DFU WOUNDMANAGEMENTTABLE 4: General pr<strong>in</strong>ciples of bacterial <strong>management</strong> (adapted from 49 ) At <strong>in</strong>itial presentation of <strong>in</strong>fection it is important to assess its severity, take appropriatecultures and consider need for surgical procedures Optimal specimens for culture should be taken after <strong>in</strong>itial cleans<strong>in</strong>g and debridementof necrotic material Patients with severe <strong>in</strong>fection require empiric broad-spectrum antibiotic therapy,pend<strong>in</strong>g culture results. Those with mild (and many with moderate) <strong>in</strong>fection can betreated with a more focused and narrow-spectrum antibioticPatients with diabetes have immunological disturbances; therefore even bacteria regardedas sk<strong>in</strong> commensals can cause severe tissue damage and should be regardedas pathogens when isolated from correctly obta<strong>in</strong>ed tissue specimens Gram-negative bacteria, especially when isolated from an ulcer swab, are oftencolonis<strong>in</strong>g organisms that do not require targeted therapy unless the person is at riskfor <strong>in</strong>fection with those organisms Blood cultures should be sent if fever and systemic toxicity are present Even with appropriate treatment, the <strong>wound</strong> should be <strong>in</strong>spected regularly for earlysigns of <strong>in</strong>fection or spread<strong>in</strong>g <strong>in</strong>fection Cl<strong>in</strong>ical microbiologists/<strong>in</strong>fectious diseases specialists have a crucial role; laboratoryresults should be used <strong>in</strong> comb<strong>in</strong>ation with the cl<strong>in</strong>ical presentation and history toguide antibiotic selection Timely surgical <strong>in</strong>tervention is crucial for deep abscesses, necrotic tissue and forsome bone <strong>in</strong>fectionsBOX 4: Guidel<strong>in</strong>es for the useof systemic antibiotic therapyAntibiotics should be prescribedus<strong>in</strong>g local protocolsand, <strong>in</strong> complex cases, theadvice of a cl<strong>in</strong>ical microbiologistor <strong>in</strong>fectious diseasesspecialist. Avoid prescrib<strong>in</strong>gantibiotics for un<strong>in</strong>fectedulcerations. IDSA 46 offersevidence-based suggestions,which can be adapted to localneeds.http://www.idsociety.org/uploadedFiles/IDSA/Guidel<strong>in</strong>es-Patient_Care/PDF_Library/2012%20Diabetic%20Foot%20Infections%20Guidel<strong>in</strong>e.pdfIf there are cl<strong>in</strong>ical signs of <strong>in</strong>fection atdress<strong>in</strong>g change, systemic antibiotic therapyshould be started. Topical antimicrobialsare not <strong>in</strong>dicated as the only anti-<strong>in</strong>fectivetreatment for moderate or severe <strong>in</strong>fectionof deep tissue or bone 38,46 .Patients may also require debridement toremove <strong>in</strong>fected material. In addition, <strong>in</strong>fected<strong>wound</strong>s should be cleansed at eachdress<strong>in</strong>g change with sal<strong>in</strong>e or an appropriateantiseptic <strong>wound</strong> cleans<strong>in</strong>g agent.Deep tissue <strong>in</strong>fection (moderate to severe<strong>in</strong>fection)For treat<strong>in</strong>g deep tissue <strong>in</strong>fection (cellulitis,lymphangitis, septic arthritis, fasciitis): Start patients quickly on broad-spectrumantibiotics, commensurate with the cl<strong>in</strong>icalhistory and accord<strong>in</strong>g to local protocolswhere possible 37 Take deep tissue specimens or aspiratesof purulent secretions for cultures at thestart of treatment to identify specificorganisms <strong>in</strong> the <strong>wound</strong>, but do not waitfor results before <strong>in</strong>itiat<strong>in</strong>g therapy 1,37 Change to an alternate antibiotic if:— <strong>in</strong>dicated by microbiology results 46— the signs of <strong>in</strong>flammation are notimprov<strong>in</strong>g 84 Adm<strong>in</strong>ister antibiotics parenterally forall severe and some moderate <strong>in</strong>fections,and switch to the oral route when thepatient is systemically well and cultureresults are available 46 Cont<strong>in</strong>ue antibiotic therapy until the <strong>in</strong>fectionresolves, but