Cerebral herniations - Applied Radiology Online
Cerebral herniations - Applied Radiology Online
Cerebral herniations - Applied Radiology Online

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
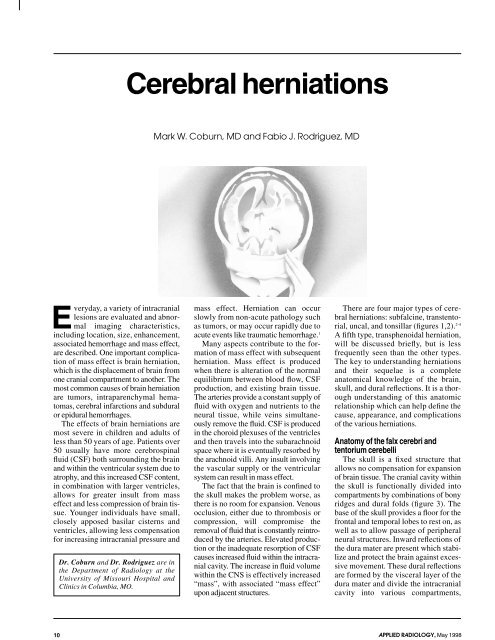
E veryday,<br />
a variety of intracranial<br />
lesions are evaluated and abnormal<br />
imaging characteristics,<br />
including location, size, enhancement,<br />
associated hemorrhage and mass effect,<br />
are described. One important complication<br />
of mass effect is brain herniation,<br />
which is the displacement of brain from<br />
one cranial compartment to another. The<br />
most common causes of brain herniation<br />
are tumors, intraparenchymal hematomas,<br />
cerebral infarctions and subdural<br />
or epidural hemorrhages.<br />
The effects of brain <strong>herniations</strong> are<br />
most severe in children and adults of<br />
less than 50 years of age. Patients over<br />
50 usually have more cerebrospinal<br />
fluid (CSF) both surrounding the brain<br />
and within the ventricular system due to<br />
atrophy, and this increased CSF content,<br />
in combination with larger ventricles,<br />
allows for greater insult from mass<br />
effect and less compression of brain tissue.<br />
Younger individuals have small,<br />
closely apposed basilar cisterns and<br />
ventricles, allowing less compensation<br />
for increasing intracranial pressure and<br />
Dr. Coburn and Dr. Rodriguez are in<br />
the Department of <strong>Radiology</strong> at the<br />
University of Missouri Hospital and<br />
Clinics in Columbia, MO.<br />
<strong>Cerebral</strong> <strong>herniations</strong><br />
Mark W. Coburn, MD and Fabio J. Rodriguez, MD<br />
mass effect. Herniation can occur<br />
slowly from non-acute pathology such<br />
as tumors, or may occur rapidly due to<br />
acute events like traumatic hemorrhage. 1<br />
Many aspects contribute to the formation<br />
of mass effect with subsequent<br />
herniation. Mass effect is produced<br />
when there is alteration of the normal<br />
equilibrium between blood flow, CSF<br />
production, and existing brain tissue.<br />
The arteries provide a constant supply of<br />
fluid with oxygen and nutrients to the<br />
neural tissue, while veins simultaneously<br />
remove the fluid. CSF is produced<br />
in the choroid plexuses of the ventricles<br />
and then travels into the subarachnoid<br />
space where it is eventually resorbed by<br />
the arachnoid villi. Any insult involving<br />
the vascular supply or the ventricular<br />
system can result in mass effect.<br />
The fact that the brain is confined to<br />
the skull makes the problem worse, as<br />
there is no room for expansion. Venous<br />
occlusion, either due to thrombosis or<br />
compression, will compromise the<br />
removal of fluid that is constantly reintroduced<br />
by the arteries. Elevated production<br />
or the inadequate resorption of CSF<br />
causes increased fluid within the intracranial<br />
cavity. The increase in fluid volume<br />
within the CNS is effectively increased<br />
“mass”, with associated “mass effect”<br />
upon adjacent structures.<br />
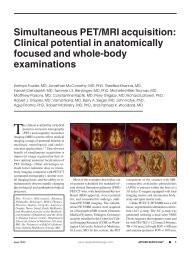
There are four major types of cerebral<br />
<strong>herniations</strong>: subfalcine, transtentorial,<br />
uncal, and tonsillar (figures 1,2). 2-4<br />
A fifth type, transphenoidal herniation,<br />
will be discussed briefly, but is less<br />
frequently seen than the other types.<br />
The key to understanding <strong>herniations</strong><br />
and their sequelae is a complete<br />
anatomical knowledge of the brain,<br />
skull, and dural reflections. It is a thorough<br />
understanding of this anatomic<br />
relationship which can help define the<br />
cause, appearance, and complications<br />
of the various <strong>herniations</strong>.<br />
Anatomy of the falx cerebri and<br />
tentorium cerebelli<br />
The skull is a fixed structure that<br />
allows no compensation for expansion<br />
of brain tissue. The cranial cavity within<br />
the skull is functionally divided into<br />
compartments by combinations of bony<br />
ridges and dural folds (figure 3). The<br />
base of the skull provides a floor for the<br />
frontal and temporal lobes to rest on, as<br />
