

PDF Download - Glidewell Dental Labs
PDF Download - Glidewell Dental Labs
PDF Download - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
BB: Sounds like it’s a truly interdisciplinary<br />
practice.<br />
DL: Absolutely. We’re really blessed to<br />
be able to jump in and take care of<br />
things, especially trauma cases.<br />
BB: You mentioned medical considerations<br />
as a determining factor when deciding<br />
what you might refer out. What<br />
are red flags for you when you’re looking<br />
at a patient’s medical history?<br />
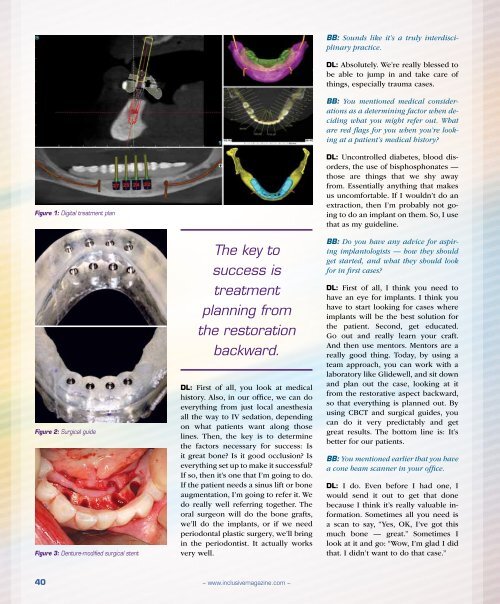
Figure 1: Digital treatment plan<br />
Figure 2: Surgical guide<br />
Figure 3: Denture-modified surgical stent<br />
The key to<br />
success is<br />
treatment<br />
planning from<br />
the restoration<br />
backward.<br />
DL: First of all, you look at medical<br />
history. Also, in our office, we can do<br />
everything from just local anesthesia<br />
all the way to IV sedation, depending<br />
on what patients want along those<br />
lines. Then, the key is to determine<br />
the factors necessary for success: Is<br />
it great bone? Is it good occlusion? Is<br />
everything set up to make it successful?<br />
If so, then it’s one that I’m going to do.<br />
If the patient needs a sinus lift or bone<br />
augmentation, I’m going to refer it. We<br />
do really well referring together. The<br />
oral surgeon will do the bone grafts,<br />
we’ll do the implants, or if we need<br />
periodontal plastic surgery, we’ll bring<br />
in the periodontist. It actually works<br />
very well.<br />
DL: Uncontrolled diabetes, blood disorders,<br />
the use of bisphosphonates —<br />
those are things that we shy away<br />
from. Essentially anything that makes<br />
us uncomfortable. If I wouldn’t do an<br />
extraction, then I’m probably not going<br />
to do an implant on them. So, I use<br />
that as my guideline.<br />
BB: Do you have any advice for aspiring<br />
implantologists — how they should<br />
get started, and what they should look<br />
for in first cases?<br />
DL: First of all, I think you need to<br />
have an eye for implants. I think you<br />
have to start looking for cases where<br />
implants will be the best solution for<br />
the patient. Second, get educated.<br />
Go out and really learn your craft.<br />
And then use mentors. Mentors are a<br />
really good thing. Today, by using a<br />
team approach, you can work with a<br />
laboratory like <strong>Glidewell</strong>, and sit down<br />
and plan out the case, looking at it<br />
from the restorative aspect backward,<br />
so that everything is planned out. By<br />
using CBCT and surgical guides, you<br />
can do it very predictably and get<br />
great results. The bottom line is: It’s<br />
better for our patients.<br />
BB: You mentioned earlier that you have<br />
a cone beam scanner in your office.<br />
DL: I do. Even before I had one, I<br />
would send it out to get that done<br />
because I think it’s really valuable information.<br />
Sometimes all you need is<br />
a scan to say, “Yes, OK, I’ve got this<br />
much bone — great.” Sometimes I<br />
look at it and go: “Wow, I’m glad I did<br />
that. I didn’t want to do that case.”<br />
40<br />
– www.inclusivemagazine.com –