not through to completeheal<strong>in</strong>g 46 . In most cases 1–3 weeks oftherapy is sufficient for soft tissue <strong>in</strong>fections Consider giv<strong>in</strong>g empiric therapy directedaga<strong>in</strong>st MRSA 46 :— <strong>in</strong> patients with a prior history of MRSA<strong>in</strong>fection— when the local prevalence of MRSAcolonisation or <strong>in</strong>fection is high— if the <strong>in</strong>fection is cl<strong>in</strong>ically severe.Note that the optimal duration of antibiotictreatment is not clearly def<strong>in</strong>ed andwill depend on the severity of <strong>in</strong>fection andresponse to treatment 84 .Infection <strong>in</strong> a neuroischaemic <strong>foot</strong> is oftenmore serious than <strong>in</strong> a neuropathic <strong>foot</strong>(which has a good blood supply), and thisshould <strong>in</strong>fluence antibiotic policy 49 . Antibiotictherapy should not be given as a preventivemeasure <strong>in</strong> the absence of signs of <strong>in</strong>fection(see Box 4). This is likely to cause <strong>in</strong>fectionwith more resistant pathogens.Obta<strong>in</strong> an urgent consultation with experts(eg <strong>foot</strong> surgeon) for patients who havea rapidly deteriorat<strong>in</strong>g <strong>wound</strong> that is notrespond<strong>in</strong>g to antibiotic therapy. Infectionsaccompanied by a deep abscess, extensivebone or jo<strong>in</strong>t <strong>in</strong>volvement, crepitus, substantialnecrosis or gangrene, or necrotis<strong>in</strong>gfasciitis, need prompt surgical <strong>in</strong>terventionalong with appropriate antibiotic therapy, toreduce the risk of major amputation 51,85 .Biofilms and chronic persistent <strong>in</strong>fectionPolymicrobial <strong>in</strong>fections predom<strong>in</strong>ate <strong>in</strong>severe <strong>diabetic</strong> <strong>foot</strong> <strong>in</strong>fections and thisdiversity of bacterial populations <strong>in</strong> chronic<strong>wound</strong>s, such as DFUs, may be an importantcontributor to chronicity 86,87 . Biofilms arecomplex polymicrobial communities thatdevelop on the surface of chronic <strong>wound</strong>s,which may lack the overt cl<strong>in</strong>ical signs of <strong>in</strong>fection34 . They are not visible to the naked eye andcannot be detected by rout<strong>in</strong>e cultures 88 .The microbes produce an extra-polymericsubstance that contributes to the structure ofthe biofilm. This matrix acts as a thick, slimyprotective barrier, mak<strong>in</strong>g it very difficult for312 BEST PRACTICEBEST PRACTICEGUIDELINESGUIDELINES:FOR SKINWOUNDAND WOUNDMANAGEMENTCARE ININEPIDERMOLYSISDIABETIC FOOTBULLOSAULCERS
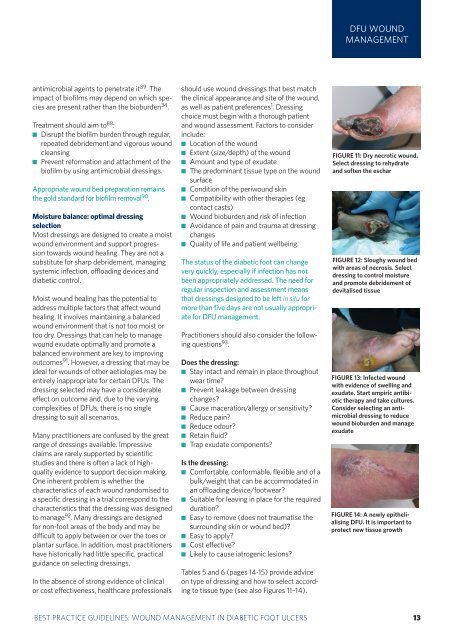
DFU WOUNDMANAGEMENTantimicrobial agents to penetrate it 89 . Theimpact of biofilms may depend on which speciesare present rather than the bioburden 34 .Treatment should aim to 88 : Disrupt the biofilm burden through regular,repeated debridement and vigorous <strong>wound</strong>cleans<strong>in</strong>g Prevent reformation and attachment of thebiofilm by us<strong>in</strong>g antimicrobial dress<strong>in</strong>gs.Appropriate <strong>wound</strong> bed preparation rema<strong>in</strong>sthe gold standard for biofilm removal 90 .Moisture balance: optimal dress<strong>in</strong>gselectionMost dress<strong>in</strong>gs are designed to create a moist<strong>wound</strong> environment and support progressiontowards <strong>wound</strong> heal<strong>in</strong>g. They are not asubstitute for sharp debridement, manag<strong>in</strong>gsystemic <strong>in</strong>fection, offload<strong>in</strong>g devices and<strong>diabetic</strong> control.Moist <strong>wound</strong> heal<strong>in</strong>g has the potential toaddress multiple factors that affect <strong>wound</strong>heal<strong>in</strong>g. It <strong>in</strong>volves ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g a balanced<strong>wound</strong> environment that is not too moist ortoo dry. Dress<strong>in</strong>gs that can help to manage<strong>wound</strong> exudate optimally and promote abalanced environment are key to improv<strong>in</strong>goutcomes 91 . However, a dress<strong>in</strong>g that may beideal for <strong>wound</strong>s of