

Download Update 11 - Update in Anaesthesia - WFSA
Download Update 11 - Update in Anaesthesia - WFSA
Download Update 11 - Update in Anaesthesia - WFSA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
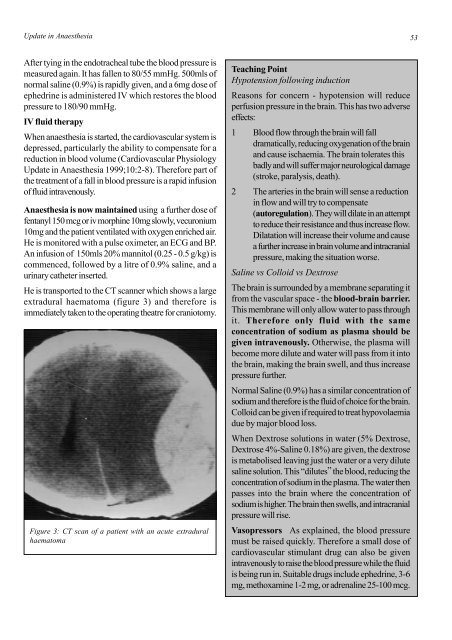
<strong>Update</strong> <strong>in</strong> <strong>Anaesthesia</strong> 53After ty<strong>in</strong>g <strong>in</strong> the endotracheal tube the blood pressure ismeasured aga<strong>in</strong>. It has fallen to 80/55 mmHg. 500mls ofnormal sal<strong>in</strong>e (0.9%) is rapidly given, and a 6mg dose ofephedr<strong>in</strong>e is adm<strong>in</strong>istered IV which restores the bloodpressure to 180/90 mmHg.IV fluid therapyWhen anaesthesia is started, the cardiovascular system isdepressed, particularly the ability to compensate for areduction <strong>in</strong> blood volume (Cardiovascular Physiology<strong>Update</strong> <strong>in</strong> <strong>Anaesthesia</strong> 1999;10:2-8). Therefore part ofthe treatment of a fall <strong>in</strong> blood pressure is a rapid <strong>in</strong>fusionof fluid <strong>in</strong>travenously.<strong>Anaesthesia</strong> is now ma<strong>in</strong>ta<strong>in</strong>ed us<strong>in</strong>g a further dose offentanyl 150 mcg or iv morph<strong>in</strong>e 10mg slowly, vecuronium10mg and the patient ventilated with oxygen enriched air.He is monitored with a pulse oximeter, an ECG and BP.An <strong>in</strong>fusion of 150mls 20% mannitol (0.25 - 0.5 g/kg) iscommenced, followed by a litre of 0.9% sal<strong>in</strong>e, and aur<strong>in</strong>ary catheter <strong>in</strong>serted.He is transported to the CT scanner which shows a largeextradural haematoma (figure 3) and therefore isimmediately taken to the operat<strong>in</strong>g theatre for craniotomy.Figure 3: CT scan of a patient with an acute extraduralhaematomaTeach<strong>in</strong>g Po<strong>in</strong>tHypotension follow<strong>in</strong>g <strong>in</strong>ductionReasons for concern - hypotension will reduceperfusion pressure <strong>in</strong> the bra<strong>in</strong>. This has two adverseeffects:1 Blood flow through the bra<strong>in</strong> will falldramatically, reduc<strong>in</strong>g oxygenation of the bra<strong>in</strong>and cause ischaemia. The bra<strong>in</strong> tolerates thisbadly and will suffer major neurological damage(stroke, paralysis, death).2 The arteries <strong>in</strong> the bra<strong>in</strong> will sense a reduction<strong>in</strong> flow and will try to compensate(autoregulation). They will dilate <strong>in</strong> an attemptto reduce their resistance and thus <strong>in</strong>crease flow.Dilatation will <strong>in</strong>crease their volume and causea further <strong>in</strong>crease <strong>in</strong> bra<strong>in</strong> volume and <strong>in</strong>tracranialpressure, mak<strong>in</strong>g the situation worse.Sal<strong>in</strong>e vs Colloid vs DextroseThe bra<strong>in</strong> is surrounded by a membrane separat<strong>in</strong>g itfrom the vascular space - the blood-bra<strong>in</strong> barrier.This membrane will only allow water to pass throughit. Therefore only fluid with the sameconcentration of sodium as plasma should begiven <strong>in</strong>travenously. Otherwise, the plasma willbecome more dilute and water will pass from it <strong>in</strong>tothe bra<strong>in</strong>, mak<strong>in</strong>g the bra<strong>in</strong> swell, and thus <strong>in</strong>creasepressure further.Normal Sal<strong>in</strong>e (0.9%) has a similar concentration ofsodium and therefore is the fluid of choice for the bra<strong>in</strong>.Colloid can be given if required to treat hypovolaemiadue by major blood loss.When Dextrose solutions <strong>in</strong> water (5% Dextrose,Dextrose 4%-Sal<strong>in</strong>e 0.18%) are given, the dextroseis metabolised leav<strong>in</strong>g just the water or a very dilutesal<strong>in</strong>e solution. This “dilutes” the blood, reduc<strong>in</strong>g theconcentration of sodium <strong>in</strong> the plasma. The water thenpasses <strong>in</strong>to the bra<strong>in</strong> where the concentration ofsodium is higher. The bra<strong>in</strong> then swells, and <strong>in</strong>tracranialpressure will rise.Vasopressors As expla<strong>in</strong>ed, the blood pressuremust be raised quickly. Therefore a small dose ofcardiovascular stimulant drug can also be given<strong>in</strong>travenously to raise the blood pressure while the fluidis be<strong>in</strong>g run <strong>in</strong>. Suitable drugs <strong>in</strong>clude ephedr<strong>in</strong>e, 3-6mg, methoxam<strong>in</strong>e 1-2 mg, or adrenal<strong>in</strong>e 25-100 mcg.













