

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
MD: And I bet most dentists know that on a certain<br />
level. They couldn’t give you numbers. They certainly<br />
couldn’t quantify it. But you might say to them,<br />
what’s your favorite thing to do? And they might say,<br />
“I like a good 3-unit bridge.” And we have 3 units<br />
here in the sweet spot, the profit per hour, but we’re<br />
only prepping 2 units, so that might be the sweet spot.<br />
You charge for the pontic, and life is good. Greatest<br />
determination ever: that we can charge the same<br />
for a pontic as an abutment. So I think most dentists<br />
would probably know that on a certain level. They<br />
couldn’t articulate it, but they would know on a certain<br />
level, that’s my favorite thing to do. And that’s<br />
probably why.<br />
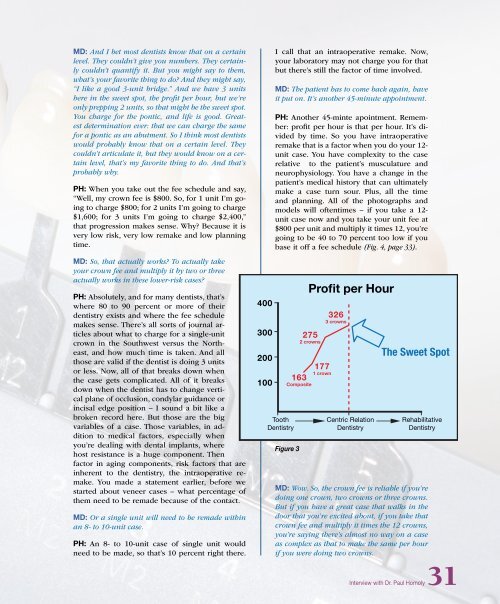
PH: When you take out the fee schedule and say,<br />
“Well, my crown fee is $800. So, for 1 unit I’m going<br />
to charge $800; for 2 units I’m going to charge<br />
$1,600; for 3 units I’m going to charge $2,400,”<br />
that progression makes sense. Why? Because it is<br />
very low risk, very low remake and low planning<br />
time.<br />
MD: So, that actually works? To actually take<br />
your crown fee and multiply it by two or three<br />
actually works in these lower-risk cases?<br />
PH: Absolutely, and for many dentists, that’s<br />
where 80 to 90 percent or more of their<br />
dentistry exists and where the fee schedule<br />
makes sense. There’s all sorts of journal articles<br />
about what to charge for a single-unit<br />
crown in the Southwest versus the Northeast,<br />
and how much time is taken. And all<br />
those are valid if the dentist is doing 3 units<br />
or less. Now, all of that breaks down when<br />
the case gets complicated. All of it breaks<br />
down when the dentist has to change vertical<br />
plane of occlusion, condylar guidance or<br />
incisal edge position – I sound a bit like a<br />
broken record here. But those are the big<br />
variables of a case. Those variables, in addition<br />
to medical factors, especially when<br />
you’re dealing with dental implants, where<br />
host resistance is a huge component. Then<br />
factor in aging components, risk factors that are<br />
inherent to the dentistry, the intraoperative remake.<br />
You made a statement earlier, before we<br />
started about veneer cases – what percentage of<br />
them need to be remade because of the contact.<br />
MD: Or a single unit will need to be remade within<br />
an 8- to 10-unit case.<br />
PH: An 8- to 10-unit case of single unit would<br />
need to be made, so that’s 10 percent right there.<br />
400<br />
300<br />
200<br />
100<br />
I call that an intraoperative remake. Now,<br />
your laboratory may not charge you for that<br />
but there’s still the factor of time involved.<br />
MD: The patient has to come back again, have<br />
it put on. It’s another 45-minute appointment.<br />
PH: Another 45-minte apointment. Remember:<br />
profit per hour is that per hour. It’s divided<br />
by time. So you have intraoperative<br />
remake that is a factor when you do your 12-<br />
unit case. You have complexity to the case<br />
relative to the patient’s musculature and<br />
neurophysiology. You have a change in the<br />
patient’s medical history that can ultimately<br />
make a case turn sour. Plus, all the time<br />
and planning. All of the photographs and<br />
models will oftentimes – if you take a 12-<br />
unit case now and you take your unit fee at<br />
$800 per unit and multiply it times 12, you’re<br />
going to be 40 to 70 percent too low if you<br />
base it off a fee schedule (Fig. 4, page 33).<br />
Tooth<br />
Dentistry<br />
Profit per Hour<br />
275<br />
2 crowns<br />
177<br />
1 crown<br />
163<br />
Composite<br />
Figure 3<br />
326<br />
3 crowns<br />
Centric Relation<br />
Dentistry<br />
The Sweet Spot<br />
Rehabilitative<br />
Dentistry<br />
MD: Wow. So, the crown fee is reliable if you’re<br />
doing one crown, two crowns or three crowns.<br />
But if you have a great case that walks in the<br />
door that you’re excited about, if you take that<br />
crown fee and multiply it times the 12 crowns,<br />
you’re saying there’s almost no way on a case<br />
as complex as that to make the same per hour<br />
if you were doing two crowns.<br />
Interview with Dr. Paul Homoly31














