<br />
Hallevorden Spatz disease<br />
Ischemic<br />
Carbon monoxide intoxication<br />
Birth anoxia<br />
Infectious<br />
AIDS<br />
TORCH encephalitis<br />
Toxoplasmosis<br />
Cysticercosis<br />
Congenital<br />
Trisomy 21<br />
Tuberous sclerosis<br />
Neurofibromatosis<br />
Chemotherapy (methotrexate)<br />
Radiation therapy<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
■ 49
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 2. Physiologic <strong>calcifications</strong> in a 55year-old<br />
woman with headache. Axial<br />
nonenhanced CT image reveals physiologic<br />
<strong>calcifications</strong> of the pineal gland and the<br />
choroid plexuses bilaterally.<br />
A B<br />
calcify. Calcifications in the subependymal<br />
and cortical hamartomas are<br />
rare during the first year of life and<br />
the rate increases along with the<br />
patient’s age.<br />
Subependymal giant-cell astrocytomas<br />
are another major manifestation<br />
of tuberous sclerosis that can present<br />
as a calcified nodule. These lesions are<br />
larger than the subependymal nodules,<br />
show interval growth, enhance on postcontrast<br />
images and are located at or<br />
50 ■ APPLIED RADIOLOGY ©<br />
FIGURE 3. Calcified falx in a 46-year-old<br />
woman with subarachnoid hemorrhage.<br />
Axial nonenhanced CT image shows dense<br />
<strong>calcifications</strong> of the anterior falx. Subarachnoid<br />
hemorrhage is seen in the sulci of the<br />
right parietal lobe.<br />
FIGURE 5. 50-year-old man with chronic right subdural hematoma. Axial nonenhanced CT<br />
image (A) shows a chronic, right, subdural hygroma with <strong>calcifications</strong> along the inner surface.<br />
Axial CT image of the skull in bone windows (B) shows <strong>calcifications</strong>.<br />
near the foramen of Monro. 9 Gyriform<br />
cortical <strong>calcifications</strong>, with a pattern<br />
similar to Sturge-Weber, are sometimes<br />
seen as well. 10<br />
The most common <strong>calcifications</strong><br />
seen in patients with neurofibromatosis<br />
type 2 (NF2) are the ones associated<br />
with disease-related tumors, such as<br />
meningiomas. Nontumoral <strong>calcifications</strong><br />
have also been described in these<br />
patients, with symmetric or asymmetric<br />
<strong>calcifications</strong> of the choroid plexus<br />
FIGURE 4. Physiologic <strong>calcifications</strong> of the<br />
dentate nuclei in a 86-year-old woman. Axial<br />
nonenhanced CT image shows prominent<br />
symmetric <strong>calcifications</strong> in the dentate<br />
nuclei bilaterally.<br />
FIGURE 6. 21-year-old patient with tuberous<br />
sclerosis presents with seizures and<br />
mental retardation. Axial noncontrast CT<br />
image reveals calcified subependymal<br />
hamartomas along the lateral ventricles and<br />
the region of the foramina of Monro. The<br />
largest lesion adjacent to the left foramen of<br />
Monro is a giant cell astrocytoma.<br />
in the lateral ventricles and nodular<br />
<strong>calcifications</strong> of the cerebellum 11 being<br />
most commonly observed. Cortical<br />
<strong>calcifications</strong> are less common. Vouge<br />
et al. 12 described subependymal <strong>calcifications</strong><br />
in a series of patients with NF2,<br />
similar to the <strong>calcifications</strong> seen in<br />
tuberous sclerosis.<br />
www.appliedradiology.com November 2009
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 7. 21-year-old patient with basal<br />
cell nevus syndrome. Axial noncontrast<br />
CT image shows dense calcification along<br />
the falx.<br />
FIGURE 9. Atherosclerosis of the intracranial<br />
arteries in a 70-year-old man. Axial<br />
nonenhanced CT image (bone algorithm)<br />
shows wall <strong>calcifications</strong> of the supraclinoid<br />
internal carotid arteries.<br />
Early dural <strong>calcifications</strong> are a common<br />
manifestation of the basal-cell<br />
nevus syndrome; they involve the falx<br />
(Figure 7), the diaphragma sella and<br />
the tentorium. These are also locations<br />
of physiologic <strong>calcifications</strong>, but in<br />
patients with basal-cell nevus syndrome,<br />
the <strong>calcifications</strong> appear in<br />
younger age groups. 13 One of the typical<br />
imaging findings in Sturge-Weber<br />
52 ■ APPLIED RADIOLOGY ©<br />
A B<br />
FIGURE 8. Six-year-old boy with Sturge-Weber syndrome. Posterioanterior radiograph (A) of<br />
the skull shows tram-track <strong>calcifications</strong> of the right side of the head. Axial nonenhanced CT<br />
image (B) shows dense gyriform <strong>calcifications</strong> in the cortex of the right frontotemporal region<br />
with associated brain volume loss. There is compensatory dilatation of the right lateral ventricle.<br />
FIGURE 10. Atherosclerosis of the left vertebrobasilar<br />
system in a 41-year-old man<br />
with lymphoma, status post kidney transplantation.<br />
Axial nonenhanced CT image<br />
reveals an elongated prominent left vertebrobasilar<br />
artery with wall <strong>calcifications</strong>.<br />
