Evaluation of IT modernisation in the NHS - NETSCC
Evaluation of IT modernisation in the NHS - NETSCC
Evaluation of IT modernisation in the NHS - NETSCC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Report to SDO for NCRS Project<strong>Evaluation</strong> <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> <strong>in</strong> <strong>the</strong> <strong>NHS</strong>A report <strong>of</strong> research project funded as:“<strong>Evaluation</strong> <strong>of</strong> <strong>the</strong> implementation <strong>of</strong> <strong>the</strong> <strong>NHS</strong> Care Record Service (NCRS)”reference: SDO/44/2003Authors:Barnaby C Reeves 1Naomi Fulop 2Jane Hendy 3Andrew Hutch<strong>in</strong>gs 4Simon Coll<strong>in</strong> 5Eugenia Priedane 4Alec M<strong>in</strong>ers 4Institutions:1 Cl<strong>in</strong>ical Trials and <strong>Evaluation</strong> Unit, University <strong>of</strong> Bristol, Level 7 Bristol RoyalInfirmary, Marlborough Street, Bristol BS2 8HW2 Department <strong>of</strong> Management, School <strong>of</strong> Social Science and Public Policy,K<strong>in</strong>g's College London, Frankl<strong>in</strong>-Wilk<strong>in</strong>s Build<strong>in</strong>g, 150 Stamford Street,London SE1 9NH3 Innovation Studies Centre, Tanaka Bus<strong>in</strong>ess School, Imperial CollegeLondon, South Kens<strong>in</strong>gton campus, London SW7 2AZ4 Health Services Research Unit, Department <strong>of</strong> Public Health and Policy,London School <strong>of</strong> Hygiene and Tropical Medic<strong>in</strong>e, Keppel Street, LondonWC1E 7HT5 Department <strong>of</strong> Social Medic<strong>in</strong>e, University <strong>of</strong> Bristol, Canynge Hall,Whiteladies Road, Bristol BS8 2PR
Report to SDO for NCRS ProjectStudy guarantors:Barnaby Reeves and Naomi Fulop are guarantors for, respectively, <strong>the</strong>quantitative and qualitative elements <strong>of</strong> <strong>the</strong> research described <strong>in</strong> <strong>the</strong> report.Acknowledgements:We are very grateful to participat<strong>in</strong>g Trusts for agree<strong>in</strong>g to be cases, and to<strong>in</strong>dividual <strong>in</strong>terviewees for <strong>the</strong>ir time and <strong>in</strong>terest <strong>in</strong> <strong>the</strong> study. They are notnamed to preserve <strong>the</strong> anonymity <strong>of</strong> <strong>the</strong> Trusts. We also thank staff whoassisted with provision <strong>of</strong> quantitative data.We are grateful to members <strong>of</strong> <strong>the</strong> Steer<strong>in</strong>g Group for <strong>the</strong>ir cont<strong>in</strong>u<strong>in</strong>g support:Dr Aileen Clarke, Mr David Lawrence, Pr<strong>of</strong> Charles Normand, Dr MichaelSoljak, Dr Ken Walton.Dr Crist<strong>in</strong>a Masseria and Mr Paco Pozo-Mart<strong>in</strong> were employed on <strong>the</strong> project forpart <strong>of</strong> its duration. We thank <strong>the</strong>m for <strong>the</strong>ir respective contributions.Fund<strong>in</strong>g:This research was funded by a grant from <strong>the</strong> Service Delivery and Organisation<strong>of</strong> Care programme <strong>of</strong> <strong>the</strong> <strong>NHS</strong> Research and Development Directorate,reference: SDO/44/2003
Report to SDO for NCRS ProjectExecutive SummaryExecutive summary1. BackgroundCaptur<strong>in</strong>g <strong>in</strong>formation accurately, communicat<strong>in</strong>g and us<strong>in</strong>g it promptly to improve <strong>the</strong>effectiveness and efficiency <strong>of</strong> health care, is central to <strong>the</strong> UK Government’s visionto modernise <strong>the</strong> <strong>NHS</strong>. It has been widely assumed that <strong>the</strong>se goals will benefitpatients, health care pr<strong>of</strong>essionals, managers and planners <strong>in</strong> <strong>the</strong> <strong>NHS</strong>.The Government’s plans for <strong>NHS</strong> <strong>modernisation</strong> have evolved over time, fromelectronic ‘patient’ and ‘health’ records to a unified National Programme forInformation Technology (NPf<strong>IT</strong>) with <strong>the</strong> creation <strong>of</strong> Connect<strong>in</strong>g for Health to manage<strong>the</strong> programme. This evolution <strong>in</strong>cluded a fundamental policy change fromdelegation <strong>of</strong> responsibility for implement<strong>in</strong>g <strong>IT</strong> <strong>modernisation</strong> to local <strong>NHS</strong>organisations, to a policy <strong>of</strong> centralised specification and procurement.The size and complexity <strong>of</strong> national programme make it <strong>the</strong> largest outsourced <strong>IT</strong>project from <strong>the</strong> public sector ever untaken. In view <strong>of</strong> previous difficulties <strong>in</strong>implement<strong>in</strong>g large scale health service <strong>IT</strong> projects, progress <strong>in</strong> achiev<strong>in</strong>g <strong>the</strong>National Programme became a key focus <strong>of</strong> <strong>in</strong>terest <strong>of</strong> this project.2. ObjectivesFollow<strong>in</strong>g <strong>the</strong> changes to government policy, our revised objectives were to:1. Describe <strong>the</strong> context for implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> <strong>in</strong> England, exam<strong>in</strong><strong>in</strong>g actualand perceived barriers, and opportunities to facilitate implementation.2. Explore how new <strong>IT</strong> applications are experienced by end-users (<strong>NHS</strong> staff),describ<strong>in</strong>g any impact on work<strong>in</strong>g practices.3. Estimate quantitative effects <strong>of</strong> implement<strong>in</strong>g specific <strong>IT</strong> applications proposed by<strong>the</strong> NPf<strong>IT</strong>.4. Review evidence about <strong>the</strong> cost-effectiveness <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> health care.