well as to allow passage of peripheral<br />
neural structures. Inward reflections of<br />
the dura mater are present which stabilize<br />
and protect the brain against excessive<br />
movement. These dural reflections<br />
are formed by the visceral layer of the<br />
dura mater and divide the intracranial<br />
cavity into various compartments,<br />
10 APPLIED RADIOLOGY, May 1998
FIGURE 1. Patterns of brain herniation,<br />
coronal drawing. (1) Subfalcine herniation<br />
of the cingulate gyrus beneath the falx<br />
cerebri; (2) compression of ipsilateral lateral<br />
ventricle due to subfalcine herniation;<br />
(3) dilatation of the contralateral ventricle<br />
due to obstruction of the foramen of Monro;<br />
(4) uncal herniation through the tentorial<br />
notch; (5) tentorium cerebelli; (6) tonsillar<br />
herniation through the foramen magnum;<br />
(7) transverse sinus within the tentorium<br />
cerebelli; (8) superior sagittal sinus within<br />
the falx cerebri. (Adapted from Bassett DL:<br />
A Stereoscopic Atlas of Human Anatomy.)<br />
known as the falx cerebri, the tentorium<br />
cerebelli, and the falx cerebelli.<br />
Anteriorly, the falx cerebri is<br />
attached to the crista galli, from where<br />
it extends midline along the skull’s<br />
inner table to the confluence of sinuses<br />
(torcular herophili) posteriorly. It is narrow<br />
anteriorly and broad posteriorly,<br />
where it connects with the upper surface<br />
of the tentorium cerebelli. 5 The<br />
falx cerebri contains the superior sagittal<br />
sinus along its upper margin and the<br />
inferior sagittal sinus along its inferior<br />
margin. 5 The superior sagittal sinus<br />
drains directly into the sinus confluence,<br />
the inferior sagittal sinus drains<br />
into the straight sinus. As the falx cerebri<br />
courses posteriorly, it elongates in<br />
its craniocaudad dimension and forms a<br />
larger barrier between the hemispheres<br />
(figure 3). The increased size of the<br />
posterior portion of the falx cerebri<br />
makes it more resistant to movement<br />
than the anterior falx cerebri. It is for<br />
this reason that subfalcine <strong>herniations</strong><br />
more commonly occur anteriorly.<br />
APPLIED RADIOLOGY, May 1998<br />
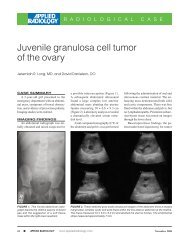
FIGURE 2. Patterns of brain herniation, sagittal drawing. (1) Ascending transtentorial herniation;<br />
(2) associated obstruction of the cerebral aqueduct; (3) tentorium cerebelli; (4) fourth<br />
ventricle; (5) tonsillar herniation through the foramen magnum.<br />
FIGURE 3. Dural reflections. (1) Falx cerebri; (2) tentorium cerebelli; (3) superior sagittal<br />
sinus within the falx cerebri; (4) inferior sagittal sinus within the falx cerebri; (5) straight sinus<br />
within the tentorium cerebelli; (6) transverse sinus within the tentorium cerebelli; (7) confluence<br />
of sinuses (torcular herophili); (8) anterior attachment of falx cerebri to the crista galli;<br />
(9) black arrows demonstrate the free edges of the tentorial notch; (10) anterior clinoid<br />
process. (Adapted from Wilkins RH, Rengachery SS: Neurosurgery, ed 2, pp 349-350. New<br />
York, McGraw-Hill, 1989.)<br />
11
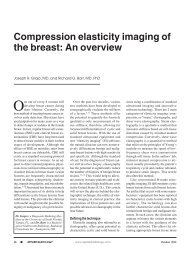
FIGURE 4. Subfalcine herniation. Note<br />
extensive midline shift due to the acute and<br />
chronic subdural hematoma. There is compression<br />
of the ipsilateral ventricle due to<br />
mass effect. The frontal and temporal horns<br />
of the contralateral ventricle are dilated due<br />
to foramen of Monro obstruction and continued<br />
CSF production. Also note the compression<br />
upon the quadrigeminal cistern<br />
causing a “crooked smile.”<br />
The tentorium cerebelli creates a<br />
compartment between the posterior<br />
fossa and the cerebral hemispheres. It is<br />
attached to the occipital bone posteriorly,<br />
the petrous portions of the temporal<br />
bones laterally, and the clinoid<br />
processes anteriorly; it courses superomedially<br />
from its bony attachments to<br />
join the falx cerebri. The tentorium cerebelli<br />
contains the transverse sinuses,<br />
which eventually course through the<br />
skull base, and the straight sinus, which<br />
empties into the sinus confluence. 5<br />