syndrome is calcification occurring<br />
adjacent to a pial angioma, originating<br />
in the subcortical white matter and<br />
then extending to the cortex (Figure 8).<br />
The parieto-occipital cortex is the most<br />
common location for cortical <strong>calcifications</strong>,<br />
but they may occur anywhere in<br />
the cerebrum. In 20% of patients these<br />
<strong>calcifications</strong> are bilateral. 14<br />
Vascular <strong>calcifications</strong><br />
Calcifications in the arterial wall of<br />
large intracranial vessels are common<br />
and should be mentioned in the report<br />
because of their association with atherosclerosis.<br />
It is also important to be<br />
aware of other calcification patterns<br />
associated with vascular pathology,<br />
such as vascular malformations and<br />
aneurysms.<br />
Atherosclerosis is associated with<br />
mural <strong>calcifications</strong> of the major intracranial<br />
arteries. 15 The carotid siphon<br />
(Figure 9) is the most commonly<br />
affected vessel, while <strong>calcifications</strong> in<br />
the anterior and middle cerebral arteries<br />
and the vertebrobasilar system<br />
(Figure 10) are less common.<br />
Arteriovenous malformations (AVMs)<br />
are associated with dystrophic intracranial<br />
<strong>calcifications</strong>. These are seen in<br />
the watershed or other areas away from<br />
the AVM nidus due to ischemic brain<br />
tissue as a result of the “vascular steal”<br />
from the AVM. 16 Calcification can also<br />
be seen in the AVM nidus. 17 AVMs are<br />
associated with mural <strong>calcifications</strong> in<br />
the ectatic veins associated with the<br />
fistula. 18 Patients with cavernous<br />
angiomas (Figure 11) often have stippled<br />
<strong>calcifications</strong> 19 in the vessel wall<br />
or the adjacent brain parenchyma.<br />
www.appliedradiology.com November 2009
A B<br />
FIGURE 11. Cavernous angioma in the pons of a 30-year-old man with headaches. Axial<br />
nonenhanced CT image (A) reveals a round hyperdense lesion with punctate <strong>calcifications</strong> in<br />
the pons. There is no associated mass effect or surrounding edema. Hyperdense foci in CSF<br />
spaces are Pantopaque residue from a previous myelogram. T2-weigheted (T2W) magnetic<br />
resonance (MR) image (B) at the level of the pons shows a lesion with mixed signal intensity<br />
and a rim of low signal intensity due to hemosiderin deposition.<br />
A B<br />
FIGURE 12: Calcifications related to a venous angioma in a 50-year-old woman with<br />
headaches. Axial nonenhanced CT image (A) shows a wedge-shaped calcified area in the left<br />
frontal lobe. Coronal nonenhanced T1-weighted (T1W) MR image (B) reveals the classic<br />
appearance of a venous angioma in the left frontal lobe (arrow).<br />
These are more commonly seen in<br />
nonhemorrhagic lesions. 20 Calcifications<br />
in developmental venous anomalies<br />
(venous angioma, Figure 12) and<br />
capillary telangiectasias have been<br />
occasionally described. 21–23 Brain aneurysms<br />
(Figure 13) often have mural<br />
<strong>calcifications</strong>, more often seen in fusiform<br />
24 compared with saccular aneurysms.<br />
Amyloid angiopathy results in<br />
November 2009<br />
gyriform calcification and sclerotic<br />
changes in the medullary arteries. 25<br />
Congenital infections<br />
<strong>Intracranial</strong> <strong>calcifications</strong> are common<br />
in patients with congenital infections,<br />
but their appearance is not<br />
specific because they reflect dystrophic<br />
<strong>calcifications</strong> similar to any chronic<br />
brain injury. Basal ganglia and cortical<br />
INTRACRANIAL CALCIFICATIONS<br />
A<br />
FIGURE 13. 75-year-old man with a giant<br />
thrombosed left ICA aneurysm. Lateral radiograph<br />
of the skull (A) shows a round lesion<br />
with rim <strong>calcifications</strong> in the suprasellar<br />
region. Coronal postcontrast CT image (B)<br />
shows a peripherally calcified round lesion in<br />
the suprasellar region without enhancement.<br />
The left middle and anterior cerebral arteries<br />
are not visualized. Lateral view of a left<br />
carotid angiogram (C) reveals no enhancement<br />
of the round calcified lesion.<br />
<strong>calcifications</strong> are common features of<br />
all infections that constitute the<br />
TORCH syndrome (toxoplasmosis,<br />
other, rubella, cytomegalovirus, herpes<br />
simplex virus).<br />
Cytomegalovirus and toxoplasmosis<br />
(Figure 14) infections result in periventricular<br />
and subependymal <strong>calcifications</strong>.<br />
26 Interestingly, <strong>calcifications</strong> in<br />
patients infected with toxoplasmosis<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
B<br />
C<br />
■ 53
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 14. Congenital toxoplasmosis in a<br />
6-year-old boy with seizures and mental<br />
retardation. Axial noncontrast CT image<br />
reveals dense <strong>calcifications</strong> in the basal<br />
ganglia and subcortical white matter bilaterally.<br />
