

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
than glove-wearing nonreactors, which explained the greater number of HBV<br />
cases. 9<br />
Most reports on the effectiveness of gloves against viruses involve assumptions<br />
only. Hadler’s report, 34 which is unique because it was distributed by<br />
the CDC, is a typical example in which HBV was supposedly transmitted to<br />
patients by an oral and maxillofacial surgeon carrier. Prior to this discovery,<br />
the surgeon did not routinely wear gloves. No other HBV transmissions were<br />
noted after he began wearing gloves. The conclusion was that the gloves<br />
prevented further transmissions. Omitted from consideration was the later<br />
discovered shorter incubation period for HBV infection, the probability that<br />
the surgeon’s carrier status changed and that newly infected patients did not<br />
immediately test positive after the test surgeon began wearing gloves. This<br />
and three other similar studies were extrapolated by the CDC to apply to HIV<br />
infections and became the prime “scientific” rationale for the recommendation<br />
that gloves be worn as an element of Universal Precautions. 1 At that time, the<br />
AIDS epidemic was peaking and any rationale, scientific or not, would suffice<br />
for CDC action.<br />
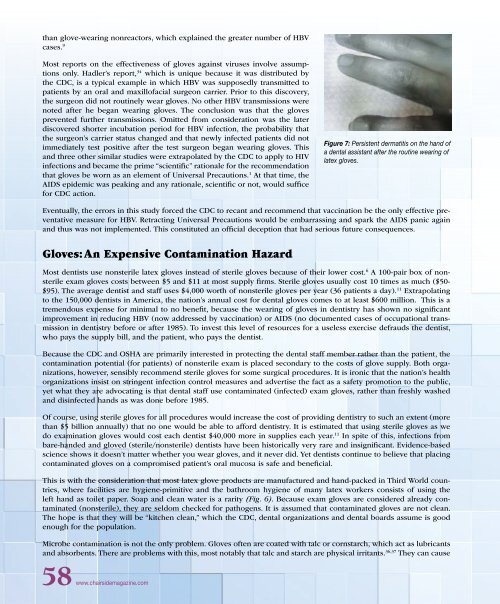
Figure 7: Persistent dermatitis on the hand of<br />
a dental assistant after the routine wearing of<br />
latex gloves.<br />
Eventually, the errors in this study forced the CDC to recant and recommend that vaccination be the only effective preventative<br />
measure for HBV. Retracting Universal Precautions would be embarrassing and spark the AIDS panic again<br />
and thus was not implemented. This constituted an official deception that had serious future consequences.<br />
Gloves: An Expensive Contamination Hazard<br />
Most dentists use nonsterile latex gloves instead of sterile gloves because of their lower cost. 6 A 100-pair box of nonsterile<br />
exam gloves costs between $5 and $11 at most supply firms. Sterile gloves usually cost 10 times as much ($50-<br />
$95). The average dentist and staff uses $4,000 worth of nonsterile gloves per year (36 patients a day). 11 Extrapolating<br />
to the 150,000 dentists in America, the nation’s annual cost for dental gloves comes to at least $600 million. This is a<br />
tremendous expense for minimal to no benefit, because the wearing of gloves in dentistry has shown no significant<br />
improvement in reducing HBV (now addressed by vaccination) or AIDS (no documented cases of occupational transmission<br />
in dentistry before or after 1985). To invest this level of resources for a useless exercise defrauds the dentist,<br />
who pays the supply bill, and the patient, who pays the dentist.<br />
Because the CDC and OSHA are primarily interested in protecting the dental staff member rather than the patient, the<br />
contamination potential (for patients) of nonsterile exam is placed secondary to the costs of glove supply. Both organizations,<br />
however, sensibly recommend sterile gloves for some surgical procedures. It is ironic that the nation’s health<br />
organizations insist on stringent infection control measures and advertise the fact as a safety promotion to the public,<br />
yet what they are advocating is that dental staff use contaminated (infected) exam gloves, rather than freshly washed<br />
and disinfected hands as was done before 1985.<br />
Of course, using sterile gloves for all procedures would increase the cost of providing dentistry to such an extent (more<br />
than $5 billion annually) that no one would be able to afford dentistry. It is estimated that using sterile gloves as we<br />
do examination gloves would cost each dentist $40,000 more in supplies each year. 11 In spite of this, infections from<br />
bare-handed and gloved (sterile/nonsterile) dentists have been historically very rare and insignificant. Evidence-based<br />
science shows it doesn’t matter whether you wear gloves, and it never did. Yet dentists continue to believe that placing<br />
contaminated gloves on a compromised patient’s oral mucosa is safe and beneficial.<br />
This is with the consideration that most latex glove products are manufactured and hand-packed in Third World countries,<br />
where facilities are hygiene-primitive and the bathroom hygiene of many latex workers consists of using the<br />
left hand as toilet paper. Soap and clean water is a rarity (Fig. 6). Because exam gloves are considered already contaminated<br />
(nonsterile), they are seldom checked for pathogens. It is assumed that contaminated gloves are not clean.<br />
The hope is that they will be “kitchen clean,” which the CDC, dental organizations and dental boards assume is good<br />
enough for the population.<br />
Microbe contamination is not the only problem. Gloves often are coated with talc or cornstarch, which act as lubricants<br />
and absorbents. There are problems with this, most notably that talc and starch are physical irritants. 36,37 They can cause<br />
58 www.chairsidemagazine.com