The tentorium cerebelli contains an<br />
opening anteriorly that allows passage<br />
of the brain stem and cerebral peduncles<br />
(figure 3). This opening is known as the<br />
tentorial hiatus, tentorial notch, or<br />
incisura and measures approximately<br />
5.5 cm in the fronto-occipital axis and<br />
3 cm in the interparietal axis. 6 The tentorial<br />
notch is semiovular in shape and its<br />
only bony attachment is at the clinoid<br />
processes anteriorly. 5 The remaining lateral<br />
and posterior borders of the tentorial<br />
notch are the “free edges.” These are<br />
without direct attachment, but are taut<br />
and firm nonetheless.<br />
A<br />
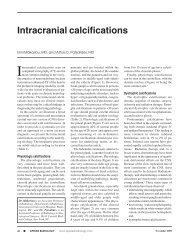
FIGURE 5. Unilateral descending transtentorial herniation due to a right-sided glioblastoma.<br />
Image A is approximately 1 cm inferior to B. (A) The inferior tip of the herniated right parahippocampal<br />
gyrus with mild mass effect upon the brainstem is demonstrated. (B) Also demonstrated<br />
is herniation of the right parahippocampal gyrus t through the tentorial notch, with<br />
displacement of the brainstem to the left and obliteration of the perimesencephalic cisterns.<br />
Notice that the inferior aspect of the third ventricle can be seen immediately superior to the<br />
midline of the midbrain. Dilatation of the contralateral lateral ventricle is present due to the<br />
concomitant subfalcine herniation.<br />
Obviously, a herniation is a critical<br />
finding that reflects evidence of a pathologic<br />
process and the need for possible<br />
emergent intervention. It is imperative<br />
to not only report the presence of a herniation,<br />
but to also evaluate for possible<br />
complications. Such complications<br />
may result from compression upon<br />
adjacent arteries, veins, nerves and<br />
brain parenchyma.<br />
Subfalcine herniation<br />
A subfalcine herniation, or midline<br />
shift, occurs when mass effect causes displacement<br />
of the falx cerebri laterally<br />
(figure 4). It is the most common type of<br />
brain herniation and is often associated<br />
with herniation of the cingulate gyrus<br />
below the falx cerebri. The cingulate<br />
gyrus of each cerebral hemisphere normally<br />
lies medial to the inferior aspect of<br />
the falx cerebri (figure 1).<br />
The degree of herniation can be mild<br />
with minimal midline shift or can be<br />
severe, exhibiting complete herniation of<br />
the cingulate gyrus and adjacent white<br />
matter. Due to the tough fibrous structure<br />
of the falx and its resistance to move-<br />
B<br />
ment, a few millimeters of midline shift<br />
is considered significant. With increasing<br />
mass effect, the ipsilateral lateral ventricle<br />
and both foramina of Monro become<br />
compressed. This compression results in<br />
a slit-like appearance of the ipsilateral<br />
ventricle and an enlarged contralateral<br />
ventricle. This enlargement is due to continued<br />
production of CSF that cannot<br />
escape into the third ventricle. 7 Chronic<br />
compression upon the cingulate gyrus<br />
may cause necrosis. 1<br />
The anterior cerebral arteries and their<br />
branches (the callosomarginal, pericallosal,<br />
and frontopolar arteries) are<br />
located between the falx cerebri and the<br />
adjacent gyri of the frontal and parietal<br />
lobes. When subfalcine herniation is<br />
present there is the possibility of anterior<br />
cerebral artery compression, 8,9 especially<br />
when an anterior lesion also is present. If<br />
these vessels become trapped against the<br />
falx, the patient may be at risk of infarction.<br />
10 Formation of an aneurysm due to<br />
vascular damage is another unusual complication<br />
of compression of the anterior<br />
cerebral arteries by the falx cerebri that<br />
may be present. 11<br />
12 APPLIED RADIOLOGY, May 1998
FIGURE 6. Bilateral descending transtentorial<br />
herniation in a 12-year-old who was hit<br />
by a car and died shortly after the CT scan<br />
was performed. Both parahippocampal gyri<br />
have herniated downward through the<br />
transtentorial notch. The perimesencephalic<br />
cisterns are obliterated and the brainstem is<br />
elongated. Note the ischemic “reversal sign”<br />