Report to SDO for NCRS ProjectExecutive Summary3. MethodsThe study sample consisted <strong>of</strong> four <strong>NHS</strong> Acute Trusts. We used a comb<strong>in</strong>ation <strong>of</strong>qualitative and quantitative methods to address our objectives, mak<strong>in</strong>g comparisonsboth with<strong>in</strong> and between organisations. We used review methods to summariseexist<strong>in</strong>g evidence for objective 4.A qualitative researcher <strong>in</strong>terviewed a range <strong>of</strong> stakeholders <strong>in</strong>volved <strong>in</strong> implement<strong>in</strong>gand us<strong>in</strong>g <strong>IT</strong> applications, and addressed objectives 1 and 2. Two levels <strong>of</strong><strong>in</strong>terviews were conducted <strong>in</strong> three stages. Level 1 <strong>in</strong>terviews (objective 1), tookplace between July and October 2004 (stage A; n=24); and between February andApril 2006 (stage A; n=25). Level 2 <strong>in</strong>terviews (objective 2) took place betweenJanuary and October 2005 (n=44). Basel<strong>in</strong>e <strong>in</strong>formation was also collected for eachstudy site data.Level 1 <strong>in</strong>terviews <strong>in</strong>vestigated (a) <strong>the</strong> <strong>in</strong>fluence <strong>of</strong> contextual factors (historical orcurrent, facilitators or barriers) on <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> applications, and (b) <strong>the</strong>impact <strong>of</strong> recent Connect<strong>in</strong>g <strong>of</strong> Health policy changes on implementation processes.Level 2 <strong>in</strong>terviews <strong>in</strong>vestigated (a) experiences <strong>of</strong> <strong>NHS</strong> staff <strong>of</strong> specific <strong>IT</strong>applications (electronic test order<strong>in</strong>g and brows<strong>in</strong>g, or computerised physician orderentry, CPOE; electronic book<strong>in</strong>g; picture archiv<strong>in</strong>g and communication systems,PACS), and (b) <strong>the</strong> impact <strong>of</strong> <strong>the</strong>se applications on work<strong>in</strong>g practices. Interviewswere semi-structured on a one-to-one basis and took about one hour. Interviewswere taped and transcribed.We applied a modified grounded <strong>the</strong>ory analytic strategy to present an analysis <strong>of</strong>processes over time. This strategy comb<strong>in</strong>ed draw<strong>in</strong>g on <strong>the</strong> literature onorganisational change, and more user-centred sociological <strong>the</strong>ories <strong>of</strong> <strong>in</strong>novationadoption and implementation, with <strong>the</strong>mes emerg<strong>in</strong>g from <strong>the</strong> data.The quantitative research used a quasi-experimental ‘controlled before-and-after’design to quantify <strong>the</strong> effects <strong>of</strong> implement<strong>in</strong>g CPOE and PACS. Indicators werecompared between trusts that did and did not implement <strong>the</strong>se <strong>IT</strong> applications dur<strong>in</strong>g<strong>the</strong> period 2000 to 2005, tak<strong>in</strong>g <strong>in</strong>to account data for a basel<strong>in</strong>e period prior toimplement<strong>in</strong>g changes. Indicators were also compared with<strong>in</strong> Trusts betweenspecialties that did and did not implement <strong>the</strong> applications dur<strong>in</strong>g <strong>the</strong> same period.
Report to SDO for NCRS ProjectExecutive SummaryTo estimate <strong>the</strong> effects <strong>of</strong> CPOE, we considered three tests: full blood count, ureaand electrolytes, and ur<strong>in</strong>e culture. For PACS, we considered three radiologicalmodalities: pla<strong>in</strong> film X-ray, computed tomography (CT), and ultrasound.Indicators were derived from a large set def<strong>in</strong>ed a priori, based partly on <strong>the</strong> <strong>NHS</strong>Efficiency Map and were classified as primary or secondary depend<strong>in</strong>g on <strong>the</strong>plausibility <strong>of</strong> a direct causal pathway between implementation and <strong>the</strong> outcome.We analysed <strong>in</strong>patient and outpatient data from <strong>the</strong> Commission<strong>in</strong>g Data Set (CDS)for 2000 to 2005, l<strong>in</strong>ked with data about target pathology and radiology tests carriedout dur<strong>in</strong>g <strong>the</strong> same period. Secondary outcomes were derived directly from <strong>the</strong> CDSdata. Individual patient data were analysed for specialties common to all four trusts.Effects were estimated by multiple regression modell<strong>in</strong>g, calculat<strong>in</strong>g robust standarderrors to take <strong>in</strong>to account cluster<strong>in</strong>g <strong>of</strong> records with<strong>in</strong> trusts and specialties.4. F<strong>in</strong>d<strong>in</strong>gsImplementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> did not progress as expected dur<strong>in</strong>g <strong>the</strong> study period.F<strong>in</strong>d<strong>in</strong>gs from Level 1 <strong>of</strong> our qualitative study were able to track <strong>the</strong> impact <strong>of</strong> thisdelay on <strong>the</strong> trusts.CPOE and PACS applications were also implemented <strong>in</strong>frequently dur<strong>in</strong>g <strong>the</strong> project.Three <strong>of</strong> four Trusts implemented aspects <strong>of</strong> PACS system, but only one Trustimplemented a ‘full’ PACS. Two Trusts implemented CPOE but, <strong>in</strong> one trust, <strong>the</strong>system was so poor it was hardly used so, <strong>in</strong> effect, had not been implemented.None <strong>of</strong> <strong>the</strong> applications studied were <strong>of</strong>ficially compliant with <strong>the</strong> NPf<strong>IT</strong>.Our quantitative and qualitative evaluations <strong>of</strong> PACs and CPOE were constra<strong>in</strong>ed tosome extent because implementation <strong>of</strong> <strong>IT</strong> applications was not as widespread asexpected when <strong>the</strong> research was commissioned. Never<strong>the</strong>less, our f<strong>in</strong>d<strong>in</strong>gs provideuseful lessons as <strong>the</strong> roll-out <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> <strong>in</strong> <strong>the</strong> <strong>NHS</strong> ga<strong>the</strong>rs pace.4.1 Qualitative f<strong>in</strong>d<strong>in</strong>gs: Level 1 – Implementation <strong>of</strong> NPf<strong>IT</strong> at local levelStage A <strong>in</strong>terviews, with senior managers and cl<strong>in</strong>icians, highlighted four key issues:(a) Trusts varied <strong>in</strong> <strong>the</strong>ir circumstances, affect<strong>in</strong>g <strong>the</strong>ir ability to implement <strong>the</strong> NPf<strong>IT</strong>.(b) The process <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> was suboptimal, lead<strong>in</strong>g to low moraleamong <strong>NHS</strong> staff responsible for implementation.
