CDC Article-US Medical Eligibility Criteria for Contraceptive Use, 2010
CDC Article-US Medical Eligibility Criteria for Contraceptive Use, 2010
CDC Article-US Medical Eligibility Criteria for Contraceptive Use, 2010

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
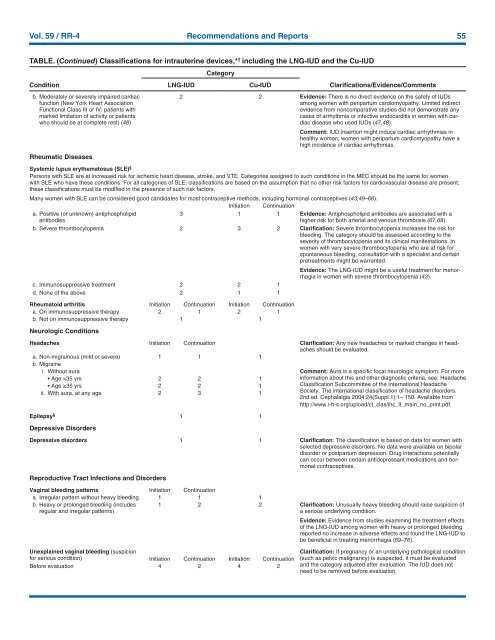
Vol. 59 / RR-4 Recommendations and Reports 55<br />
TABLE. (Continued) Classifications <strong>for</strong> intrauterine devices,* † including the LNG-IUD and the Cu-IUD<br />
Condition<br />
b. Moderately or severely impaired cardiac<br />
function (New York Heart Association<br />
Functional Class III or IV: patients with<br />
marked limitation of activity or patients<br />
who should be at complete rest) (46)<br />
Rheumatic Diseases<br />
LNG-IUD<br />
Category<br />
Cu-IUD<br />
Clarifications/Evidence/Comments<br />
2 2 Evidence: There is no direct evidence on the safety of IUDs<br />
among women with peripartum cardiomyopathy. Limited indirect<br />
evidence from noncomparative studies did not demonstrate any<br />
cases of arrhythmia or infective endocarditis in women with cardiac<br />
disease who used IUDs (47,48).<br />
Comment: IUD insertion might induce cardiac arrhythmias in<br />
healthy women; women with peripartum cardiomyopathy have a<br />
high incidence of cardiac arrhythmias.<br />
Systemic lupus erythematosus (SLE) §<br />
Persons with SLE are at increased risk <strong>for</strong> ischemic heart disease, stroke, and VTE. Categories assigned to such conditions in the MEC should be the same <strong>for</strong> women<br />
with SLE who have these conditions. For all categories of SLE, classifications are based on the assumption that no other risk factors <strong>for</strong> cardiovascular disease are present;<br />
these classifications must be modified in the presence of such risk factors.<br />
Many women with SLE can be considered good candidates <strong>for</strong> most contraceptive methods, including hormonal contraceptives (43,49–66).<br />
Initiation Continuation<br />
a. Positive (or unknown) antiphospholipid<br />
antibodies<br />
3 1 1 Evidence: Antiphospholipid antibodies are associated with a<br />
higher risk <strong>for</strong> both arterial and venous thrombosis (67,68).<br />
b. Severe thrombocytopenia 2 3 2 Clarification: Severe thrombocytopenia increases the risk <strong>for</strong><br />
bleeding. The category should be assessed according to the<br />
severity of thrombocytopenia and its clinical manifestations. In<br />
women with very severe thrombocytopenia who are at risk <strong>for</strong><br />
spontaneous bleeding, consultation with a specialist and certain<br />
pretreatments might be warranted.<br />
Evidence: The LNG-IUD might be a useful treatment <strong>for</strong> menorrhagia<br />
in women with severe thrombocytopenia (43).<br />
c. Immunosuppressive treatment 2 2 1<br />
d. None of the above 2 1 1<br />
Rheumatoid arthritis Initiation Continuation Initiation Continuation<br />
a. On immunosuppressive therapy 2 1 2 1<br />
b. Not on immunosuppressive therapy 1 1<br />
Neurologic Conditions<br />
Headaches Initiation Continuation Clarification: Any new headaches or marked changes in headaches<br />
should be evaluated.<br />
a. Non-migrainous (mild or severe) 1 1 1<br />
b. Migraine<br />
i. Without aura Comment: Aura is a specific focal neurologic symptom. For more<br />
• Age