Veras FHAP, et al. <strong>Anomalous</strong> <strong>Origin</strong> <strong>of</strong> <strong>Coronary</strong> <strong>Arteries</strong>. Rev Bras Cardiol Invas 2007; 15(3).murmur in the mitral area, as a result <strong>of</strong> secondarymitral insufficiency to the increase <strong>of</strong> the cardiac areadue to its dilatation or due to dysfunction <strong>of</strong> the papillarymuscle 10,11 . Mortality during the first year <strong>of</strong> life isestimated at 90%, even with clinical treatment 10,11 .The adult or mature form can occur in childrenand necessarily in adults in around 10 – 15% <strong>of</strong> cases.It is characterized by an abundance <strong>of</strong> intercoronarycollateral circulation, <strong>of</strong> sufficient magnitude to allowa survival rate until adult age, in some cases, it hasbeen told, until 72 years <strong>of</strong> age.Sometimes, there are no appreciable clinical manifestationsand the diagnosis <strong>of</strong> OACEP is suspecteddue to the presence <strong>of</strong> murmurs: continuous, as aresult <strong>of</strong> the passage <strong>of</strong> blood through the coronarypulmonaryfistula, or systolic, because <strong>of</strong> dysfunction<strong>of</strong> the mitral valve 10 . Some patients evolve towardscardiac insufficiency; others towards angina 10,11 .In the OACEA, some symptoms such as syncope,chest pain and palpitations may be present 12,28 . Butmost bearers are asymptomatic and the only expression<strong>of</strong> this coronary anomaly in young athletes might besudden death 12,28 . The studies suggest that these coronaryanomalies can be lethal only during or immediatelyafter extenuating physical exercise, typically in youngsubjects 8 . (Table 1).COMPLEMENTARY EXAMSElectrocardiogram (ECG) and ergometric test (ET)One study demonstrated that the presence <strong>of</strong> the“Q” wave with a depth over 3 mm, duration higherthan 30 ms and a “QR” pattern in at least one <strong>of</strong> thedeviations – DI, aVL, V5-V7, was present in 100% <strong>of</strong>exams <strong>of</strong> patients with OACEP 29 . The absence <strong>of</strong> the“Q” wave in the lower wall is also a prevalent finding(82% <strong>of</strong> cases) 13,15,29 . The axel deviation towards theleft is less frequent (64% <strong>of</strong> cases) 13 . Atypical electrocardiographicalterations can mask the illness whenassociated to lesions with important pulmonary hip<strong>of</strong>lux.In the OACEA, the ECG and the TE are almostalways normal 8,9,12,28 . In spite <strong>of</strong> the OACEA being thecause <strong>of</strong> myocardial ischemia, this is incidental, with manifestationsunder extenuating clinical conditions 8,9,12,28 .Thorax X-RayIn general, it shows alterations in the cases associatedto cardiac insufficiency. In the OACEP, young agedchildren can present an increase <strong>of</strong> the cardiac area 10 .Lung circulation is normal, however, when cardiacinsufficiency is present, a picture <strong>of</strong> venous pulmonarycongestion can be observed 10 .EchocardiogramThe bidimensional echocardiogram with coloredDoppler is useful in the morph<strong>of</strong>unctional assessment<strong>of</strong> the heart. For the diagnosis <strong>of</strong> anomalous origin <strong>of</strong>the coronary arteries, the studies show a variablesensibility, with better results in children 11,13,15,26 .The transesophageal echocardiogram (TEE) is anexam with a much higher sensibility for the detection<strong>of</strong> the anomalous origin <strong>of</strong> coronary arteries 1,26 . TheTEE, specially with the use <strong>of</strong> a multi-plane probe/catheter, is capable <strong>of</strong> drawing, with precision, theproximal course and the flux pattern in the anomalouscoronary arteries 1,26 .Computer Tomography <strong>of</strong> <strong>Coronary</strong> <strong>Arteries</strong> (CTCA)The studies show a quick evolution <strong>of</strong> this noninvasivemethod in the assessment <strong>of</strong> coronary arteries.Initially, the studies with the Electron Beam ComputedTomography (EBCT), demonstrated excellent accuracyin the assessment <strong>of</strong> the origin and proximal course <strong>of</strong>coronary anomalies 19,25 .With the advent <strong>of</strong> Computer Tomography withMultiple Detectors (16 and 64 acquisitions), a betterassessment <strong>of</strong> the middle and distal segments waspossible, for the detection <strong>of</strong> obstructive coronary arteryillness 16. It uses ionizing radiation and requires theuse <strong>of</strong> medication to diminish heart frequency 25. Themethod requires the administration <strong>of</strong> a contrast meansin the veins, which is potentially