Veras FHAP, et al. <strong>Anomalous</strong> <strong>Origin</strong> <strong>of</strong> <strong>Coronary</strong> <strong>Arteries</strong>. Rev Bras Cardiol Invas 2007; 15(3).with an anomalous origin in the aorta, congenital atresia<strong>of</strong> the left coronary trunk, coronary arteriovenous fistulas,coronary arteries forming myocardial bridges, aneurysms<strong>of</strong> coronary arteries and coronary stenosis.For Angelini et al. 8 , a coronary anomaly should bedefined as any coronary pattern, with a characteristic(number <strong>of</strong> ostios, proximal course, distal bed… ) “rarely”encountered in the general population. The followingdefinitions being favorable: normal, any morphologicalcharacteristic observed in more than 1% <strong>of</strong> a nonselectedpopulation; variable <strong>of</strong> normality, a relativelyuncommon morphological characteristic prevalent inmore than 1% <strong>of</strong> the population; and anomaly, a morphologicalcharacteristic seen in less than 1% <strong>of</strong> thatpopulation. Normal coronary anatomy, universally accepted,is defined in this way 16,17 :• The coronary trunk originates from the left coronarysinus and divides into descendent anterior arteryand circumflex artery;• The anterior descendent artery follows behindthe pulmonary trunk in the intraventricular anteriorgrove;• The circumflex artery follows the posterioratrioventricular grove;• The right coronary artery originates from the rightcoronary sinus and follows along the anterioratrioventricular grove.Any alteration in this pattern must be consideredas an anomalous coronary anatomy 16,17 . The circumflexcoronary artery, originating from the right coronarysinus or from the right coronary artery, with a retroaorticcourse, is the most common congenital anomaly<strong>of</strong> the coronary artery 18, 19 .PHYSIOPATHOLOGY<strong>Coronary</strong> anomalies have been implicated as a causefor thoracic pain, sudden death, heart insufficiency,syncope, dyspnea, ventricular fibrillation and AMI 8 .In the OACEP, it is observed that, during intrauterinelife, no functional alteration takes place, however,after birth, in the measure that arteriolar resistance fallsand blood pressure decreases in the pulmonary artery,the oxi-hemoglobinic saturation <strong>of</strong> the venous blooddiminishes, the arterial channel and the oval foramenclose, progressively diminishing the myocardial bloodperfusion, irrigated by the anomalous artery, leadingto ischemic alterations.The OACEP is generally an isolated defect, butmight be associated, in about 5% <strong>of</strong> cases, to othercardiac defects such as, intraventricular communication,interatrial communication, aortal coarctation, Fallot’sTetralogy and other anomalies 13 . In Fallot’s Tetralogybearers, the incidence <strong>of</strong> coronary anomaly can varyfrom 3% to 36% 20,21 .The congenital atresy <strong>of</strong> the left coronary trunk(LCT) is an extremely rare anomaly and generally hasa benign evolution 22 . In some cases, it can lead tomyocardium ischemia and sudden death 22 . The bearers<strong>of</strong> this anomaly survive thanks to the development <strong>of</strong>collateral circulation for the anterior descendent artery 22 .Collateral circulation can be made up by branches/bunches from the cone artery, also known as VieussensCircle; or anastomosis between the anterior ventricularbranches <strong>of</strong> the right coronary artery and the anteriordescendent artery 22,23 .The explanation for myocardial ischemia in theatresia <strong>of</strong> the TCE, in the absence <strong>of</strong> arterioscleroses orvessel spasm, is not clear and the most logical justificationis the fact that an only coronary artery is incapable <strong>of</strong>supplying, adequately, the myocardial blood demand 22 .The anomalous origin <strong>of</strong> the left coronary artery<strong>of</strong> the right coronary sinus can be related to suddendeath in 59% <strong>of</strong> cases, preceded by physical activityin 81% <strong>of</strong> events 8 . This anomaly can present 4 courses:anterior, to the pulmonary artery; posterior, to the aorta;intra-septal, between the aorta and the pulmonary artery;and intra-arterial, between the aorta and the pulmonary(Figure 1) 24 . All the subtypes <strong>of</strong> this anomaly have beenassociated to sudden death, but the intra-arterial variety,which is the most common pattern, has a strongerrelation with catastrophic events 1,8,24-26 .Potential mechanisms have been erected to explainthe presence <strong>of</strong> myocardial ischemia and sudden deathin patients with OACEA; the formation <strong>of</strong> an acute andcontorted angle at the origin <strong>of</strong> the anomalous coronary<strong>of</strong> the aorta; a narrowing <strong>of</strong> the coronary orifice, secondaryto the anomalous anatomy; compression <strong>of</strong>the anomalous coronary artery during its course betweenthe aorta and the pulmonary trunk during exercise; andspasm <strong>of</strong> the anomalous artery, possibly as a result <strong>of</strong>endothelial injury 8,27,28 .According with current evidence, the coronarysegments with anomalous course are not more susceptibleto obstructive arterosclerotic disease than normalsegments in a same individual 8,9 (Figure 1).CLINICAL OUTLOOKThe OACEP presents two levels: an infantile formand an adult form. The infantile form is characterizedby poor intercoronary collateral circulation, which canresult in AMI, cardiac insufficiency or sudden death 11 .In this type <strong>of</strong> presentation, the symptoms appear in thefirst months <strong>of</strong> life, with constant crying, intense paleness,sudden stop when suckling, weight loss and signs <strong>of</strong>cardiac insufficiency, such as taquipnea tachycardia,tiredness while suckling, sweating, hepathomegalia andperipherical cyanosis. On auscultation, a galloping rhythmcan be heard, muffling <strong>of</strong> the bustle, especially thefirst one, and occasionally, the appearance <strong>of</strong> systolic2
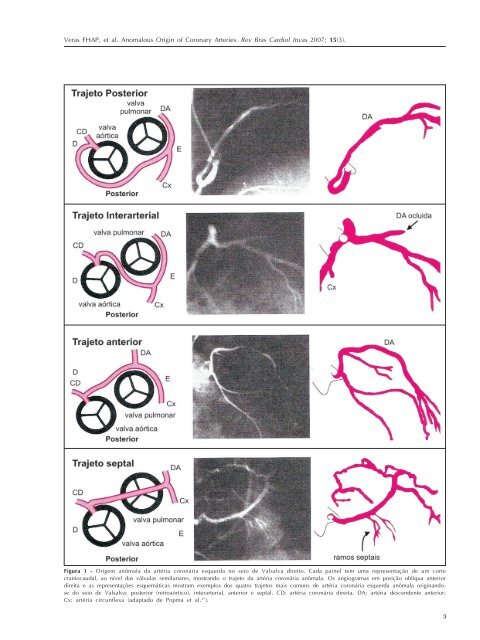
Veras FHAP, et al. <strong>Anomalous</strong> <strong>Origin</strong> <strong>of</strong> <strong>Coronary</strong> <strong>Arteries</strong>. Rev Bras Cardiol Invas 2007; 15(3).Figura 1 - Origem anômala da artéria coronária esquerda no seio de Valsalva direito. Cada painel tem uma representação de um cortecraniocaudal, ao nível das válvulas semilunares, mostrando o trajeto da artéria coronária anômala. Os angiogramas em posição oblíqua anteriordireita e as representações esquemáticas mostram exemplos dos quatro trajetos mais comuns de artéria coronária esquerda anômala originandosedo seio de Valsalva: posterior (retroaórtico), interarterial, anterior e septal. CD: artéria coronária direita, DA: artéria descendente anterior;Cx: artéria circunflexa (adaptado de Popma et al. 27 ).3