

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
have to do that you didn’t foresee, that you didn’t plan on.<br />
Composites falling out and you’ve got to do some filler, and<br />
now that post is coming out.<br />
PH: Or you laid a flap and what looked like good bone<br />
now is mush and you have to graft the area and allow it<br />
to heal. Or you have a post-operative complication. You<br />
place three or four implants. I remember earlier in my<br />
career, we weren’t as sophisticated about our flap management.<br />
We’d place three to four implants. We’d come<br />
back in about 10 days or so, pull the lip back and you<br />
know what? Some of the cases, the flaps would open and<br />
we would see the tops of the implants, and that’s when I<br />
would feel the heat – the heat from my stomach come up,<br />
like swamp gas settling on my face.<br />
MD: That’s going to take a few minutes off of your life! And<br />
you weren’t being compensated for it, were you?<br />
PH: I wasn’t being compensated for it. So how do you fix<br />
a case like that? You don’t. You let it granulate in. You see<br />
the patient for 15-minute increments every two weeks and<br />
it’s like watching a death march. And the longer you look<br />
at the patient like a little thermometer, your profitability is<br />
going down. Now you’re just hoping to break even.<br />
And specialists wonder why more dentists don’t<br />
refer dental implants or complex-care patients. Because<br />
oftentimes the general dentist is much more<br />
profitable from the sweet spot on down, from 3<br />
units on down, than they are with these big godalmighty<br />
cases that sometimes can take years to<br />
complete. The dentist that refers a lot, Mike, is the<br />
dentist that has abundance in his or her practice.<br />
The dentist who’s doing a lot of bread and butter<br />
dentistry, their bills are paid, they’re making<br />
their profit goals, their staff is happy, they have<br />
a good facility, they feel good about the dentistry<br />
they’re doing. Abundance drives referrals. That’s a<br />
different topic we can touch on another time – the<br />
specialist-generalist relationship.<br />
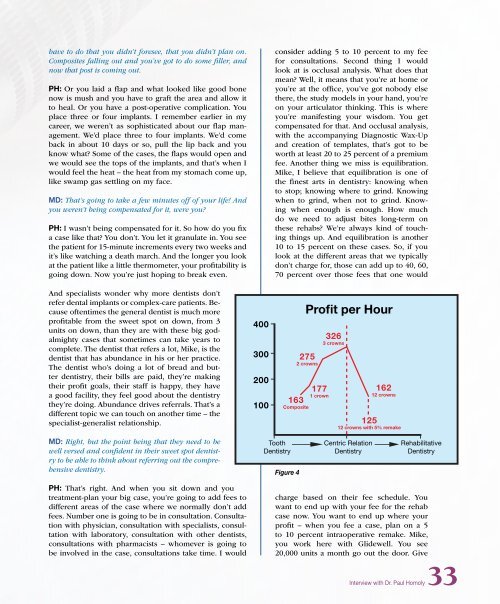
400<br />
300<br />
200<br />
100<br />
consider adding 5 to 10 percent to my fee<br />
for consultations. Second thing I would<br />
look at is occlusal analysis. What does that<br />
mean? Well, it means that you’re at home or<br />
you’re at the office, you’ve got nobody else<br />
there, the study models in your hand, you’re<br />
on your articulator thinking. This is where<br />
you’re manifesting your wisdom. You get<br />
compensated for that. And occlusal analysis,<br />
with the accompanying Diagnostic Wax-Up<br />
and creation of templates, that’s got to be<br />
worth at least 20 to 25 percent of a premium<br />
fee. Another thing we miss is equilibration.<br />
Mike, I believe that equilibration is one of<br />
the finest arts in dentistry: knowing when<br />
to stop; knowing where to grind. Knowing<br />
when to grind, when not to grind. Knowing<br />
when enough is enough. How much<br />
do we need to adjust bites long-term on<br />
these rehabs? We’re always kind of touching<br />
things up. And equilibration is another<br />
10 to 15 percent on these cases. So, if you<br />
look at the different areas that we typically<br />
don’t charge for, those can add up to 40, 60,<br />
70 percent over those fees that one would<br />
Profit per Hour<br />
275<br />
2 crowns<br />
177<br />
1 crown<br />
163<br />
Composite<br />
326<br />
3 crowns<br />
162<br />
12 crowns<br />
125<br />
12 crowns with 5% remake<br />
MD: Right, but the point being that they need to be<br />
well versed and confident in their sweet spot dentistry<br />
to be able to think about referring out the comprehensive<br />
dentistry.<br />
Tooth<br />
Dentistry<br />
Figure 4<br />
Centric Relation<br />
Dentistry<br />
Rehabilitative<br />
Dentistry<br />
PH: That’s right. And when you sit down and you<br />
treatment-plan your big case, you’re going to add fees to<br />
different areas of the case where we normally don’t add<br />
fees. Number one is going to be in consultation. Consultation<br />
with physician, consultation with specialists, consultation<br />
with laboratory, consultation with other dentists,<br />
consultations with pharmacists – whomever is going to<br />
be involved in the case, consultations take time. I would<br />
charge based on their fee schedule. You<br />
want to end up with your fee for the rehab<br />
case now. You want to end up where your<br />
profit – when you fee a case, plan on a 5<br />
to 10 percent intraoperative remake. Mike,<br />
you work here with <strong>Glidewell</strong>. You see<br />
20,000 units a month go out the door. Give<br />
Interview with Dr. Paul Homoly33