Report to SDO for NCRS ProjectExecutive Summary(c) The timetable for implementation was unrealistic, caus<strong>in</strong>g uncerta<strong>in</strong>ty. Renew<strong>in</strong>gPatient Adm<strong>in</strong>istration Systems (PAS) was a bottleneck and this rate-limit<strong>in</strong>g stepcould not be reconciled with targets for implement<strong>in</strong>g substantive <strong>IT</strong> applications.(d) Short term benefits <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> are unlikely to be sufficient to persuade<strong>NHS</strong> staff to support <strong>the</strong> programme unreservedly.These <strong>in</strong>terviews were too early to assess <strong>the</strong> success <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> but demonstratedconcern among <strong>in</strong>terviews about <strong>the</strong> process <strong>of</strong> implementation.In stage B, senior managers and cl<strong>in</strong>icians felt that <strong>the</strong> NPf<strong>IT</strong> is a highly desirableobjective. Interviewees were enthusiastic about, and supportive <strong>of</strong>, <strong>the</strong> goals <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong> but still had serious concerns, several <strong>of</strong> which were <strong>the</strong> same as before.Cont<strong>in</strong>u<strong>in</strong>g uncerta<strong>in</strong>ty was mak<strong>in</strong>g key managerial decisions about <strong>IT</strong>implementation more difficult, given <strong>the</strong> current need to make f<strong>in</strong>ancial sav<strong>in</strong>gs andachieve efficiencies. Although <strong>IT</strong> <strong>modernisation</strong> should facilitate <strong>the</strong>se goals <strong>in</strong> <strong>the</strong>longer-term, senior managers still did not know: (a) what <strong>the</strong> local costs <strong>of</strong>implementation will be; (b) when a replacement patient adm<strong>in</strong>istration systemcompliant with <strong>the</strong> programme will be available; (c) <strong>the</strong> timetable for delivery <strong>of</strong><strong>in</strong>terim applications; (d) <strong>the</strong> features <strong>of</strong> <strong>the</strong>se applications; (e) <strong>the</strong> likely benefits andefficiencies from new systems.These uncerta<strong>in</strong>ties made it difficult to prioritise local implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>.Concern was expressed about threats to patient safety from a ‘patch and mend’approach to ma<strong>in</strong>ta<strong>in</strong> exist<strong>in</strong>g systems. Trust managers wanted concrete <strong>in</strong>formationabout implementation timetables, system compatibility with <strong>the</strong> long term goals <strong>of</strong> <strong>the</strong>programme, value-for-money and better communication with Connect<strong>in</strong>g for Health.4.2 Qualitative f<strong>in</strong>d<strong>in</strong>gs: level 2 – Process and impact <strong>of</strong> implementation <strong>of</strong>PACs and CPOEWe found four factors which <strong>in</strong>fluenced <strong>the</strong> adoption <strong>of</strong> CPOE and PACS:(a) The attributes <strong>of</strong> <strong>the</strong> application; <strong>the</strong> speed, ease <strong>of</strong> use, reliability and flexibility <strong>of</strong><strong>the</strong> application were key issues.(b) The characteristics <strong>of</strong> <strong>the</strong> adopter; <strong>the</strong>se were most important early dur<strong>in</strong>gimplementation and persuad<strong>in</strong>g users who were unfamiliar with <strong>IT</strong> was a challenge.
Report to SDO for NCRS ProjectExecutive Summary(c) Implementation processes; user consultation dur<strong>in</strong>g implementation, <strong>the</strong> quality <strong>of</strong>tra<strong>in</strong><strong>in</strong>g and <strong>IT</strong> support; and creation <strong>of</strong> a ‘critical mass’ <strong>of</strong> benefit were crucial to <strong>the</strong>iruse.(d) organisational factors; <strong>the</strong> most important were that <strong>the</strong> designers andimplementers <strong>of</strong> <strong>the</strong> application understood <strong>the</strong> bus<strong>in</strong>ess process which <strong>the</strong> <strong>IT</strong> wassupport<strong>in</strong>g, availability <strong>of</strong> a strong project management team with high levelmanagement support, good team work<strong>in</strong>g with<strong>in</strong> and between departments and <strong>the</strong>ability <strong>of</strong> <strong>the</strong> organisation to work as a whole.The perceived impact <strong>of</strong> <strong>IT</strong> <strong>in</strong>novations varied accord<strong>in</strong>g to <strong>the</strong> specific application,how <strong>the</strong>y had been implemented, and relate to patient experiences, work<strong>in</strong>g practicesand safety/governance. In all cases, <strong>in</strong>terviewees reported positive and negativeexamples <strong>in</strong> <strong>the</strong>se areas but, overall, for PACs <strong>in</strong> all three Trusts and CPOE <strong>in</strong> oneTrust, <strong>the</strong> positives appear to outweigh <strong>the</strong> negatives. Very little formal measurement<strong>of</strong> <strong>the</strong>se consequences was carried out by <strong>the</strong> Trusts. These consequences areimportant, not least because <strong>the</strong> perceived positive and negative impacts <strong>of</strong> <strong>the</strong>application <strong>in</strong>fluenced its cont<strong>in</strong>ued use and wider adoption.4.3 Quantitative f<strong>in</strong>d<strong>in</strong>gs: Impact <strong>of</strong> implementation <strong>of</strong> PACs and CPOEThe size <strong>of</strong> <strong>the</strong> effects estimated for primary outcomes, e.g. a change <strong>in</strong> <strong>the</strong> volume<strong>of</strong> test order<strong>in</strong>g <strong>of</strong> 10 to 20%, was certa<strong>in</strong>ly potentially important, <strong>in</strong> that such effectswould have major implications if observed across <strong>the</strong> <strong>NHS</strong> dur<strong>in</strong>g roll out <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong>. However, <strong>the</strong>re were challenges <strong>in</strong> dist<strong>in</strong>guish<strong>in</strong>g real effects frombackground variation and <strong>in</strong> attribut<strong>in</strong>g effects to CPOE or PACS.The ma<strong>in</strong> effects <strong>of</strong> CPOE were to reduce <strong>the</strong> proportion <strong>of</strong> patients who had anypathology test at outpatient appo<strong>in</strong>tments and <strong>the</strong> number <strong>of</strong> patients who had <strong>the</strong>same test at <strong>the</strong>ir next outpatient appo<strong>in</strong>tments. These effects were observed to agreater or lesser extent for all tests that were <strong>in</strong>vestigated. These effects are alsoplausible. For some tests, CPOE also reduced <strong>the</strong> proportion <strong>of</strong> <strong>in</strong>patients hav<strong>in</strong>gpathology tests but this effect was not consistent between and with<strong>in</strong> trusts.Similar effects were observed when PACS was implemented with respect to repeatpla<strong>in</strong> X-ray films and ultrasound scans on subsequent visits. However, <strong>the</strong>re was noconsistent effect on <strong>the</strong> overall proportion <strong>of</strong> patients who had a pla<strong>in</strong> X-ray film, CTor ultrasound scans at outpatient appo<strong>in</strong>tments.