manifested by higher density in the cerebellum<br />
than the cerebral hemispheres, due to<br />
massive supratentorial edema.<br />
When the lesion is located posteriorly<br />
in the hemisphere, there may be compression<br />
of the internal cerebral veins, 9 vein of<br />
Galen, or the deep subependymal veins.<br />
Compression of these veins raises the<br />
pressure of the entire deep venous system,<br />
which further aggravates parenchymal<br />
congestion and increases intracranial<br />
pressure (ICP). 12 When a subfalcine herniation<br />
is present, the concomitant presence<br />
of a transtentorial or uncal herniation also<br />
should be evaluated. 1<br />
Transtentorial herniation<br />
Transtentorial herniation is due to<br />
mass effect that causes shift of neural<br />
components into the tentorial notch.<br />
There are three separate types of <strong>herniations</strong><br />
which cross the tentorium<br />
cerebelli. Descending and ascending<br />
transtentorial herniation will be discussed<br />
here, and uncal herniation, a subtype<br />
of a transtentorial herniation, will<br />
be discussed separately.<br />
There is limited space within the tentorial<br />
notch, which contains the brain<br />
APPLIED RADIOLOGY, May 1998<br />
FIGURE 7. Midbrain/parahippocampus. <strong>Cerebral</strong> peduncles and adjacent structures.<br />
(1) Uncus of parahippocampal gyrus; (2) parahippocampal gyrus; (3) ambient cistern;<br />
(4) quadrigeminal cistern; (5) posterior cerebral artery in the ambient cistern; (6) middle cerebral<br />
artery; (7) anterior cerebral artery; (8) posterior communicating artery; (9) oculomotor<br />
nerve (CN3).<br />
stem and its surrounding subarachnoid<br />
cisterns. Only a few millimeters of<br />
space are present between the midbrain<br />
and the rigid tentorial edge. 13 Therefore,<br />
much lateral displacement of the brainstem<br />
cannot be tolerated, and a shift<br />
from the midline of a few millimeters<br />
will result in compression. 14-16 Both<br />
ascending and descending herniation<br />
can produce enough pressure on the<br />
brainstem to produce cerebral aqueduct<br />
occlusion (figure 2). 1 When this occurs,<br />
it results in obstructive hydrocephalus<br />
supratentorially, which compounds the<br />
problem by increasing ICP. 14 Eventually,<br />
the increasing compression upon the<br />
brainstem compromises the cardiorespiratory<br />
centers, which can be fatal.<br />
Descending<br />
Descending transtentorial herniation<br />
occurs when mass effect displaces the<br />
medial part of the temporal lobe<br />
through the tentorial notch. Specifically,<br />
it is the middle and posterior<br />
portions of the parahippocampal gyrus<br />
that herniate and compress the brainstem.<br />
17 Descending transtentorial herniation<br />
is commonly seen with masses<br />
involving the inferior portion of a<br />
hemisphere. This increase in mass<br />
effect forces the diencephalon and midbrain<br />
inferiorly through the tentorial<br />
notch (figure 5). 3 The herniated<br />
parahippocampal gyrus generally is<br />
unilateral, but has also been found to be<br />
bilateral. 1 Bilateral herniation is commonly<br />
produced by a midline mass,<br />
bilateral mass, or supratentorial hydrocephalus<br />
whose vector forces are<br />
directed inferiorly and medially (figure<br />
6). 18 Transtentorial herniation commonly<br />
is associated with a concomitant<br />
subfalcine herniation. 1<br />
13
FIGURE 8. Ascending transtentorial and<br />
tonsillar <strong>herniations</strong> due to medulloblastoma.<br />
Gadolinium-enhanced T1weighted<br />
image demonstrates that the<br />
superior portions of the cerebellum have<br />
herniated through the tentorial notch. The<br />
brainstem is compressed, showing displacement<br />
both superiorly and anteriorly.<br />
Supratentorial hydrocephalus is present<br />
due to cerebral aqueduct compression. The<br />
cerebellar tonsils have herniated below the<br />
foramen magnum and also exhibit compression<br />
of the medulla. There is near obliteration<br />
of the fourth ventricle.<br />
In severe cases of descending<br />
transtentorial herniation, there is obliteration<br />
of all basilar cisterns. When displaced<br />
inferiorly, the parahippocampal<br />
