

PDF Download - Glidewell Dental Labs
PDF Download - Glidewell Dental Labs
PDF Download - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
But the real key is not just the CBCT.<br />
It’s putting it in the software and being<br />
able to manipulate it. I call it virtual<br />
planning. I want to be able to show<br />
my patient that I’m going to put in<br />
this size implant, and this is why, and<br />
this is how it’s going to be contoured<br />
and shaped, all the way to the final<br />
restoration. Because I think the key to<br />
success is treatment planning from the<br />
restoration backward.<br />
BB: What is your favorite planning software?<br />
There are several on the market.<br />
DL: I use SimPlant ® (Materialise <strong>Dental</strong><br />
Inc.; Glen Burnie, Md.), mostly<br />
because you can use every implant<br />
system. But with whatever implant<br />
you’re using, there is going to be a<br />
system that will work with you. So,<br />
again, I think you’ve got to look at the<br />
total picture.<br />
BB: We’ve had the same experience. We<br />
do a lot of SimPlant cases here because it<br />
has an open architecture. Let’s talk about<br />
guided surgery and level of guidance.<br />
DL: Obviously, you can have the lab<br />
make a guide for you from a wax-up.<br />
That will kind of give you the position,<br />
but it doesn’t really give you the angle,<br />
doesn’t give you the depth. It just gives<br />
you a guide to stay within that area.<br />
Or you can go all the way to where<br />
you can actually control depth, angle,<br />
and position; you can even place the<br />
implant through the guide (Figs. 1, 2).<br />
Everything is planned out. I like that<br />
the best because it gives me the perfect<br />
emergence profile. The software helps<br />
me establish what my abutment is<br />
going to be like, so the laboratory can<br />
work with me to create a provisional<br />
that stays in that same position —<br />
everything is worked through.<br />
I’ll also say that using even the<br />
patient’s denture as a guide is huge<br />
because that makes sure that you keep<br />
those implants in the neutral zone,<br />
and you’re going to get a great result<br />
as well (Fig. 3). There are a lot of guide<br />
techniques, but I like using the one<br />
that controls all of it, if I can.<br />
BB: At the California <strong>Dental</strong> Association<br />
(CDA) meeting in Anaheim last<br />
May, you spoke on the topic of overdentures.<br />
Can you talk a little bit about how<br />
you approach your edentulous patients?<br />
DL: A lot of denture patients are dental<br />
cripples. They really can’t function<br />
and they can’t eat. So, one of the<br />
things I do is I ask them, “Do you want<br />
to eat what you want, or eat only what<br />
you can?” Then I talk about what the<br />
different solutions are. I ask questions<br />
like, “At the end of this, would you just<br />
like it that your denture stays in a little<br />
better, or are you looking for something<br />
that you never have to take out?”<br />
Their answers will tell you the direction<br />
they want to go. Then I look at<br />
implant-retained, soft tissue-supported<br />
as a solution. You can do that with<br />
mini implants, or you can do that with<br />
two or four conventional implants,<br />
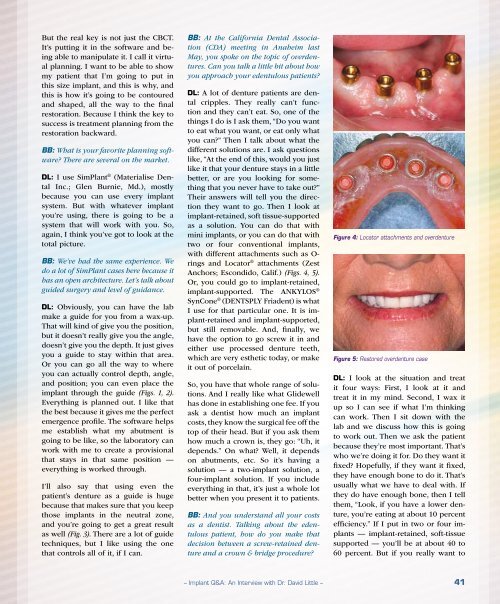
with different attachments such as O-<br />
rings and Locator ® attachments (Zest<br />
Anchors; Escondido, Calif.) (Figs. 4, 5).<br />
Or, you could go to implant-retained,<br />
implant-supported. The ANKYLOS ®<br />
SynCone ® (DENTSPLY Friadent) is what<br />
I use for that particular one. It is implant-retained<br />
and implant-supported,<br />
but still removable. And, finally, we<br />
have the option to go screw it in and<br />
either use processed denture teeth,<br />
which are very esthetic today, or make<br />
it out of porcelain.<br />
So, you have that whole range of solutions.<br />
And I really like what <strong>Glidewell</strong><br />
has done in establishing one fee. If you<br />
ask a dentist how much an implant<br />
costs, they know the surgical fee off the<br />
top of their head. But if you ask them<br />
how much a crown is, they go: “Uh, it<br />
depends.” On what? Well, it depends<br />
on abutments, etc. So it’s having a<br />
solution — a two-implant solution, a<br />
four-implant solution. If you include<br />
everything in that, it’s just a whole lot<br />
better when you present it to patients.<br />
BB: And you understand all your costs<br />
as a dentist. Talking about the edentulous<br />
patient, how do you make that<br />
decision between a screw-retained denture<br />
and a crown & bridge procedure?<br />
Figure 4: Locator attachments and overdenture<br />
Figure 5: Restored overdenture case<br />
DL: I look at the situation and treat<br />
it four ways: First, I look at it and<br />
treat it in my mind. Second, I wax it<br />
up so I can see if what I’m thinking<br />
can work. Then I sit down with the<br />
lab and we discuss how this is going<br />
to work out. Then we ask the patient<br />
because they’re most important. That’s<br />
who we’re doing it for. Do they want it<br />
fixed? Hopefully, if they want it fixed,<br />
they have enough bone to do it. That’s<br />
usually what we have to deal with. If<br />
they do have enough bone, then I tell<br />
them, “Look, if you have a lower denture,<br />
you’re eating at about 10 percent<br />
efficiency.” If I put in two or four implants<br />
— implant-retained, soft-tissue<br />
supported — you’ll be at about 40 to<br />
60 percent. But if you really want to<br />
– Implant Q&A: An Interview with Dr. David Little – 41