There is brain volume loss with<br />
colpocephaly.<br />
may resolve after treatment. 27 Congenital<br />
HIV infection (Figure 15) is associated<br />
with periventricular frontal<br />
white-matter and cerebellar <strong>calcifications</strong>.<br />
28 Congenital herpes (HSV-2)<br />
infection is associated with thalamic,<br />
periventricular, and punctate cortical 29<br />
or extensive gyral <strong>calcifications</strong>. 30<br />
Acquired infections<br />
Cysticercosis, tuberculosis, HIV and<br />
cryptococcus are the most common<br />
acquired intracranial infections typically<br />
associated with <strong>calcifications</strong>. As<br />
in the case of congenital infections, the<br />
pattern of calcification is not specific<br />
but is still useful in making the diagnosis<br />
and evaluating disease progression.<br />
In cysticercosis (Figure 16), <strong>calcifications</strong><br />
are seen in the dead larva (granular-nodular<br />
stage) and the typical<br />
appearance is that of a small, calcified<br />
cyst containing an eccentric calcified<br />
nodule that represents the dead scolex.<br />
The most common locations for the <strong>calcifications</strong><br />
are the subaracnhoid spaces<br />
in the convexities, ventricles, and basal<br />
cisterns and the brain parenchyma, especially<br />
the gray-white matter junction.<br />
Tuberculosis results in calcified<br />
parenchymal granulomata in 10% to<br />
54 ■ APPLIED RADIOLOGY ©<br />
A B<br />
FIGURE 15. 5-year-old boy with congenital HIV infection with generalized atrophy. Axial<br />
nonenhanced CT image (A) shows <strong>calcifications</strong> in the subcortical white matter of the frontal<br />
lobes and the dentate nuclei. Axial nonenhanced CT image (B) shows additional <strong>calcifications</strong><br />
in the basal ganglia bilaterally.<br />
20% of patients; 31 meningeal <strong>calcifications</strong><br />
are much less common. HIV<br />
encephalitis is associated with basal<br />
ganglia calcification. 32 Cryptococcus<br />
affects immunocompromised patients<br />
and <strong>calcifications</strong> can be seen in both<br />
the brain parenchyma 33 and the leptomeninges.<br />
34<br />
Inflammatory lesions<br />
Sarcoidosis involves the leptomeninges,<br />
producing granulomas of the<br />
pituitary stalk and the optic chiasm.<br />
Calcified sarcoid granulomas can also<br />
be seen in the pituitary, pons, hypothalamus<br />
and the periventricular white<br />
matter. Systemic lupus erythematosus<br />
(Figure 17) has been associated with<br />
cerebral <strong>calcifications</strong> in the basal ganglia,<br />
thalamus, cerebellum and centrum<br />
semiovale. 35<br />
Tumors<br />
Commonly calcified intracranial<br />
tumors include the oligodendrogliomas,<br />
low-grade astrocytomas, craniopharyngiomas,<br />
meningiomas, pineal gland<br />
tumors and the ependymomas. Since<br />
many tumors have overlapping imaging<br />
findings, knowing which tumors calcify<br />
is useful in limiting the differential<br />
diagnosis. In some instances, the presence<br />
and pattern of calcification can be<br />
essentially pathognomonic as in the<br />
case of oligodendrogliomas and craniopharyngiomas.<br />
We present the intracranial tumors<br />
that calcify divided into intra- and extraaxial<br />
and intraventricular, in order to<br />
make the differential diagnosis more<br />
meaningful. The presence or absence of<br />
<strong>calcifications</strong> is not related to the benign<br />
or malignant nature of the tumor.<br />
Intra-axial tumors<br />
The diffuse low-grade astrocytomas<br />
(Figure 18) are the most common glial<br />
neoplasms demonstrating <strong>calcifications</strong>;<br />
however, only the minority of these<br />
tumors calcify. 36 The calcification can be<br />
linear, diffuse, punctate or multifocal<br />
and may follow the white-matter tracts,<br />
especially with large tumors. 37 Calcifications<br />
are present in the majority of<br />
subependymal giant-cell astrocytomas<br />
in the form of calcified chunks or nodules.<br />
38,39 Up to 25% of pilocytic astrocytomas<br />
have intratumoral calcification.<br />
Other astrocytomas such as the pleomorphic<br />
xanthostrocytoma, anaplastic<br />
astrocytomas and glioblastoma multiforme<br />
(Figure 19) only rarely calcify.<br />
www.appliedradiology.com November 2009
A B<br />
C D<br />
FIGURE 16. Cysticercosis in a 32-year-old man with seizures and headaches. Axial nonenhanced<br />
CT image (A) shows several punctuate <strong>calcifications</strong> in the parenchyma and along the<br />
left frontal horn. Axial nonenhanced CT image (B) shows several punctuate <strong>calcifications</strong> in<br />
the parenchyma. Axial contrast-enhanced T1W MR image (C) shows enhancement of the left<br />
frontal horn lesion (arrow). Coronal contrast-enhanced T1W MR image (D) shows an enhancing<br />
lesion in the right temporal lobe (arrow).<br />
The oligodendrogliomas (Figure 20)<br />
exhibit the highest frequency of calcification<br />
among all brain tumors, since up to<br />
90% of them calcify. 40,41 The <strong>calcifications</strong><br />