Report to SDO for NCRS ProjectExecutive SummaryVarious changes <strong>in</strong> secondary outcomes were observed but could not be attributedconfidently to implementation <strong>of</strong> CPOE and PACS. There appeared to be aconsistent reduction <strong>in</strong> <strong>the</strong> proportion <strong>of</strong> patients discharged at outpatientappo<strong>in</strong>tments after both applications were implemented.5. Future research agendaThis study has shown that it is possible to use rout<strong>in</strong>ely collected patient-level data asa basis for assess<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> technological changes on <strong>in</strong>dicators <strong>of</strong> cl<strong>in</strong>icalactivity and operational efficiency. Our technique <strong>of</strong> jo<strong>in</strong><strong>in</strong>g CDS data with <strong>the</strong>sespecialist datasets could form <strong>the</strong> basis for operational research <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong> on anationwide scale. Our study also shows that smaller studies, designed to measureeffects at a much f<strong>in</strong>er level <strong>of</strong> detail, are also necessary to understand fully <strong>the</strong>impact <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> health care.The importance <strong>of</strong> study<strong>in</strong>g a large number <strong>of</strong> trusts should not be underestimated;this will improve statistical precision but, more importantly, will allow variationbetween implement<strong>in</strong>g and non-implement<strong>in</strong>g trusts to be estimated much better. Itis important that future studies <strong>of</strong> <strong>the</strong> impact <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> <strong>in</strong>clude qualitativeanalyses <strong>of</strong> <strong>the</strong> implementation process, <strong>in</strong> order to understand what <strong>the</strong> quantitativedata are <strong>in</strong>dicat<strong>in</strong>g. Multiple case studies, such as this one, provide useful analyses,both with<strong>in</strong> and across case studies. Longitud<strong>in</strong>al studies are important <strong>in</strong> study<strong>in</strong>gimplementation processes and, when implement<strong>in</strong>g complex <strong>in</strong>novations <strong>in</strong> largeorganisations, studies need to be conducted over at least 5 years.Development <strong>of</strong> appropriate outcome measures is one example <strong>of</strong> how qualitativeand quantitative methods should be comb<strong>in</strong>ed. One way to choose outcomes is tostudy <strong>in</strong>dices which are available, easily derived from rout<strong>in</strong>e sources or which areexpected to change for reasons <strong>of</strong> face validity. A second approach is to chooseoutcomes on <strong>the</strong> basis <strong>of</strong> feedback from users experienced with <strong>IT</strong> applications, toreflect aspects <strong>of</strong> service delivery which users consider important to <strong>the</strong>ir ways <strong>of</strong>work<strong>in</strong>g and which <strong>the</strong>y believe are <strong>in</strong>fluenced by <strong>IT</strong> <strong>modernisation</strong>.One major evidence gap is <strong>the</strong> absence <strong>of</strong> high quality evaluations <strong>of</strong> <strong>the</strong> economicimplications <strong>of</strong> implement<strong>in</strong>g organisation-wide <strong>IT</strong> applications. There is an urgentneed for better evaluations <strong>of</strong> <strong>the</strong> economic and f<strong>in</strong>ancial consequences <strong>of</strong> <strong>IT</strong>
Report to SDO for NCRS ProjectExecutive Summary<strong>modernisation</strong> to help plan implementation but it is not clear that conventionalmethods are applicable to such large scale and complex <strong>in</strong>terventions. In plann<strong>in</strong>gfuture economic evaluations, we recommend that, researchers should: (a) be clearabout <strong>the</strong> exact question that needs to be addressed; (b) def<strong>in</strong>e precisely <strong>the</strong> nature<strong>of</strong> <strong>the</strong> <strong>in</strong>tervention; (c) study and value health as well as resource consequences <strong>of</strong> <strong>IT</strong>implementation; (d) study <strong>the</strong> transition from <strong>the</strong> exist<strong>in</strong>g method <strong>of</strong> provid<strong>in</strong>g healthto <strong>the</strong> new method based on <strong>the</strong> <strong>in</strong>novation be<strong>in</strong>g studied; (e) study <strong>the</strong> <strong>in</strong>terventionfor long enough to describe longer term effects.This study has taken place at <strong>the</strong> very beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>g anational <strong>IT</strong> system at local level. However <strong>IT</strong> policy develops <strong>in</strong> <strong>the</strong> future, it will beimportant to cont<strong>in</strong>ue to study <strong>the</strong> processes <strong>of</strong> implementation and <strong>the</strong> impact <strong>the</strong>yhave on organisations, teams, and patient care.6. Implications for a national <strong>IT</strong> systemAn important lesson from our study is <strong>the</strong> difficulty <strong>in</strong> achiev<strong>in</strong>g an appropriatebalance <strong>of</strong> responsibility between government and local health care systems.Devolv<strong>in</strong>g control <strong>of</strong> <strong>IT</strong> to local managers results <strong>in</strong> a lack <strong>of</strong> standards, and disparatefunctionality. However, with central control, <strong>the</strong> sheer size <strong>of</strong> <strong>the</strong> task makescommunication and realistic goal sett<strong>in</strong>g difficult. The NPf<strong>IT</strong> has not made <strong>the</strong>progress that was expected and senior <strong>NHS</strong> staff warned <strong>of</strong> <strong>the</strong> cont<strong>in</strong>u<strong>in</strong>gchallenges ahead. The process <strong>of</strong> implementation needs to change rapidly for <strong>NHS</strong>staff to feel optimistic and to embrace <strong>IT</strong> changes with enthusiasm.A third strategy is now <strong>in</strong> place, sett<strong>in</strong>g central standards but with localimplementation. The role <strong>of</strong> Connect<strong>in</strong>g for Health is shift<strong>in</strong>g from implementationtowards provid<strong>in</strong>g a national <strong>in</strong>frastructure and standards-sett<strong>in</strong>g body.Implementation will be devolved more locally. Even with <strong>the</strong>se changes, <strong>the</strong> issuesraised <strong>in</strong> our study still need to be addressed. Connect<strong>in</strong>g for Health still needs to<strong>in</strong>volve local end users <strong>in</strong> discussions about <strong>the</strong> form <strong>the</strong> national <strong>in</strong>frastructure andnational standards; <strong>the</strong>se should not be imposed. Fur<strong>the</strong>r, devolv<strong>in</strong>g responsibility forimplementation locally raises questions about <strong>the</strong> degree <strong>of</strong> local customisationpermitted. We found that local customisation is an important factor <strong>in</strong> successfuladoption. However, too much customisation might weaken national standards and