other aetiologies may beentirely <strong>in</strong>appropriate for certa<strong>in</strong> DFUs. Thedress<strong>in</strong>g selected may have a considerableeffect on outcome and, due to the vary<strong>in</strong>gcomplexities of DFUs, there is no s<strong>in</strong>gledress<strong>in</strong>g to suit all scenarios.Many practitioners are confused by the greatrange of dress<strong>in</strong>gs available. Impressiveclaims are rarely supported by scientificstudies and there is often a lack of highqualityevidence to support decision mak<strong>in</strong>g.One <strong>in</strong>herent problem is whether thecharacteristics of each <strong>wound</strong> randomised toa specific dress<strong>in</strong>g <strong>in</strong> a trial correspond to thecharacteristics that the dress<strong>in</strong>g was designedto manage 92 . Many dress<strong>in</strong>gs are designedfor non-<strong>foot</strong> areas of the body and may bedifficult to apply between or over the toes orplantar surface. In addition, most practitionershave historically had little specific, practicalguidance on select<strong>in</strong>g dress<strong>in</strong>gs.In the absence of strong evidence of cl<strong>in</strong>icalor cost effectiveness, healthcare professionalsshould use <strong>wound</strong> dress<strong>in</strong>gs that <strong>best</strong> matchthe cl<strong>in</strong>ical appearance and site of the <strong>wound</strong>,as well as patient preferences 1 . Dress<strong>in</strong>gchoice must beg<strong>in</strong> with a thorough patientand <strong>wound</strong> assessment. Factors to consider<strong>in</strong>clude: Location of the <strong>wound</strong> Extent (size/depth) of the <strong>wound</strong> Amount and type of exudate The predom<strong>in</strong>ant tissue type on the <strong>wound</strong>surface Condition of the peri<strong>wound</strong> sk<strong>in</strong> Compatibility with other therapies (egcontact casts) Wound bioburden and risk of <strong>in</strong>fection Avoidance of pa<strong>in</strong> and trauma at dress<strong>in</strong>gchanges Quality of life and patient wellbe<strong>in</strong>g.The status of the <strong>diabetic</strong> <strong>foot</strong> can changevery quickly, especially if <strong>in</strong>fection has notbeen appropriately addressed. The need forregular <strong>in</strong>spection and assessment meansthat dress<strong>in</strong>gs designed to be left <strong>in</strong> situ formore than five days are not usually appropriatefor DFU <strong>management</strong>.Practitioners should also consider the follow<strong>in</strong>gquestions 93 .Does the dress<strong>in</strong>g: Stay <strong>in</strong>tact and rema<strong>in</strong> <strong>in</strong> place throughoutwear time? Prevent leakage between dress<strong>in</strong>gchanges? Cause maceration/allergy or sensitivity? Reduce pa<strong>in</strong>? Reduce odour? Reta<strong>in</strong> fluid? Trap exudate components?Is the dress<strong>in</strong>g: Comfortable, conformable, flexible and of abulk/weight that can be accommodated <strong>in</strong>an offload<strong>in</strong>g device/<strong>foot</strong>wear? Suitable for leav<strong>in</strong>g <strong>in</strong> place for the requiredduration? Easy to remove (does not traumatise thesurround<strong>in</strong>g sk<strong>in</strong> or <strong>wound</strong> bed)? Easy to apply? Cost effective? Likely to cause iatrogenic lesions?Tables 5 and 6 (pages 14-15) provide adviceon type of dress<strong>in</strong>g and how to select accord<strong>in</strong>gto tissue type (see also Figures 11–14).FIGURE 11: Dry necrotic <strong>wound</strong>.Select dress<strong>in</strong>g to rehydrateand soften the escharFIGURE 12: Sloughy <strong>wound</strong> bedwith areas of necrosis. Selectdress<strong>in</strong>g to control moistureand promote debridement ofdevitalised tissueFIGURE 13: Infected <strong>wound</strong>with evidence of swell<strong>in</strong>g andexudate. Start empiric antibiotictherapy and take cultures.Consider select<strong>in</strong>g an antimicrobialdress<strong>in</strong>g to reduce<strong>wound</strong> bioburden and manageexudateFIGURE 14: A newly epithelialis<strong>in</strong>gDFU. It is important toprotect new tissue growthBEST PRACTICE GUIDELINES: WOUND MANAGEMENT IN DIABETIC FOOT ULCERS 13