gyrus compresses regions of the midbrain,<br />
including the cerebral aqueduct.<br />
Increasing herniation will then sequentially<br />
compress the pons and, subsequently,<br />
the medulla. 19 Often, acute<br />
compression of the entire brain stem<br />
occurs simultaneously due to the acute<br />
and catastrophic nature of the lesion.<br />
The midbrain is surrounded laterally<br />
by the ambient cisterns, posteriorly by<br />
the quadrigeminal cistern, and anteriorly<br />
by the interpeduncular and<br />
suprasellar cisterns (figure 7). These<br />
cisterns serve as corridors for the passage<br />
of the posterior cerebral arteries<br />
and the third cranial nerves. Each third<br />
cranial nerve courses through the<br />
interpeduncular cistern below the posterior<br />
cerebral artery.<br />
To a variable extent, the herniated<br />
temporal lobe can compress the oculomotor<br />
nerve, the posterior cerebral<br />
artery, the anterior choroidal artery, and<br />
the superior cerebellar artery. 20 Compression<br />
of the oculomotor nerve produces<br />
ipsilateral pupillary dilatation.<br />
Compression of the posterior cerebral<br />
artery between the temporal lobe and<br />
tentorial edge results in infarction. Both<br />
posterior cerebral arteries may become<br />
compressed if bilateral herniation is<br />
present. 21 Occlusion of the anterior<br />
choroidal artery results in infarction of<br />
the structures in its vascular supply,<br />
which include the optic tract, temporal<br />
lobe, basal ganglia, cerebral peduncles,<br />
and midbrain. 22 Cerebellar infarction<br />
will occur if the superior cerebellar<br />
artery is compressed.<br />
In severe cases of transtentorial herniation,<br />
a Duret hemorrhage may occur. This<br />
is a brainstem hemorrhage caused by<br />
mechanical shearing of the pontine<br />
and mesencephalic perforating vessels,<br />
especially the arterials, by the herniating<br />
tissue. 23,24 Compression related to Duret<br />
hemorrhage may compromise the cardiorespiratory<br />
centers, resulting in death. 3,25<br />
Transtentorial herniation is a grim<br />
finding as it usually is an acute process<br />
which is lethal in a very short time. In<br />
unilateral descending transtentorial herniation,<br />
the brainstem is shifted away<br />
from the herniating temporal lobe,<br />
resulting in enlargement of the ipsilateral<br />
cerebellopontine angle cistern. 7 In<br />
this instance, the brainstem will appear<br />
flattened and elongated, with compressed<br />
or obliterated perimesencephalic<br />
cisterns.<br />
Ascending<br />
Ascending transtentorial herniation is<br />
due to increased pressure in the posterior<br />
fossa. This increase in pressure projects<br />
the central lobule, culmen, and<br />
superior surface of the cerebellum<br />
upward through the tentorial notch,<br />
resulting in compression of the brain<br />
stem (figure 2). 7 This brainstem displacement<br />
is well visualized on multiplanar<br />
magnetic resonance images.<br />
In ascending transtentorial herniation,<br />
the superior vermian cistern is effaced<br />
and the fourth ventricle is compressed<br />
and displaced anteriorly (figures 8,9). 7<br />
With increasing upward herniation, the<br />
quadrigeminal cistern becomes effaced<br />
and the midbrain displaced anteriorly<br />
against the clivus. 26,27 Increasing mass<br />
effect may occlude the cerebral aqueduct,<br />
resulting in increased intracranial<br />
pressure. 14 An ascending transtentorial<br />
herniation also is likely to obstruct<br />
venous outflow through direct compres-<br />
FIGURE 9. Ascending transtentorial herniation<br />
in the same patient as figure 8. This<br />
gadolinium-enhanced T1-weighted axial<br />
image is at the level of the cerebral peduncles.<br />
The cerebellum is enlarged and demonstrates<br />
compression of the quadrigeminal<br />
plate. The quadrigeminal cistern and posterior<br />
ambient cisterns are obliterated. The<br />
third and lateral ventricles are enlarged due<br />
to cerebral aqueduct compression.<br />
sion of the vein of Galen and the basal<br />
vein of Rosenthal, which further aggravates<br />
parenchymal congestion and<br />
increases the ICP. 12 Midbrain compression<br />