Report to SDO for NCRS ProjectExecutive Summary<strong>the</strong> ability to pass data between providers. F<strong>in</strong>ally, a national <strong>in</strong>frastructure needs tohelp trusts to prioritise <strong>IT</strong> <strong>modernisation</strong> aga<strong>in</strong>st compet<strong>in</strong>g f<strong>in</strong>ancial pressures, e.g.by its <strong>in</strong>clusion <strong>in</strong> performance management frameworks. New plans need to becommunicated throughout <strong>the</strong> <strong>NHS</strong> with clear timetables to end <strong>the</strong> uncerta<strong>in</strong>ty.7. Implications for local implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong>novationsBoth studies, <strong>of</strong> NPf<strong>IT</strong> implementation at local level and end users’ views <strong>of</strong> specific<strong>IT</strong> applications, have implications at <strong>the</strong> local level <strong>in</strong> <strong>the</strong> <strong>NHS</strong>. The importance <strong>of</strong> <strong>the</strong>attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation, characteristics <strong>of</strong> <strong>the</strong> adopter, implementation processes,and organisational factors need to be addressed.The CPOE application <strong>in</strong> one Trust, and <strong>the</strong> PACS <strong>in</strong> ano<strong>the</strong>r, were considered bymanagers and end-users to have been successful implementations, preced<strong>in</strong>g byseveral years <strong>the</strong> roll-out <strong>of</strong> similar applications under NPf<strong>IT</strong>. It is possible that CPOEand PACS, when fully <strong>in</strong>tegrated with <strong>the</strong> o<strong>the</strong>r <strong>IT</strong> systems which comprise NPf<strong>IT</strong>(national electronic health records, PAS, electronic book<strong>in</strong>g, etc), will contribute tomore dramatic quantitative changes.In <strong>the</strong> longer term, <strong>the</strong> issue <strong>of</strong> where responsibility for local implementation lies, atnational or local level, rema<strong>in</strong>s. In <strong>the</strong> meantime, evidence to support <strong>the</strong>procurement and implementation <strong>of</strong> <strong>IT</strong> systems by health care providers falls far short<strong>of</strong> that required to <strong>in</strong>form changes <strong>in</strong> cl<strong>in</strong>ical practice by <strong>the</strong>se same providers.8. ConclusionsThis study is one <strong>of</strong> <strong>the</strong> few carried out on <strong>the</strong> early stages <strong>of</strong> implementation <strong>of</strong> <strong>the</strong>national <strong>IT</strong> programme for <strong>the</strong> <strong>NHS</strong> <strong>in</strong> England. It provides useful <strong>in</strong>sights <strong>in</strong>to <strong>the</strong>challenges <strong>of</strong> attempt<strong>in</strong>g this very ambitious programme, from <strong>the</strong> perspective <strong>of</strong> <strong>the</strong>local level. It also provides data on <strong>the</strong> processes and impact <strong>of</strong> implement<strong>in</strong>gspecific <strong>IT</strong> applications on a scale not achieved before. The study has significantimplications for <strong>the</strong> future direction <strong>of</strong> <strong>NHS</strong> <strong>IT</strong> policy. We have also raised importantmethodological issues for future studies <strong>of</strong> large scale <strong>IT</strong> implementation <strong>in</strong> healthcare.
Report to SDO for NCRS ProjectExecutive SummaryContents1. Introduction................................................................................................................. 11.1. Orig<strong>in</strong>al conception <strong>of</strong> <strong>the</strong> project ....................................................................11.2. Changes to <strong>the</strong> conception <strong>of</strong> <strong>the</strong> project ........................................................21.3. Additional changes dur<strong>in</strong>g <strong>the</strong> course <strong>of</strong> <strong>the</strong> project ........................................71.4. Outl<strong>in</strong>e <strong>of</strong> <strong>the</strong> report.........................................................................................92. Literature to support <strong>the</strong> <strong>in</strong>vestigation <strong>of</strong> <strong>the</strong> study objectives ................................ 132.1. Literature search strategies ...........................................................................132.2. Difficulties <strong>in</strong> evaluat<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> EPRs..................................................142.3. Organisational research exam<strong>in</strong><strong>in</strong>g EPR implementation ..............................162.4. Organisational research exam<strong>in</strong><strong>in</strong>g CPOE implementation ...........................182.5. Research exam<strong>in</strong><strong>in</strong>g implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong>.............................202.6. Conclusions...................................................................................................223. Systematic review <strong>of</strong> <strong>the</strong> economic implications <strong>of</strong> large scale <strong>IT</strong>implementation <strong>in</strong> health care................................................................................ 243.1. Introduction ...................................................................................................243.2. Background <strong>in</strong>formation on <strong>IT</strong> implementation...............................................243.3. Methods ........................................................................................................253.4. Results..........................................................................................................283.5. Discussion.....................................................................................................374. Methods for <strong>the</strong> qualitative and quantitative empirical elements <strong>of</strong> <strong>the</strong> study ........ 404.1. Ethics ............................................................................................................404.2. Methods for <strong>the</strong> qualitative study...................................................................404.3. Methods for <strong>the</strong> quantitative study.................................................................525. Qualitative f<strong>in</strong>d<strong>in</strong>gs from Level 1: Implementation <strong>of</strong> NPf<strong>IT</strong> at local level............... 