in oligodendrogliomas can be central<br />
or peripheral, punctate or ribbon like,<br />
usually located within walls of intrinsic<br />
tumor vessels. 42 Calcifications may even<br />
extend to the surrounding brain<br />
parenchyma. The medulloblastomas<br />
show small, clumplike or nodular <strong>calcifications</strong><br />
in approximately 20% of cases. 43<br />
Calcifications are typically seen in the<br />
majority of gangliocytomas 44 and in<br />
November 2009<br />
approximately 40% of gangliogliomas<br />
(Figure 21). 45 The <strong>calcifications</strong> are more<br />
commonly seen in cystic rather than solid<br />
gangliogliomas. 46 Dysembryoplastic neuroepithelial<br />
tumors have a calcification<br />
pattern similar to oligodendrogliomas but<br />
only a small percentage of these tumors<br />
calcify. 47 Calcified intracranial metastases<br />
(Figure 22) are very rare and have been<br />
primarily described in case reports. 48 The<br />
osteogenic sarcoma, lung and breast carcinomas<br />
are the most common primary<br />
tumors with brain metastases that<br />
calcify. 49<br />
INTRACRANIAL CALCIFICATIONS<br />
Extra-axial tumors<br />
The percentage of meningiomas<br />
(Figures 23–25) that calcify ranges<br />
from 20% to 69%. 36,50 The <strong>calcifications</strong><br />
can be focal, diffuse, coarse, sand-like<br />
or even rim. There is a higher percentage<br />
of calcified meningiomas in children,<br />
which could be associated with<br />
more aggressive subtypes of meningiomas.<br />
51 Pineal gland <strong>calcifications</strong> are<br />
very common: seen in approximately<br />
40% of normal people by the age of<br />
20 years. 1 Compact pineal <strong>calcifications</strong><br />
measuring
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 18. Low-grade astrocytoma in a 75year-old<br />
woman. Axial nonenhanced CT image<br />
shows a left posterior frontal/parietal mass<br />
with dense <strong>calcifications</strong>, surrounding edema<br />
and mass effect on adjacent parenchyma.<br />
A<br />
B<br />
FIGURE 21. 25-year-old man with ganglioglioma<br />
in the right temporal lobe. Axial<br />
nonenhanced CT image (A) shows a completely<br />
calcified lesion in the right temporal<br />
lobe without associated edema or mass<br />
effect. Axial nonenhanced CT image (B, bone<br />
algorithm) shows the densely calcified lesion<br />
in the right temporal lobe.<br />
56 ■ APPLIED RADIOLOGY ©<br />
FIGURE 19. Gliobastoma multiforme in a<br />
44-year-old. Axial nonenhanced CT image<br />
shows a heterogenous lesion with peripheral<br />
irregular <strong>calcifications</strong> in the left basal ganglia<br />
region with a large zone of surrounding vasogenic<br />
edema. The lesion produces mass<br />
effect on the lateral ventricles and midline<br />
shift to the right.<br />
A B<br />
not associated with underlying pathology.<br />
Larger pineal gland <strong>calcifications</strong><br />
however, are worrisome for pineal<br />
gland tumors.<br />
Among the pineal cell parenchymal<br />
tumors, the pineocytomas are the ones<br />
that calcify more frequently, showing<br />
FIGURE 20. 35-year-old man with left frontal<br />
oligodendroglioma and history of seizures.<br />
Axial nonenhanced CT image shows a<br />
round lesion with peripheral <strong>calcifications</strong><br />
and a small surrounding zone of edema.<br />
FIGURE 22. Calcified brain metastases in a 65-year-old-man with prostate cancer. Axial<br />
nonenhanced CT image (A) shows a dense calcified lesion with surrounding vasogenic edema<br />
in the left frontal lobe. A calcified focus is seen in the right frontal lobe. Axial nonenhanced CT<br />
image (B) shows calcified lesions with a small zone of edema in both parietal lobes.<br />
either peripheral or central <strong>calcifications</strong>.<br />
Peripheral <strong>calcifications</strong> are<br />
thought to be native pineal body <strong>calcifications</strong><br />
displaced by the tumor,<br />
whereas the central <strong>calcifications</strong> are<br />
produced by the tumor itself. 52 Among<br />
the pineal tumors arising from germ<br />
www.appliedradiology.com November 2009
A B<br />
FIGURE 23. 58-year-old woman with a calcified occipital meningioma. Axial nonenhanced CT<br />
image (A) shows a calcified, broad-based, extra-axial lesion in the occipital regions. Axial<br />
nonenhanced CT image (B, bone algorithm) shows the calcified lesion in the occipital regions.<br />
A B<br />
FIGURE 25. Small suprasellar calcified meningioma in a 78-year-old woman. Axial nonenhanced<br />
CT image (A) shows a round, well-defined, calcified lesion in the suprasellar region.<br />
Axial nonenhanced CT image (B, bone algorithm) shows the calcification.The same lesion on<br />
MRI is isointense on T1W and hypointense on T2W images with a dural tail and minimal<br />
peripheral enhancement (not shown).<br />
cells, teratomas commonly have dense<br />
<strong>calcifications</strong>. The germinomas very<br />
rarely calcify but may displace or<br />
engulf preexisting physiologic pineal<br />