also may be complicated by periaqueductal<br />
necrosis of the brain stem.<br />
Uncal herniation<br />
Uncal herniation occurs when the<br />
uncus is displaced medially and inferiorly<br />
over the free edge of the tentorium cerebelli.<br />
2 The uncus is the hooked, anterior<br />
extension of the parahippocampal formation<br />
of the medial temporal lobe (figure<br />
7). Normally it is located 3 to 4 mm<br />
medial to the free edge of the tentorium,<br />
which is adjacent to the suprasellar cistern.<br />
28 In herniation, the uncal gyrus is displaced<br />
into the suprasellar cistern<br />
between the free edge of the tentorium<br />
and the anterior edge of the midbrain (figures<br />
10,11,12). 14 This type of herniation<br />
usually is secondary to a mass located<br />
more inferiorly in the cerebral hemisphere,<br />
such as in the temporal lobe.<br />
Uncal herniation often exhibits compression<br />
of one or both of the cerebral<br />
peduncles, as well as the adjacent oculomotor<br />
nerve. The oculomotor nerve is<br />
14 APPLIED RADIOLOGY, May 1998
FIGURE 10. Unilateral uncal herniation due<br />
to an intraparenchymal hematoma. The left<br />
uncus has herniated through the tentorial<br />
notch, evidenced by distortion of the<br />
suprasellar cistern. The normal “star” configuration<br />
has been disrupted. There is mild<br />
compression upon the ipsilateral cerebral<br />
peduncle, with associated tilting and displacement<br />
of the brainstem to the right. The<br />
right perimesencephalic cisterns are obliterated<br />
due to the brainstem displacement.<br />
located medial to the uncus and passes<br />
between the superior cerebellar artery<br />
and the posterior cerebral artery. 29 Mass<br />
effect upon the third cranial nerve and<br />
compression of the ipsilateral cerebral<br />
APPLIED RADIOLOGY, May 1998<br />
FIGURE 11. Unilateral uncal herniation.<br />
This axial CT image through the level of the<br />
4th ventricle demonstrates widening of the<br />
left cerebellopontine angle due to a left unilateral<br />
uncal herniation. The inferior tip of<br />
the left uncus can be seen anterolateral to<br />
the brainstem.<br />
peduncle causes a recognizable clinical<br />
syndrome, characterized by a blown<br />
pupil with contralateral hemiparesis. 10<br />
Alternatively, the uncus can displace the<br />
A<br />
B<br />
FIGURE 13. Tonsillar herniation. (A) An axial CT of a patient with a large cerebellar metastasis.<br />
(B) An axial T1-weighted image of the same patient with medulloblastoma in figure 8.<br />
Image shows that the foramen magnum is nearly completely filled with brain tissue, and virtually<br />
no CSF is seen. The brainstem is elongated and compressed bilaterally by the herniating<br />
cerebellar tonsils. This image demonstrates the similar findings, with an abnormally low<br />
position of the cerebellar tonsils and very little surrounding CSF.<br />
FIGURE 12. Bilateral uncal herniation due<br />
to traumatic injury. The normal “star” configuration<br />
is disrupted with inferomedial displacement<br />
of the uncus bilaterally.<br />
Associated cerebellar infarctions are seen<br />
due to compression of both superior cerebellar<br />
arteries.<br />
brain stem against the opposite tentorial<br />
edge and cause an indentation of the<br />
contralateral cerebral peduncle, known<br />
as Kernohan’s notch. 28,29 This contralateral<br />
compression causes ipsilateral<br />
hemiparesis, which falsely localizes the<br />
symptoms to the other side. 22<br />
Uncal herniation can compress the<br />
posterior cerebral artery as it encircles<br />
the cerebral peduncle anterolaterally;<br />
however, the risk of infarction is greater<br />
with transtentorial herniation due to a<br />
closer anatomic relationship between<br />
the parahippocampal gyrus and the<br />
posterior cerebral artery (figure 3).<br />
Additionally, there also can be compression<br />
upon the anterior choroidal artery<br />
and superior cerebellar artery, with<br />
resultant infarction.<br />
Imaging features of uncal herniation<br />
include distortion of the suprasellar cistern<br />
due to the medial and inferior position<br />
of the uncus. The normal<br />
suprasellar cistern has a “star”" configuration,<br />