605.1. Stage a.: results ............................................................................................605.2. Stage b.: results ............................................................................................675.3. Summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gs......................................................................................756. Qualitative f<strong>in</strong>d<strong>in</strong>gs from Level 2: implementation <strong>of</strong> specific e-functions .............. 776.1. Introduction ...................................................................................................776.2. Background to <strong>IT</strong> applications .......................................................................776.3. F<strong>in</strong>d<strong>in</strong>gs ........................................................................................................796.4. Summary <strong>of</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gs.............................................................................907. Quantitative results .................................................................................................. 927.1. Information about participat<strong>in</strong>g Trusts............................................................927.2. CPOE association with primary outcomes.....................................................927.3. PACS association with primary outcomes .....................................................937.4. Secondary outcomes.....................................................................................977.5. Summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gs....................................................................................105
Report to SDO for NCRS ProjectExecutive Summary8. Discussion .............................................................................................................. 1098.1. Introduction .................................................................................................1098.2. Summary <strong>of</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gs...........................................................................1098.3. Strengths and weaknesses <strong>of</strong> <strong>the</strong> study ......................................................1138.4. F<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> <strong>the</strong> context <strong>of</strong> exist<strong>in</strong>g literature.................................................1198.5. Research.....................................................................................................1238.6. Implications for a National <strong>IT</strong> System ..........................................................1288.7. Implications for local implementation <strong>of</strong> <strong>IT</strong> applications ...............................1298.8. Conclusions.................................................................................................1319. References ............................................................................................................. 132
Report to SDO for NCRS ProjectExecutive SummaryTable <strong>of</strong> abbreviationsAbbreviationA&EADEAHPCDSCfHCPOECPRSCRSCTDoHDOIEHREPREMRERDIPFBCGPHESICP<strong>IT</strong><strong>IT</strong>UIM&TLISLoSLSPAccident & EmergencyAdverse drug eventAllied health pr<strong>of</strong>essionalCommission<strong>in</strong>g Data SetConnect<strong>in</strong>g for HealthDescription <strong>of</strong> abbreviationComputerised physician order entry (USA); electronic test order<strong>in</strong>gand brows<strong>in</strong>g (UK)Computerized Patient Record SystemCare Record ServiceComputed TomographyDepartment <strong>of</strong> HealthDiffusion <strong>of</strong> InnovationsElectronic health recordElectronic patient recordElectronic medical recordElectronic Record Development and Implementation ProgrammeFull blood countGeneral PracticeHospital Episode StatisticsIntegrated care pathwayInformation TechnologyIntensive <strong>the</strong>rapy unitInformation Management and TechnologyLaboratory Information SystemLength <strong>of</strong> StayLocal Service Provider
Report to SDO for NCRS ProjectExecutive SummaryAbbreviationM<strong>IT</strong>MeSHNCRS<strong>NHS</strong>NPf<strong>IT</strong>NPVNSFNSWNWCSPACSPASPCPCISPFRISRCTSUIUCUEUSVAVISNsDescription <strong>of</strong> abbreviationMassachusetts Institute <strong>of</strong> TechnologyMedical Subject Head<strong>in</strong>g<strong>NHS</strong> Care Record ServiceNational Health ServiceNational Programme for Information TechnologyNet Present ValueNational Service FrameworkNew South Wales<strong>NHS</strong>-wide Clear<strong>in</strong>g ServicePicture archive and communication systemPatient Adm<strong>in</strong>istration SystemPersonal computerPatient Care Information SystemPla<strong>in</strong> FilmRadiology Information SystemRandomized controlled trialSerious untoward <strong>in</strong>cidentUr<strong>in</strong>e cultureUrea and electrolytesUltrasoundVeterans’ AffairsVeterans’ Integrated Services Networks
Report to SDO for NCRS ProjectIntroduction1. Introduction1.1. Orig<strong>in</strong>al conception <strong>of</strong> <strong>the</strong> projectCaptur<strong>in</strong>g <strong>in</strong>formation accurately, communicat<strong>in</strong>g and us<strong>in</strong>g <strong>the</strong> <strong>in</strong>formationpromptly to improve <strong>the</strong> effectiveness and efficiency <strong>of</strong> health care, is central to<strong>the</strong> UK Government’s vision <strong>of</strong> modernis<strong>in</strong>g <strong>the</strong> <strong>NHS</strong>. 1In <strong>the</strong> White Paperpublished <strong>in</strong> 1998, Information for Health, <strong>IT</strong> <strong>modernisation</strong> was described asfocus<strong>in</strong>g on <strong>the</strong> establishment <strong>of</strong> high quality <strong>in</strong>formation systems with<strong>in</strong><strong>in</strong>stitutions, to capture data “describ<strong>in</strong>g <strong>the</strong> record <strong>of</strong> periodic care provided ma<strong>in</strong>lyby one <strong>in</strong>stitution”, i.e. <strong>the</strong> electronic patient record (EPR). Implementation <strong>of</strong>EPRs is a crucial step towards <strong>the</strong> longer term goal <strong>of</strong> electronic health records,which will provide “a longitud<strong>in</strong>al record <strong>of</strong> patient’s health and health care – fromcradle to grave.” 