gland <strong>calcifications</strong>. 53 Seventy percent<br />
to ninety percent of craniopharyngiomas<br />
(Figure 26) are seen in children<br />
with <strong>calcifications</strong>, and 30% to 40% of<br />
craniopharyngiomas are seen in adults<br />
who have <strong>calcifications</strong>. This is<br />
explained by the different histology of<br />
the tumor in different age groups; the<br />
November 2009<br />
adamantinous craniopharyngiomas are<br />
usually seen in children and almost<br />
always (90%) calcify either in the<br />
periphery and/or the solid component<br />
of the tumor. 54 The squamous papillary<br />
craniopharyngiomas are more often<br />
seen in adults and are less likely to calcify.<br />
Dermoid and epidermoid tumors<br />
show peripheral stippled calcification<br />
in approximately 20% to 25% of cases 55<br />
while teratomas typically show internal<br />
<strong>calcifications</strong>. 56 Pituitary adenomas do<br />
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 24. 69-year-old woman with partially<br />
calcified meningioma. Axial nonenhanced CT<br />
image shows a broad-based, partially calcified,<br />
extra-axial lesion in the right cerebellopontine<br />
angle. There is associated hyperostosis<br />
of the petrous bone and mass effect<br />
on the pons and right cerebellum.<br />
not calcify frequently. They should be<br />
suspected however, when calcification<br />
is seen within the pituitary gland. 57,58<br />
Pericallosal and interhemispheric<br />
lipomas may show calcification of the<br />
fibrous capsule with rim or eggshell<br />
appearance. The calcification can also<br />
be located in the center of the lipoma.<br />
Lipomas located elsewhere, are much<br />
less likely to show <strong>calcifications</strong>. 59,60<br />
Colloid cysts rarely calcify. 61<br />
Intraventricular tumors<br />
Intraventricular ependymomas typically<br />
calcify, ranging from punctate<br />
to mass-like <strong>calcifications</strong>. 62,63 Posterior<br />
fossa ependymomas exhibit small, round<br />
<strong>calcifications</strong> up to 50% 64 and have the<br />
highest frequency of calcification among<br />
the posterior fossa tumors. The subependymomas<br />
calcify in approximately<br />
one third of cases and usually demonstrate<br />
small foci of calcification. 65,66 The<br />
choroid plexus papillomas and carcinomas<br />
have punctate <strong>calcifications</strong> in<br />
approximately 25% of cases. 38 The central<br />
neurocytomas (Figure 27) were<br />
thought to characteristically show globular<br />
<strong>calcifications</strong>. 68 Other authors, however,<br />
reported <strong>calcifications</strong> in only 50%<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
■ 57
INTRACRANIAL CALCIFICATIONS<br />
A B<br />
FIGURE 26. Peripherally calcified craniopharyngioma in a 55-year-old woman complaining of<br />
headaches and vision disturbances. Axial nonenhanced CT image (A) shows a round, peripherally<br />
calcified lesion compromising the third ventricle, resulting in obstructive hydrocephalus.<br />
Coronal postcontrast T1W MR image (B) shows the suprasellar lesion with an enhancing rim.<br />
FIGURE 28. 45-year-old woman with intraventricular<br />
meningioma. Axial nonenhanced<br />
CT image shows a well-defined, ovoid,<br />
densely calcified lesion in the region of the<br />
third ventricle extending into the frontal<br />
horns. There is mild dilatation of the lateral<br />
ventricles.<br />
of these tumors. 67 The calcification in<br />
these tumors is variable, ranging from<br />
punctate to mass like. Intraventricular<br />
meningiomas (Figure 28) calcify in<br />
approximately 50% of cases, 62 with calcification<br />
patterns similar to the extraaxial<br />
meningiomas.<br />
Endocrine/metabolic/idiopathic<br />
Metabolic disorders affecting the<br />
calcium homeostasis are associated<br />
with intracranial <strong>calcifications</strong> that<br />
58 ■ APPLIED RADIOLOGY ©<br />
A B<br />
C D<br />
FIGURE 27. Calcified central neurocytoma in<br />
a 35-year-old with headaches. Axial nonenhanced<br />
CT image shows a densely calcified,<br />
well-defined, irregularly shaped mass in the<br />
region of the septum pellucidum and left<br />
frontal horn. The left frontal horn is enlarged.<br />
FIGURE 29. Progressive brain <strong>calcifications</strong> in a 31-year-old HIV-positive patient with renal<br />
failure on dialysis. Axial nonenhanced CT image (A) shows punctuate <strong>calcifications</strong> in the<br />
globus pallidus bilaterally and along the posterior falx. Calcifications are also seen along the<br />
tentorium, bilaterally (B). Five months later, another CT study of the head (C) showed marked<br />
progression of these <strong>calcifications</strong> in the globus pallidus, along the posterior falx and the tentorium<br />
bilaterally (D).<br />
www.appliedradiology.com November 2009
A B<br />
FIGURE 30. 50-year-old man with hypoparathyroidism. Nonenhanced axial CT image (A)<br />
shows areas of <strong>calcifications</strong> in the subcortical white matter and the basal ganglia. Nonenhanced<br />