but in uncal herniation the lateral<br />
aspect of the star is obliterated by the<br />
uncus. 30 The cerebral peduncle will<br />
appear flattened and the midbrain can be<br />
rotated or tilted. 1 The ipsilateral cerebel-<br />
15
lopontine angle cistern may be widened<br />
due to shift of the brainstem (figure 11).<br />
Tonsillar herniation<br />
Tonsillar herniation occurs when<br />
mass effect in the posterior fossa causes<br />
inferior displacement of the cerebellar<br />
tonsils into or beyond the foramen<br />
magnum (figures 1,2). 31 Two-thirds of<br />
patients with ascending transtentorial<br />
and one-half of those with descending<br />
transtentorial shift have concurrent tonsillar<br />
herniation (figures 8,13). 4<br />
Tonsillar herniation usually is not<br />
fatal; however, in rare cases, there can<br />
be significant compression upon the<br />
medulla which can be fatal. 1 Additionally,<br />
compression upon the posterior<br />
inferior cerebellar arteries can produce<br />
infarction. 10 The presence of a concomitant<br />
ascending transtentorial herniation<br />
must be evaluated because of its common<br />
association and clinical importance.<br />
Tonsillar herniation can obstruct<br />
CSF outflow from the fourth ventricle,<br />
resulting in hydrocephalus. 1<br />
Tonsillar herniation is difficult to accurately<br />
characterize on axial CT images.<br />
However, the demonstration of brain<br />
parenchyma around the medulla in the<br />
foramen magnum and a less than adequate<br />
amount of CSF in the foramen magnum<br />
(figure 13) may provide clues to its<br />
presence. 22 Although sagittal MR images<br />
have been found to be the best method for<br />
evaluating tonsillar herniation, direct or<br />
reconstructed coronal CT images also<br />
will demonstrate an abnormal inferior<br />
location of the cerebellar tonsils.<br />
It is important to know not to perform<br />
a lumbar puncture in the presence of significant<br />
herniation, especially a transtentorial<br />
or tonsillar herniation. The<br />
withdrawal of CSF will decrease the<br />
pressure below the foramen magnum,<br />
allowing further herniation inferiorly.<br />
This can increase compression upon the<br />
brain stem suddenly, often resulting<br />
in death due to cardiorespiratory center<br />
compromise. 32<br />
Transphenoidal (transalar) herniation<br />
Transphenoidal herniation is found<br />
when mass effect displaces brain tissue<br />
across the sphenoid wing. There are<br />
two types of transphenoidal herniation,<br />
ascending and descending, which<br />
involve the temporal lobe and frontal<br />
lobe, respectively. Descending herniation<br />
occurs when the frontal lobe is<br />
forced posteriorly over the greater sphenoid<br />
wing, causing backward displacement<br />
of the sylvian fissure, the<br />
horizontal middle cerebral artery, and<br />
the temporal lobe. This type of herniation,<br />
caused by a lesion in the anterior<br />
frontal lobe, can lead to ischemic<br />
changes in the inferior frontal lobe. 1<br />
Ascending herniation occurs when the<br />
temporal lobe, sylvian fissure, and middle<br />
cerebral artery are displaced anterosuperiorly<br />
over the sphenoid ridge by all<br />
adjacent mass.<br />
Summary<br />
Complications due to mass effect are<br />
commonly seen. It is extremely important<br />
to not only describe an inciting<br />
mass lesion, but also to comment on any<br />
associated complications such as cerebral<br />
herniation. The type of herniation<br />
and any associated complications are<br />
important to the clinician to help assess<br />
therapeutic options and the possible<br />
need for emergent intervention. AR<br />
REFERENCES<br />
1. Taveras JM: Neuroradiology, ed 3, pp 111-115.<br />
Baltimore, Williams & Wilkins, 1996.<br />
2. Meyer A: Herniation of the brain. Arch Neurol<br />
Psychiatr 4:387-400, 1920.<br />
3. Scheinker IM: Transtentorial herniation of the<br />
brainstem; A characteristic clinicopathologic syndrome;<br />
Pathogenesis of hemorrhages in the brainstem.<br />
Arch Neurol Psychiatr 53:289-298, 1945.<br />
4. Reich JB, Sierra J, Camp W, et al: Magnetic resonance<br />
imaging measurements and clinical changes<br />
accompanying transtentorial and foramen magnum<br />