1The White Paper identified five key functions <strong>of</strong> EPRs:(a) Electronic book<strong>in</strong>g (out-patients, elective surgery and emergency referrals);(b) Electronic order<strong>in</strong>g <strong>of</strong> tests and <strong>in</strong>vestigations and electronic access to, or‘brows<strong>in</strong>g’ <strong>of</strong>, test results (i.e. described here as “computerised physician orderentry”, or CPOE, follow<strong>in</strong>g <strong>the</strong> North American literature);(c) Electronic communication with<strong>in</strong> and between acute Trusts and betweensecondary and primary care sectors;(d) Prescrib<strong>in</strong>g (e.g. automatic prescrib<strong>in</strong>g /dispens<strong>in</strong>g <strong>of</strong> medications specified <strong>in</strong>discharge summaries);(e) Picture Archive and Communication Systems (PACS; provid<strong>in</strong>g <strong>the</strong> same <strong>the</strong>functions as electronic order<strong>in</strong>g <strong>of</strong> tests)At this time, EPRs were considered to br<strong>in</strong>g benefits to patients, health carepr<strong>of</strong>essionals, managers and planners <strong>in</strong> <strong>the</strong> <strong>NHS</strong>. Table 1 describes our orig<strong>in</strong>alframework sett<strong>in</strong>g out potential quantifiable consequences <strong>of</strong> implement<strong>in</strong>g EPRsand <strong>the</strong> potential benefits <strong>of</strong> <strong>the</strong>se consequences for <strong>the</strong> different groups.Additional potential benefits span <strong>the</strong>se functions, for example:• Electronic <strong>in</strong>tegrated care pathways (ICPs): more effective cl<strong>in</strong>icalmanagement through implementation <strong>of</strong> structured care pathways, improvedCl<strong>in</strong>ical Governance, high quality data to demonstrate <strong>the</strong>se benefits.• ‘Seamless’ care: secure but accessible <strong>in</strong>formation to all caregivers <strong>in</strong>volved <strong>in</strong>health care delivery.1
Report to SDO for NCRS ProjectIntroduction• Automated and secure audit trail for decisions, us<strong>in</strong>g electronicf<strong>in</strong>gerpr<strong>in</strong>ts/signatures.• More accurate, and more readily available, <strong>in</strong>formation for plann<strong>in</strong>g andperformance monitor<strong>in</strong>g purposes locally; more accurate data returns fornational purposes achieved more efficiently.Our orig<strong>in</strong>al aim was to evaluate <strong>the</strong> implementation <strong>of</strong> electronic patient records(EPRs) <strong>in</strong> four ma<strong>in</strong> areas: processes; consequences, both <strong>in</strong>tended andun<strong>in</strong>tended; <strong>the</strong> associated costs and sav<strong>in</strong>gs <strong>of</strong> <strong>the</strong> processes andconsequences; lessons for future implementation. We described two specificobjectives:(a) To evaluate <strong>the</strong> consequences and costs/sav<strong>in</strong>gs <strong>of</strong> implement<strong>in</strong>g EPRs <strong>in</strong> arange <strong>of</strong> secondary acute Trusts;(b) To evaluate <strong>the</strong> processes and impact <strong>of</strong> implement<strong>in</strong>g EPRs on <strong>the</strong>organisation, all levels <strong>of</strong> staff and patients.Information for Health required all acute Trusts to implement EPRs. 1At <strong>the</strong> time<strong>of</strong> f<strong>in</strong>alis<strong>in</strong>g <strong>the</strong> project <strong>in</strong> 2003, <strong>the</strong> target date for achiev<strong>in</strong>g full implementationwas rescheduled to December 2007, 2 with <strong>the</strong> Government acknowledg<strong>in</strong>g thatEPRs had “not yet been adopted on a national scale”. At <strong>the</strong> time, we saw a clearopportunity for <strong>the</strong> study to identify important lessons for implementation. EPRswere also be<strong>in</strong>g implemented <strong>in</strong> “different ways” across acute Trusts. SomeTrusts had <strong>the</strong> advantage <strong>of</strong> ‘new build’ projects, which allowed <strong>the</strong> ‘hardware’and ‘s<strong>of</strong>tware’ <strong>in</strong>frastructure for EPRs to be <strong>in</strong>stalled <strong>in</strong> an optimal fashion. O<strong>the</strong>rTrusts were establish<strong>in</strong>g EPR functionality by modify<strong>in</strong>g exist<strong>in</strong>g <strong>IT</strong> systems.1.2. Changes to <strong>the</strong> conception <strong>of</strong> <strong>the</strong> projectIn November 2003, <strong>the</strong> SDO agreed that changes to <strong>the</strong> project protocol wererequired. These changes were needed because <strong>the</strong> government’s orig<strong>in</strong>al planfor implement<strong>in</strong>g electronic patient records (EPRs) <strong>in</strong> <strong>the</strong> <strong>NHS</strong> (on which ourapplication and orig<strong>in</strong>al objectives were based) 1,2 had been abandoned dur<strong>in</strong>g <strong>the</strong>period between submission <strong>of</strong> <strong>the</strong> application and contract<strong>in</strong>g <strong>of</strong> <strong>the</strong> project.2
Report to SDO for NCRS ProjectIntroductionTable 1: Illustrative consequences and potential benefits to patients, healthcare pr<strong>of</strong>essionals and managers <strong>of</strong> implement<strong>in</strong>g EPRs. Adaptedfrom <strong>in</strong>formation provided by participat<strong>in</strong>g Trusts.EPR functionsPotential consequences (<strong>in</strong>tended ‘benefits’) for:(operational change) Patient Pr<strong>of</strong>essional Manager2 Book<strong>in</strong>g (out-patient and <strong>in</strong>patient)• patient history available forOP appo<strong>in</strong>tments• date and time allocated attime <strong>of</strong> referral• allow book<strong>in</strong>g <strong>of</strong> urgent /next day OP appo<strong>in</strong>tments• allow emergency admissionto ward• referral at time to suitpatient• patient notified <strong>of</strong> dateat earliest possible time• reduce / avoid OP wait• <strong>in</strong>formation availablefor cl<strong>in</strong>ical decisionmak<strong>in</strong>g• avoid A&E wait; moreappropriate / timelymanagement• reasons for referralalways available• more timely cl<strong>in</strong>icaldecision mak<strong>in</strong>g• referral aga<strong>in</strong>st agreedprotocols reduces timereview<strong>in</strong>g referrals• cl<strong>in</strong>ics scheduled <strong>in</strong>accordance withprotocols• avoid <strong>in</strong>appropriateadmissions• avoid A&E attendances• reduce time spent byOP staff <strong>in</strong> search<strong>in</strong>gfor patient history,preparation <strong>of</strong> notes,etc.