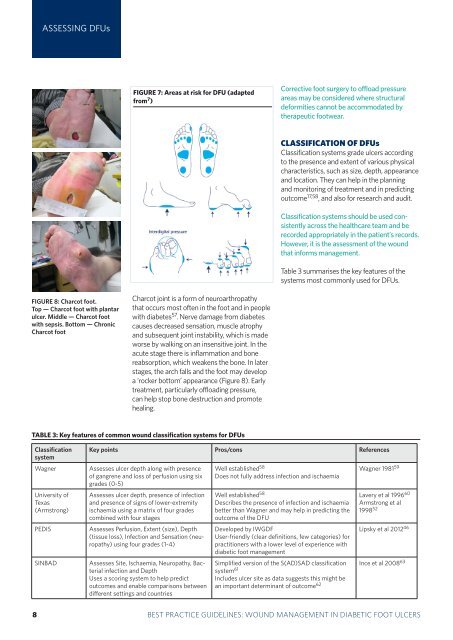
ASSESSING DFUsFIGURE 7: Areas at risk for DFU (adaptedfrom 7 )Corrective <strong>foot</strong> surgery to offload pressureareas may be considered where structuraldeformities cannot be accommodated bytherapeutic <strong>foot</strong>wear.CLASSIFICATION OF DFUsClassification systems grade <strong>ulcers</strong> accord<strong>in</strong>gto the presence and extent of various physicalcharacteristics, such as size, depth, appearanceand location. They can help <strong>in</strong> the plann<strong>in</strong>gand monitor<strong>in</strong>g of treatment and <strong>in</strong> predict<strong>in</strong>goutcome 17,58 , and also for research and audit.Classification systems should be used consistentlyacross the healthcare team and berecorded appropriately <strong>in</strong> the patient’s records.However, it is the assessment of the <strong>wound</strong>that <strong>in</strong>forms <strong>management</strong>.Table 3 summarises the key features of thesystems most commonly used for DFUs.FIGURE 8: Charcot <strong>foot</strong>.Top — Charcot <strong>foot</strong> with plantarulcer. Middle — Charcot <strong>foot</strong>with sepsis. Bottom — ChronicCharcot <strong>foot</strong>Charcot jo<strong>in</strong>t is a form of neuroarthropathythat occurs most often <strong>in</strong> the <strong>foot</strong> and <strong>in</strong> peoplewith diabetes 57 . Nerve damage from diabetescauses decreased sensation, muscle atrophyand subsequent jo<strong>in</strong>t <strong>in</strong>stability, which is madeworse by walk<strong>in</strong>g on an <strong>in</strong>sensitive jo<strong>in</strong>t. In theacute stage there is <strong>in</strong>flammation and bonereabsorption, which weakens the bone. In laterstages, the arch falls and the <strong>foot</strong> may developa ‘rocker bottom’ appearance (Figure 8). Earlytreatment, particularly offload<strong>in</strong>g pressure,can help stop bone destruction and promoteheal<strong>in</strong>g.TABLE 3: Key features of common <strong>wound</strong> classification systems for DFUsClassificationsystemWagnerUniversity ofTexas(Armstrong)PEDISSINBADKey po<strong>in</strong>ts Pros/cons ReferencesAssesses ulcer depth along with presenceof gangrene and loss of perfusion us<strong>in</strong>g sixgrades (0-5)Assesses ulcer depth, presence of <strong>in</strong>fectionand presence of signs of lower-extremityischaemia us<strong>in</strong>g a matrix of four gradescomb<strong>in</strong>ed with four stagesAssesses Perfusion, Extent (size), Depth(tissue loss), Infection and Sensation (neuropathy)us<strong>in</strong>g four grades (1-4)Assesses Site, Ischaemia, Neuropathy, Bacterial<strong>in</strong>fection and DepthUses a scor<strong>in</strong>g system to help predictoutcomes and enable comparisons betweendifferent sett<strong>in</strong>gs and countriesWell established 58Does not fully address <strong>in</strong>fection and ischaemiaWell established 58Describes the presence of <strong>in</strong>fection and ischaemiabetter than Wagner and may help <strong>in</strong> predict<strong>in</strong>g theoutcome of the DFUDeveloped by IWGDFUser-friendly (clear def<strong>in</strong>itions, few categories) forpractitioners with a lower level of experience with<strong>diabetic</strong> <strong>foot</strong> <strong>management</strong>Wagner 1981 59Lavery et al 1996 60Armstrong et al1998 52Lipsky et al 2012 46Simplified version of the S(AD)SAD classification Ince et al 2008 63system 61Includes ulcer site as data suggests this might bean important determ<strong>in</strong>ant of outcome 6238 BEST PRACTICEBEST PRACTICEGUIDELINESGUIDELINES:FOR SKINWOUNDAND WOUNDMANAGEMENTCARE ININEPIDERMOLYSISDIABETIC FOOTBULLOSAULCERS
DFU WOUNDMANAGEMENTDFU <strong>wound</strong> <strong>management</strong>Practitioners must strive to prevent DFUs develop<strong>in</strong>g elsewhere on the <strong>foot</strong> or onthe contralateral limb and to achieve limb preservation 64The pr<strong>in</strong>ciple aim of DFU <strong>management</strong> is<strong>wound</strong> closure 17 . More specifically, the <strong>in</strong>tentionshould be to treat the DFU at an earlystage to allow prompt heal<strong>in</strong>g 65 .The essential components of <strong>management</strong>are: Treat<strong>in</strong>g underly<strong>in</strong>g disease processes Ensur<strong>in</strong>g adequate blood supply Local <strong>wound</strong> care, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong>fectioncontrol