axial CT image (B) shows areas of <strong>calcifications</strong> in the subcortical white matter and<br />
the basal ganglia.<br />
predominantly involve the basal ganglia.<br />
Although the pattern is similar to<br />
the physiologic, age-related <strong>calcifications</strong>,<br />
they appear at younger ages and<br />
are often progressive. Basal ganglia<br />
and subcortical <strong>calcifications</strong> have been<br />
described in patients with chronic renal<br />
failure and secondary hyperparathyroidism<br />
(Figure 29). 69 In patients with<br />
hypoparathyroidism (Figure 30), the<br />
<strong>calcifications</strong> typically involve the<br />
basal ganglia, thalami, and the cerebellum.<br />
70 <strong>Intracranial</strong> <strong>calcifications</strong> are<br />
more commonly seen in the pseudorather<br />
than idiopathic hypoparathyroidism.<br />
71 Hypothyroidism is also associated<br />
with basal ganglia and cerebellar<br />
<strong>calcifications</strong>.<br />
<strong>Intracranial</strong> <strong>calcifications</strong> can also<br />
be seen in rare idiopathic disorders<br />
such as Fahr disease (bilateral striopallidodentate<br />
calcinosis, Figure 31). This<br />
disease shows characteristic <strong>calcifications</strong><br />
in the basal ganglia, especially in<br />
the lateral globus pallidus. Other involved<br />
areas are the thalami, the cerebral<br />
white matter and the dentate<br />
nuclei of the cerebellum. 72 Progressive<br />
and symmetric basal ganglia <strong>calcifications</strong><br />
are the commonest radiological<br />
finding of MELAS syndrome. 73<br />
November 2009<br />
Conclusion<br />
Knowledge of physiologic <strong>calcifications</strong><br />
in the brain parenchyma is essential<br />
to avoid misinterpretations. However,<br />
several pathologic conditions<br />
involving the brain are associated with<br />
<strong>calcifications</strong> and the recognition of<br />
their appearance and distribution helps<br />
narrow the differential diagnosis.<br />
REFERENCES<br />
1. Zimmerman RA, Bilaniuk LT. Age-related incidence<br />
of pineal calcification detected by computed<br />
tomography. <strong>Radiology</strong>. 1982;142:659-662.<br />
2. Roche J, Warner D. Arachnoid granulations in the<br />
transverse and sigmoid sinuses CT, MR, and MR<br />
angiographic appearance of a normal anatomic variation.<br />
AJNR Am J Neuroradiol. 1996;17:677-683.<br />
3. Kendall B, Cavanagh N. <strong>Intracranial</strong> calcification<br />
in paediatric computed tomography. Neuroradiology.<br />
1986;28:324-330.<br />
4. Koller WC, Klawans HL. Cerebellar calcification<br />
on computerized tomography. Ann Neurol. 1980;7:<br />
193-194.<br />
5. Sato K, Yamada M, Shimzu S, et al. Infected and<br />
calcified chronic subdural hematoma presenting an<br />
attitude of acute hematoma on MRI: Case report. No<br />
Shinkei Geka. 2005;33:805-808.<br />
6. Chang JH, Choi JY, Chang JW, et al. Chronic<br />
epidural hematoma with rapid ossification. Childs<br />
Nerv Syst. 2002;18:712-716.<br />
7. Erdogan B, Sen O, Bal N, Cekinmez M, et al.<br />
Rapidly calcifying and ossifying epidural hematoma.<br />
Pediatr Neurosurg. 2003;39:208-211.<br />
8. Fernandez-Bouzas A, Ramirez Jimenez H,<br />
Vazquez Zamudio J, et al. Brain <strong>calcifications</strong> and<br />
dementia in children treated with radiotherapy and<br />
INTRACRANIAL CALCIFICATIONS<br />
FIGURE 31. 42-year-old with Fahr disease<br />
and progressive mental deterioration. Axial<br />
nonenhanced CT image shows prominent<br />
<strong>calcifications</strong> in the white matter of the<br />
frontal lobes and in the basal ganglia. There<br />
is also brain volume loss.<br />
intrathecal methotrexate. J Neurosurg Sci. 1992;36:<br />
211-214.<br />
9. Kingsley DP, Kendall BE, Fitz CR. Tuberous<br />
sclerosis: A clinicoradiological evaluation of 110<br />
cases with particular reference to atypical presentation.<br />
Neuroradiology. 1986;28:38-46.<br />
10. Wilms G, Van Wijck E, Demaerel P, et al. Gyriform<br />
<strong>calcifications</strong> in tuberous sclerosis simulating<br />
the appearance of Sturge-Weber disease. AJNR<br />
Am J Neuroradiol. 1992;13:295-7.<br />
11. Mayfrank L, Mohadjer M, Wullich B. <strong>Intracranial</strong><br />
calcified deposits in neurofibromatosis type 2. A CT<br />
study of 11 cases. Neuroradiology. 1990;32:33-37.<br />
12. Vouge M, Pasquini U, Salvolini U. CT findings<br />
of atypical forms of phakomatosis. Neuroradiology.<br />
1980;20:99-101.<br />
13. Stavrou T, Dubovsky EC, Reaman GH, et al.<br />
<strong>Intracranial</strong> <strong>calcifications</strong> in childhood medulloblastoma:<br />
Relation to nevoid basal cell carcinoma syndrome.<br />
AJNR Am J Neuroradiol. 2000;21:790-794.<br />
14. Gardeur D, Palmieri A, Mashaly R. Cranial<br />
computed tomography in the phakomatoses. Neuroradiology.<br />
1983;25:293-304.<br />
15. Savy LE, Moseley IF. <strong>Intracranial</strong> arterial calcification<br />
and ectasia in visual failure. Br J Radiol.<br />
1996;69:394-401.<br />
