Addiction Awareness OSCA 11-036 response - REDACTED.pdf
Addiction Awareness OSCA 11-036 response - REDACTED.pdf
Addiction Awareness OSCA 11-036 response - REDACTED.pdf

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
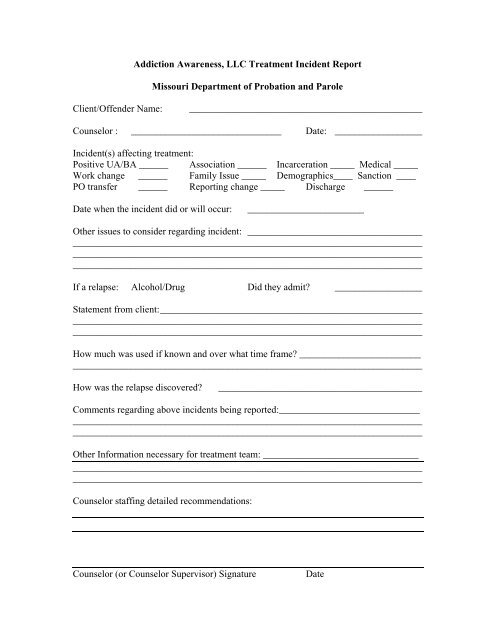
<strong>Addiction</strong> <strong>Awareness</strong>, LLC Treatment Incident Report<br />
Missouri Department of Probation and Parole<br />
Client/Offender Name:<br />
________________________________________________<br />
Counselor : _______________________________ Date: __________________<br />
Incident(s) affecting treatment:<br />
Positive UA/BA ______ Association ______ Incarceration _____ Medical _____<br />
Work change ______ Family Issue _____ Demographics____ Sanction ____<br />
PO transfer ______ Reporting change _____ Discharge ______<br />
Date when the incident did or will occur:<br />
________________________<br />
Other issues to consider regarding incident: ____________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
If a relapse: Alcohol/Drug Did they admit? __________________<br />
Statement from client: ______________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
How much was used if known and over what time frame? _________________________<br />
________________________________________________________________________<br />
How was the relapse discovered?<br />
__________________________________________<br />
Comments regarding above incidents being reported:_____________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
Other Information necessary for treatment team: ________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
Counselor staffing detailed recommendations:<br />
Counselor (or Counselor Supervisor) Signature<br />
Date