Pressure offload<strong>in</strong>g.Effective <strong>foot</strong> care should be a partnershipbetween patients, carers and healthcareprofessionals 1,66 . This means provid<strong>in</strong>gappropriate <strong>in</strong>formation to enable patientsand carers to participate <strong>in</strong> decision mak<strong>in</strong>gand understand the rationale beh<strong>in</strong>d someof the cl<strong>in</strong>ical decisions as well as support<strong>in</strong>ggood self-care.TREATING THE UNDERLYINGDISEASE PROCESSESPractitioners should identify the underly<strong>in</strong>gcause of the DFU dur<strong>in</strong>g the patient assessmentand, where possible, correct orelim<strong>in</strong>ate it. Treat<strong>in</strong>g any severe ischaemia is criticalto <strong>wound</strong> heal<strong>in</strong>g, regardless of other<strong>in</strong>terventions 17 . It is recommended thatall patients with critical limb ischaemia,<strong>in</strong>clud<strong>in</strong>g rest pa<strong>in</strong>, ulceration and tissueloss, should be referred for considerationof arterial reconstruction 31 . Achiev<strong>in</strong>g optimal <strong>diabetic</strong> control. Thisshould <strong>in</strong>volve tight glycaemic control andmanag<strong>in</strong>g risk factors such as high bloodpressure, hyperlipidaemia and smok<strong>in</strong>g 67 .Nutritional deficiencies should also bemanaged 7 . Address<strong>in</strong>g the physical cause of thetrauma. As well as exam<strong>in</strong><strong>in</strong>g the <strong>foot</strong>,practitioners should exam<strong>in</strong>e the patient's<strong>foot</strong>wear for proper fit, wear and tear andthe presence of any foreign bodies (suchas small stones, glass fragments, draw<strong>in</strong>gp<strong>in</strong>s, pet hairs) that may traumatisethe <strong>foot</strong> 1 . When possible and appropriate,practitioners should check other <strong>foot</strong>wearworn at home and at work (eg slippersand work boots).ENSURING ADEQUATE BLOODSUPPLYA patient with acute limb ischaemia (seepage 5) is a cl<strong>in</strong>ical emergency and may beat great risk if not managed <strong>in</strong> a timely andeffective way.It is important to appreciate that, aside fromcritical limb ischaemia, decreased perfusionor impaired circulation may be an <strong>in</strong>dicatorfor revascularisation <strong>in</strong> order to achieveand ma<strong>in</strong>ta<strong>in</strong> heal<strong>in</strong>g and to avoid or delay afuture amputation 34 .OPTIMISING LOCAL WOUND CAREThe European Wound Management Association(EWMA) states that the emphasis <strong>in</strong><strong>wound</strong> care for DFUs should be on radical andrepeated debridement, frequent <strong>in</strong>spectionand bacterial control and careful moisturebalance to prevent maceration 49 . Its positiondocument on <strong>wound</strong> bed preparationsuggests the follow<strong>in</strong>g TIME framework formanag<strong>in</strong>g DFUs (see also Box 2): Tissue debridement Inflammation and <strong>in</strong>fection control Moisture balance (optimal dress<strong>in</strong>gselection) Epithelial edge advancement.Tissue debridementThere are many methods of debridementused <strong>in</strong> the <strong>management</strong> of DFUs <strong>in</strong>clud<strong>in</strong>gsurgical/sharp, larval, autolytic and, morerecently, hydrosurgery and ultrasonic 68,69 .Debridement may be a one-off procedure orit may need to be ongo<strong>in</strong>g for ma<strong>in</strong>tenanceof the <strong>wound</strong> bed 69 . The requirement forfurther debridement should be determ<strong>in</strong>edat each dress<strong>in</strong>g change. If the <strong>wound</strong> is notprogress<strong>in</strong>g, practitioners should reviewthe current treatment plan and look for anunderly<strong>in</strong>g cause of delayed heal<strong>in</strong>g (suchBOX 2: Wound bed preparationand TIME framework(adapted from 49 )Wound bed preparationis not a static concept,but a dynamic and rapidlychang<strong>in</strong>g oneThere are fourcomponents to <strong>wound</strong>bed preparation, whichaddress the differentpathophysiologicalabnormalities underly<strong>in</strong>gchronic <strong>wound</strong>s The TIME framework canbe used to apply <strong>wound</strong>bed preparation to<strong>practice</strong>BEST PRACTICE GUIDELINES: WOUND MANAGEMENT IN DIABETIC FOOT ULCERS 9