16. Yu YL, Chiu EK, Woo E, et al. Dystrophic<br />
intracranial calcification: CT evidence of ‘cerebral<br />
steal’ from arteriovenous malformation. Neuroradiology.<br />
1987;29:519-522.<br />
17. Yamamoto M, Jimbo M, Ide M, et al. Gamma<br />
knife radiosurgery in cerebral arteriovenous malformations:<br />
Postobliteration nidus changes observed<br />
on neurodiagnostic imaging. Stereotact Funct Neurosurg.<br />
1995;64 (Suppl 1):126-133.<br />
18. Tomlinson FH, Rufenacht DA, Sundt TM Jr, et<br />
al. Arteriovenous fistulas of the brain and the spinal<br />
cord. J Neurosurg. 1993;79:16-27.<br />
www.appliedradiology.com APPLIED RADIOLOGY ©<br />
■ 59
INTRACRANIAL CALCIFICATIONS<br />
19. Shaida AM, McFerran DJ, da Cruz M, et al. Cavernous<br />
haemangioma of the internal auditory canal.<br />
J Laryngol Otol. 2000;114:453-455.<br />
20. Nakase H, Morimoto T, Tsunoda S, et al. Cortical<br />
and subcortical cavernous angioma: A comparison of<br />
patients with and without hemorrhage as the initial<br />
symptom. Neurol Med Chir. (Tokyo) 1992;32:196-200.<br />
21. Fontaine S, de la Sayette V, Gianfelice D, et al.<br />
CT, MRI, and angiography of venous angiomas: A<br />
comparative study. Can Assoc Radiol J. 1987;38:<br />
259-263.<br />
22. Ramina R, Ingunza W, Vonofakos D. Cystic<br />
cerebral cavernous angioma with dense calcification.<br />
Case report. J Neurosurg. 1980;52:259-262.<br />
23. Runnels JB, Gifford DB, Forsberg PL, Hanberry<br />
JW. Dense calcification in a large cavernous angioma.<br />
Case report. J Neurosurg. 1969;30:293-298.<br />
24. Yasui T, Komiyama M, Nishikawa M, et al.<br />
Fusiform vertebral artery aneurysms as a cause of<br />
dissecting aneurysms. Report of two autopsy cases<br />
and a review of the literature. J Neurosurg. 1999;91:<br />
139-144.<br />
25. Terada S, Ishizu H, Tanabe Y, et al. Plaque-like<br />
structures and arteriosclerotic changes in “diffuse<br />
neurofibrillary tangles with calcification.” Acta Neuropathol.<br />
2001;102:597-603.<br />
26. Collins AT, Cromwell LD. Computed tomography<br />
in the evaluation of congenital cerebral toxoplasmosis.<br />
J Comput Assist Tomogr. 1980;4:326-329.<br />
27. Patel DV, Holfels EM, Vogel NP, et al. Resolution<br />
of intracranial <strong>calcifications</strong> in infants with treated<br />
congenital toxoplasmosis. <strong>Radiology</strong>. 1996;199:<br />
433-440.<br />
28. Kauffman WM, Sivit CJ, Fitz CR, et al. CT and<br />
MR evaluation of intracranial involvement in pediatric<br />
HIV infection: A clinical-imaging correlation.<br />
AJNR Am J Neuroradiol. 1992;13:949-957.<br />
29. Benator RM, Magill HL, Gerald B, et al. Herpes<br />
simplex encephalitis: CT findings in the neonate<br />
and young infant. AJNR Am J Neuroradiol. 1985;6:<br />
539-543.<br />
30. Dublin AB, Merten DF. Computed tomography in<br />
the evaluation of herpes simplex encephalitis. <strong>Radiology</strong>.<br />
1977;125:133-134.<br />
31. Wasay M, Kheleani BA, Moolani MK, et al. Brain<br />
CT and MRI findings in 100 consecutive patients<br />
with intracranial tuberculoma. J Neuroimaging.<br />
2003;13:240-247.<br />
32. DeCarli C, Civitello LA, Brouwers P, et al. The<br />
prevalence of computed tomographic abnormalities<br />
of the cerebrum in 100 consecutive children symptomatic<br />
with the human immune deficiency virus. Ann<br />
Neurol. 1993;34:198-205.<br />
33. Caldemeyer KS, Mathews VP, Edwards-Brown<br />
MK, Smith RR. Central nervous system cryptococcosis:<br />
Parenchymal calcification and large gelatinous<br />
pseudocysts. AJNR Am J Neuroradiol. 1997;<br />
18:107-109.<br />
34. Tien RD, Chu PK, Hesselink JR, et al. <strong>Intracranial</strong><br />
cryptococcosis in immunocompromised patients:<br />
CT and MR findings in 29 cases. AJNR Am J<br />
Neuroradiol. 1991;12:283-289.<br />
35. Raymond AA, Zariah AA, Samad SA, et al. Brain<br />
calcification in patients with cerebral lupus. Lupus.<br />
1996;5:123-128.<br />
60 ■ APPLIED RADIOLOGY ©<br />
36. Ricci P. Imaging of adult brain tumors. Neuroimaging<br />
Clin N Am. 1999;9:651-669.<br />
37. Okuchi K, Hiramatsu K, Morimoto T, et al. Astrocytoma<br />
with widespread calcification along axonal<br />
fibers. Neuroradiology. 1992;34:328-330.<br />
38. Luh YG, Bird CR. Imaging of the brain tumors in<br />
the pediatric population. Neuroimaging Clin N Am.<br />
1999;9:691-716.<br />
39. Smirniotopoulos JG. The new WHO classification<br />
of brain tumors. Neuroimaging Clin N Am.<br />
1999;9:595-613.<br />
40. Vonofakos D, Marcu H, Hacker H. Oligodendrogliomas:<br />
CT patterns with emphasis on features<br />
indicating malignancy. J Comput Assist Tomogr.<br />
1979;3:783-788.<br />
41. Reiche W, Grunwald I, Hermann K, et al. Oligodendrogliomas.<br />
Acta Radiol. 2002;43:474-482.<br />
42. Brunette WC, Nesbit GM, Hall F. Pathologic correlation<br />
in oligodendroglioma. Int J Neuroradiol.<br />
1997;3:503.<br />
43. Meyers SP, Kemp SS, Tarr RW. MR imaging<br />
features of medulloblastomas. AJR Am J<br />
Roentgenol. 1992;158:859-865.<br />
44. Peretti-Viton P, Perez-Castillo AM, Raybaud C,<br />
et al. Magnetic resonance imaging in gangliogliomas<br />