allergic and nephrotoxic.The data in the literature show it to be a safe andefficient method with excellent spatial resolution 16,24,25,30 .Comparative studies with coronary angiography haveshown a higher efficacy, suggesting that ComputerTomography with Multiple Detectors is the ideal examfor the detection <strong>of</strong> coronary anomalies 16,19 .TABELA 1Incidência de morte súbita relacionada a anomalias de artérias coronárias (adaptado de Angelini et al. 8 ).Grupo (idade) Número de mortes Mortes relacionadas a anomalias coronarianas,%Indivíduos fazendo exercício (8-66 a) 550 11População geral (< 40 a) 162 0,6Atletas competitivos(idade média de 17 a) 134 23Corredores (30-46 a) 120 1,6Indivíduos fazendo exercício, Maryland - EUA 62 04
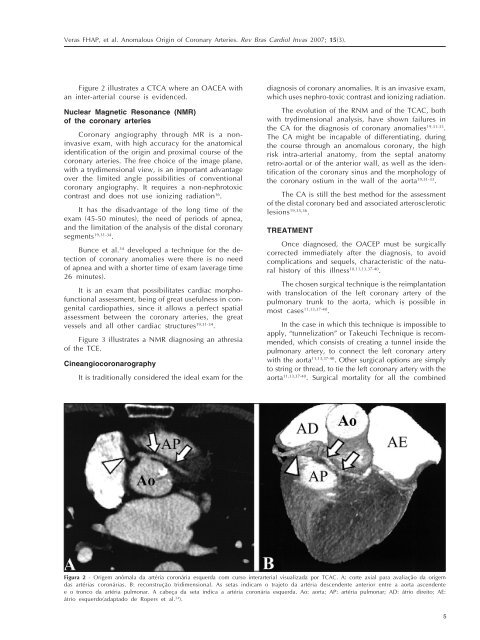
Veras FHAP, et al. <strong>Anomalous</strong> <strong>Origin</strong> <strong>of</strong> <strong>Coronary</strong> <strong>Arteries</strong>. Rev Bras Cardiol Invas 2007; 15(3).Figure 2 illustrates a CTCA where an OACEA withan inter-arterial course is evidenced.Nuclear Magnetic Resonance (NMR)<strong>of</strong> the coronary arteries<strong>Coronary</strong> angiography through MR is a noninvasiveexam, with high accuracy for the anatomicalidentification <strong>of</strong> the origin and proximal course <strong>of</strong> thecoronary arteries. The free choice <strong>of</strong> the image plane,with a trydimensional view, is an important advantageover the limited angle possibilities <strong>of</strong> conventionalcoronary angiography. It requires a non-nephrotoxiccontrast and does not use ionizing radiation 16 .It has the disadvantage <strong>of</strong> the long time <strong>of</strong> theexam (45-50 minutes), the need <strong>of</strong> periods <strong>of</strong> apnea,and the limitation <strong>of</strong> the analysis <strong>of</strong> the distal coronarysegments 19,31-34 .Bunce et al. 34 developed a technique for the detection<strong>of</strong> coronary anomalies were there is no need<strong>of</strong> apnea and with a shorter time <strong>of</strong> exam (average time26 minutes).It is an exam that possibilitates cardiac morph<strong>of</strong>unctionalassessment, being <strong>of</strong> great usefulness in congenitalcardiopathies, since it allows a perfect spatialassessment between the coronary arteries, the greatvessels and all other cardiac structures 19,31-34 .Figure 3 illustrates a NMR diagnosing an athresia<strong>of</strong> the TCE.CineangiocoronarographyIt is traditionally considered the ideal exam for thediagnosis <strong>of</strong> coronary anomalies. It is an invasive exam,which uses nephro-toxic contrast and ionizing radiation.The evolution <strong>of</strong> the RNM and <strong>of</strong> the TCAC, bothwith trydimensional analysis, have shown failures inthe CA for the diagnosis <strong>of</strong> coronary anomalies 19,31-33 .The CA might be incapable <strong>of</strong> differentiating, duringthe course through an anomalous coronary, the highrisk intra-arterial anatomy, from the septal anatomyretro-aortal or <strong>of</strong> the anterior wall, as well as the identification<strong>of</strong> the coronary sinus and the morphology <strong>of</strong>the coronary ostium in the wall <strong>of</strong> the aorta 19,31-33 .The CA is still the best method for the assessment<strong>of</strong> the distal coronary bed and associated arteroscleroticlesions 19,35,36 .TREATMENTOnce diagnosed, the OACEP must be surgicallycorrected immediately after the diagnosis, to avoidcomplications and sequels, characteristic <strong>of</strong> the naturalhistory <strong>of</strong> this illness 10,11,13,37-40 .The chosen surgical technique is the reimplantationwith translocation <strong>of</strong> the left coronary artery <strong>of</strong> thepulmonary trunk to the aorta, which is possible inmost cases 11,13,37-40 .In the case in which this technique is impossible toapply, “tunnelization” or Takeuchi Technique is recommended,which consists <strong>of</strong> creating a tunnel inside thepulmonary artery, to connect the left coronary arterywith the aorta 11,13,37-40 . Other surgical options are simplyto string or thread, to tie the left coronary artery with theaorta 11,13,37-40 . Surgical mortality for all the combinedFigura 2 - Origem anômala da artéria coronária esquerda com curso interarterial visualizada por TCAC. A: corte axial para avaliação da origemdas artérias coronárias. B: reconstrução tridimensional. As setas indicam o trajeto da artéria descendente anterior entre a aorta ascendentee o tronco da artéria pulmonar. A cabeça da seta indica a artéria coronária esquerda. Ao: aorta; AP: artéria pulmonar; AD: átrio direito; AE:átrio esquerdo(adaptado de Ropers et al. 24 ).5