brain herniation. Ann Neurol 33:159-170, 1993.<br />
5. Gray H: Gray’s Anatomy, pp 512-523. Philadelphia,<br />
Running Press, 1974.<br />
6. Sunderland S: The tentorial notch and complications<br />
produced by <strong>herniations</strong> of the brain through<br />
that aperture. Br J Surg 455:422-438, 1958.<br />
7. Osborn AG: Handbook of Neuroradiology:<br />
Brain and Skull, ed 2, pp 222-230. St. Louis,<br />
Mosby, 1996.<br />
8. Hassler O: Arterial pattern of human brainstem:<br />
Normal appearance and deformation in expanding<br />
supratentorial conditions. Neurology 17:1-6, 1967.<br />
9. Sohn D, Levine S: Frontal lobe infarcts caused<br />
by brain herniation: Compression of anterior cerebral<br />
artery branches. Arch Pathol Lab Med 84:509-<br />
512, 1967.<br />
10. Barr R, Gean AD: Trauma. In: Brandt WE,<br />
Helms CA: Fundamentals of Diagnostic <strong>Radiology</strong>,<br />
pp 65-68. Baltimore, Williams & Wilkins, 1994.<br />
11. Nakstad P, Nornes H, Hauge HN: Traumatic<br />
aneurysms of the pericallosal arteries. Neuroradiology<br />
28:335-338, 1986.<br />
12. Ecker A: Upward transtentorial herniation of<br />
the brainstem and cerebellum due to tumor of the<br />
posterior fossa: With a special note on tumors of<br />
acoustic nerve. J Neurosurg 5:51-61, 1948.<br />
13. Elguera M: Transtentorial Herniation, Finney<br />
LA, Walker AE (eds). Springfield, IL, Charles C.<br />
Thomas, 1962.<br />
14. Schwarz GA, Rosner AA: Displacement and<br />
herniation of the hippocampal gyrus through the<br />
incisura tentorii. Arch Neurol Psychiatry 46:297-<br />
321, 1941.<br />
15. Jefferson G: The tentorial pressure cone. Arch<br />
Neurol Psychiatr 40:857-876, 1938.<br />
16. Smyth GE, Henderson WR: Observations on<br />
the cerebrospinal fluid pressure on simultaneous<br />
ventricular and lumbar punctures. J Neurol Psychiatr<br />
1:226-238, 1938.<br />
17. Stovring J: Descending tentorial <strong>herniations</strong>:<br />
Findings on computed tomography. Neuroradiology<br />
14:101-106, 1977.<br />
18. Hahn F, Gurney J: CT signs of central<br />
descending transtentorial herniation. AJNR 6:844-<br />
845, 1985.<br />
19. Feldmann E, Gandy SE, Becker R, et al: MRI<br />
demonstrates descending transtentorial herniation.<br />
Neurology 38:697-701, 1988.<br />
20. Blinkov SM, Gabibov GA, Tanyashin SV:<br />
Variations in location of the arteries coursing<br />
between the brain stem and the free edge of the<br />
tentorium. J Neurosurg 76:973-978, 1992.<br />
21. Komaki S, Handel S: Molding of the posterior<br />
communicating artery in downward transtentorial<br />
herniation. <strong>Radiology</strong> 113:107-119, 1974.<br />
22. Grossman RI, Yousem DM: Trauma. In: Neuroradiology<br />
- The Requisites, pp 161-162. St.<br />
Louis, Mosby-Year Book, Inc., 1994.<br />
23. Fisher CM: The arterial source of secondary<br />
brain stem hemorrhages (abstr). J Pathol 66:9a,<br />
1972.<br />
24. Thompson RK, Salcman M: Brain stem hemorrhages:<br />
historical perspective. Neurosurgery 22:<br />
623-628, 1988.<br />
25. Howell DA: Longitudinal brain stem compression<br />
with buckling. Arch Neurol 4:572-579, 1961.<br />
26. Osborn AG: Secondary effects of intracranial<br />
trauma. Neurosurg Clin N Am 1:461-474, 1991.<br />
27. Speigelman R, Hadani M, Ram Z, et al:<br />
Upward transtentorial herniation: A complication of<br />
postoperative edema at the cervicomedullary junction.<br />
Neurosurg 24:284-288, 1989.<br />
28. Cohen D, Quest D: Increased intracranial<br />
pressure, brain herniation. In: Wilkins RH, Rengachary<br />
SS (eds): Neurosurgery, ed 2, pp 349-<br />
350. New York, McGraw-Hill, 1996.<br />
29. Kernohan JW, Woltman HW: Incisura of the<br />
crus due to contralateral brain tumor. Arch Neurol<br />
Psychiatry 21:274-287, 1929.<br />
30. Osborn, AG: Diagnosis of descending<br />
transtentorial herniation by cranial computed<br />
tomography. <strong>Radiology</strong> 123:93-96, 1976.<br />
31. Ishikawa M, Kikuchi H, Fujisawa I,<br />
Yonekawa Y: Tonsillar herniation on magnetic resonance<br />
imaging. Neurosurgery 22:77-81, 1988.<br />
32. Ramsey RG: Disorders of the spine. In: Neuroradiology,<br />
ed 3, pp 42-43, 496. Philadelphia, WB<br />
Saunders, 1994.<br />
16 APPLIED RADIOLOGY, May 1998