and gangliocytomas of the nervous system. J Neuroradiol.<br />
1991;18:189-199.<br />
45. Zentner J, Wolf HK, Ostertun B, et al. Gangliogliomas:<br />
Clinical, radiological, and histopathological<br />
findings in 51 patients. J Neurol Neurosurg<br />
Psychiatry. 1994;57:1497-1502.<br />
46. Castillo M, Davis PC, Takei Y, Hoffman JC.<br />
<strong>Intracranial</strong> ganglioglioma: MR, CT, and clinical findings<br />
in 18 patients. AJNR Am J Neuroradiol.<br />
1990;11:109-114.<br />
47. Ostertun B, Wolf HK, Campos MG, et al. Dysembryoplastic<br />
neuroepithelial tumors: MR and CT evaluation.<br />
AJNR Am J Neuroradiol. 1996;17:419-430.<br />
48. Tomita T, Larsen MB. Calcified metastases to<br />
the brain in a child: Case report. Neurosurgery.<br />
1983;13:435-437.<br />
49. Sastre-Garriga J, Tintore M, Montaner J, et al.<br />
Calcified cerebral metastases. Study of two cases<br />
and review of the literature. Neurologia. 2000;15:<br />
136-139.<br />
50. Kizana E, Lee R, Young N, et al. A review of the<br />
radiological features of intracranial meningiomas.<br />
Australas Radiol. 1996;40:454-462.<br />
51. Hope JK, Armstrong DA, Babyn PS, et al. Primary<br />
meningeal tumors in children: Correlation of<br />
clinical and CT findings with histologic type and prognosis.<br />
AJNR Am J Neuroradiol. 1992;13:1353-1364.<br />
52. Chiechi MV, Smirniotopoulos JG, Mena H.<br />
Pineal parenchymal tumors: CT and MR features.<br />
J Comput Assist Tomogr. 1995;19:509-517.<br />
53. Zee CS, Segall H, Apuzzo M, et al. MR imaging<br />
of pineal region neoplasms. J Comput Assist<br />
Tomogr. 1991;15:56-63.<br />
54. Tsuda M, Takahashi S, Higano S, et al. CT and<br />
MR imaging of craniopharyngioma. Eur Radiol.<br />
1997;7:464-469.<br />
55. Gao PY, Osborn AG, Smirniotopoulos JG, Harris<br />
CP. Radiologic-pathologic correlation. Epidermoid<br />
tumor of the cerebellopontine angle. AJNR Am J<br />
Neuroradiol. 1992;13:863-872.<br />
56. Fujimaki T, Matsutani M, Funada N, et al. CT and<br />
MRI features of intracranial germ cell tumors. J Neurooncol.<br />
1994;19:217-226.<br />
57. Kinoshita Y, Yasukouchi H, Tsuru E, Yamaguchi<br />
R. Case report of Rosai-Dorfman disease mimicking<br />
pachymeningitis. No Shinkei Geka. 2004;32:<br />
1051-1056.<br />
58. Tamaki T, Takumi I, Kitamura T, et al. Pituitary<br />
stone—case report. Neurol Med Chir. (Tokyo) 2000;<br />
40:383-386.<br />
59. Dean B, Drayer BP, Beresini DC, Bird CR. MR<br />
imaging of pericallosal lipoma. AJNR Am J Neuroradiol.<br />
1988;9:929-931.<br />
60. Truwit CL, Barkovich AJ. Pathogenesis of<br />
intracranial lipoma: An MR study in 42 patients. AJR<br />
Am J Roentgenol. 1990;155:855-864.<br />
61. Ganti SR, Antunes JL, Louis KM, Hilal SK. Computed<br />
tomography in the diagnosis of colloid cysts of<br />
the third ventricle. <strong>Radiology</strong>. 1981;138:385-391.<br />
62. Koeller KK, Sandberg GD; Armed Forces Institute<br />
of Pathology. From the archives of the AFIP.<br />
Cerebral intraventricular neoplasms: Radiologicpathologic<br />
correlation. Radiographics. 2002;22:<br />
1473-1505.<br />
63. Van Tassel P, Lee YY, Bruner JM. Supratentorial<br />
ependymomas: Computed tomographic and pathologic<br />
correlations. J Comput Tomogr. 1986;10:<br />
157-165.<br />
64. Swartz JD, Zimmerman RA, Bilaniuk LT. Computed<br />
tomography of intracranial ependymomas.<br />
<strong>Radiology</strong>. 1982;143:97-101.<br />
65. Chiechi MV, Smirniotopoulos JG, Jones RV.<br />
<strong>Intracranial</strong> subependymomas: CT and MR imaging<br />
features in 24 cases. AJR Am J Roentgenol.<br />
1995;165:1245-1250.<br />
66. Furie DM, Provenzale JM. Supratentorial<br />
ependymomas and subependymomas: CT and<br />
MR appearance. J Comput Assist Tomogr. 1995;19:<br />
518-526.<br />
67. Goergen SK, Gonzales MF, McLean CA. Interventricular<br />
neurocytoma: Radiologic features and<br />
review of the literature. <strong>Radiology</strong>. 1992;182:<br />
787-792.<br />
68. Yasargil MG, von Ammon K, von Deimling, et al.<br />
Central neurocytoma: Histopathological variants and<br />
therapeutic approaches. J Neurosurg. 1992;76:<br />
32-37.<br />
69. Swartz JD, Faerber EN, Singh N, Polinsky MS.<br />
CT demonstration of cerebral subcortical <strong>calcifications</strong>.<br />
J Comput Assist Tomogr. 1983;7:476-478.<br />
70. Karimi M, Habibzadeh F, De Sanctis V.<br />
Hypoparathyroidism with extensive intracerebral calcification<br />
in patients with beta-thalassemia major.<br />
J Pediatr Endocrinol Metab. 2003;16:883-886.<br />
71. Fujita T. Mechanism of intracerebral calcification<br />
in hypoparathyroidism. Clin Calcium. 2004;14:<br />
55-57.<br />
72. Ogi S, Fukumitsu N, Tsuchida D, et al. Imaging<br />
of bilateral striopallidodentate calcinosis. Clin Nucl<br />
Med. 2002;27:721-724.<br />
73. Sue CM, Crimmins DS, Soo YS, et al. Neuroradiological<br />
features of six kindreds with MELAS<br />
tRNA(Leu) A2343G point mutation: Implications for<br />
pathogenesis. J Neurol Neurosurg Psychiatry.<br />
1998;65:233-240.<br />
www.appliedradiology.com November 2009