• fewer missedappo<strong>in</strong>tments• reduce adm<strong>in</strong>istrativetime deal<strong>in</strong>g withreferrals / book<strong>in</strong>gs• avoid <strong>in</strong>appropriateadmissions• avoid A&E attendance3 Test order<strong>in</strong>g and brows<strong>in</strong>g<strong>of</strong> results (Biochemistry,Pathology, Microbiology,text results for Radiology)• tests ordered electronically• test results availableelectronically4 Inter-pr<strong>of</strong>essionalcommunication• ‘automated’ cl<strong>in</strong>ic lettersproduced ‘automatically’,with added free text• automated dischargesummaries, with added freetext5 Prescrib<strong>in</strong>g• highlight contra-<strong>in</strong>dications• apply prescrib<strong>in</strong>gguidel<strong>in</strong>es, e.g. NSF• co-ord<strong>in</strong>ation withdischarge plans6 PACS• same changes forradiological images as foro<strong>the</strong>r tests, see 2 above• avoid unnecessarytests• tests carried out moreefficiently• avoid duplicate test<strong>in</strong>g• more timely cl<strong>in</strong>icaldecision mak<strong>in</strong>g• avoid duplicate test<strong>in</strong>g• <strong>in</strong>formation about cl<strong>in</strong>icdecisions available toGPs, etc. quicker• <strong>in</strong>formation about aftercareavailable to GPs,etc. quicker, withquicker implementation<strong>of</strong> after-care plan• discharges occurpromptly• GPs can implementafter-care quicker• avoid adverse drug<strong>in</strong>teractions• ensures appropriatemedication• avoids delay <strong>in</strong>discharge• benefits as for o<strong>the</strong>rtests (see 2 above)• reduce time spentorder<strong>in</strong>g tests• <strong>in</strong>troduce ICPs at <strong>the</strong>earliest po<strong>in</strong>t <strong>in</strong> <strong>the</strong>patient’s care• avoid cl<strong>in</strong>ical delay / reorder<strong>in</strong>gwhen testresults miss<strong>in</strong>g• more timely cl<strong>in</strong>icaldecision mak<strong>in</strong>g• time reduced dictat<strong>in</strong>gletters• <strong>in</strong>formation quicklyavailable to o<strong>the</strong>rs, e.g.GPs• time reduced dictat<strong>in</strong>gletters• <strong>in</strong>formation quicklyavailable to o<strong>the</strong>rs, e.g.GPs• avoid adverse drug<strong>in</strong>teractions• promotes effective andefficient care• reduces time spentchas<strong>in</strong>g / collect<strong>in</strong>gmedications• benefits as for o<strong>the</strong>rtests (see 2 above)• reduction <strong>in</strong> <strong>the</strong> number<strong>of</strong> tests and<strong>in</strong>vestigations ordered• allows test protocols tobe established, e.g. forpreadmission• elim<strong>in</strong>ation <strong>of</strong> test orderpaper forms• reduce re-order<strong>in</strong>g <strong>of</strong>tests when results aremiss<strong>in</strong>g• elim<strong>in</strong>ation <strong>of</strong> paperresults• less requirement fortime <strong>of</strong> medicalsecretaries• less requirement fortime <strong>of</strong> junior doctors• avoid adverse drug<strong>in</strong>teractions• promotes effective andefficient care• avoids delay <strong>in</strong>discharge• benefits as for o<strong>the</strong>rtests (see 2 above)3
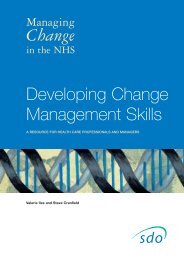
Report to SDO for NCRS ProjectIntroductionBy <strong>the</strong> spr<strong>in</strong>g <strong>of</strong> 2002, just 3% <strong>of</strong> trusts were set to meet this target <strong>of</strong> achiev<strong>in</strong>gsome EPR functionality. 3 The Treasury’s Wanless report <strong>in</strong> 2002 suggested twoma<strong>in</strong> reasons for this: budgets for <strong>in</strong>formation technology (<strong>IT</strong>), allocated locally,were be<strong>in</strong>g used to relieve f<strong>in</strong>ancial pressures elsewhere, and <strong>the</strong> process <strong>of</strong>sett<strong>in</strong>g <strong>of</strong> central <strong>IT</strong> standards was <strong>in</strong>adequate. 4 The report recommended r<strong>in</strong>gfenc<strong>in</strong>g and doubl<strong>in</strong>g <strong>the</strong> <strong>IT</strong> budget. The government responded with £2.3bn for anew National Programme for Information Technology (NPf<strong>IT</strong>) <strong>in</strong> <strong>the</strong> <strong>NHS</strong> <strong>in</strong>England. 5 In November 2003, <strong>the</strong>re were still considerable uncerta<strong>in</strong>ties about<strong>the</strong> NPf<strong>IT</strong>.The first progress report for this project covered <strong>the</strong> period from October 2003 toJune 2004. It was extended to cover n<strong>in</strong>e months with <strong>the</strong> <strong>in</strong>tention that <strong>the</strong> researchteam should propose changes to <strong>the</strong> study protocol <strong>in</strong> light <strong>of</strong> (a) <strong>the</strong> government’semerg<strong>in</strong>g new <strong>IT</strong> strategy and (b) discussions with participat<strong>in</strong>g Trusts about how <strong>the</strong>new strategy would impact on <strong>the</strong>ir local plans for implementation <strong>of</strong> EPRs.Orig<strong>in</strong>ally, <strong>the</strong> government drew a clear dist<strong>in</strong>ction between EPRs and electronichealth records (EHRs). The former were <strong>in</strong>tended to cover <strong>the</strong> management anddocumentation <strong>of</strong> s<strong>in</strong>gle health care episodes, whereas <strong>the</strong> latter were <strong>in</strong>tended to besummary longitud<strong>in</strong>al records (“cradle to grave”) <strong>of</strong> key health <strong>in</strong>formation for<strong>in</strong>dividuals. In <strong>the</strong> NPf<strong>IT</strong>, this dist<strong>in</strong>ction was dropped, with aspects <strong>of</strong> electronicmanagement and documentation <strong>of</strong> care <strong>in</strong>tegrated and referred to as <strong>the</strong> <strong>NHS</strong> CareRecord Service (NCRS).A more fundamental change was <strong>the</strong> switch from a policy <strong>of</strong> delegat<strong>in</strong>g responsibilityfor implement<strong>in</strong>g <strong>IT</strong> <strong>modernisation</strong> to local <strong>NHS</strong> organisations, to a policy <strong>of</strong>centralised specification and procurement. 5 Key features <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> were str<strong>in</strong>gentnational data and <strong>IT</strong> standards, procured and paid for nationally. Implementation <strong>in</strong>acute trusts was through one <strong>of</strong> five geographic partnerships with <strong>in</strong>dustry, called“clusters”, with <strong>IT</strong> applications be<strong>in</strong>g provided by a local service provider (LSP) foreach geographic area contract by <strong>the</strong> NPf<strong>IT</strong> through a process <strong>of</strong> nationalcompetitive tender<strong>in</strong>g. The ma<strong>in</strong> national features were a new national network<strong>in</strong>gservice provid<strong>in</strong>g broadband, called “N3”; electronic book<strong>in</strong>g, called “choose andbook”; electronic transfer <strong>of</strong> prescriptions; and a nationally accessible, “cradle tograve” summary patient record called “<strong>the</strong> sp<strong>in</strong>e”(Figure 1). The provision <strong>of</strong>4
Report to SDO for NCRS ProjectIntroductionelectronic functions at acute trust level formed part <strong>of</strong> <strong>the</strong> NCRS, a collective term forall aspects <strong>of</strong> cl<strong>in</strong>ical <strong>IT</strong> support applications, from cl<strong>in</strong>ical decision mak<strong>in</strong>g tools todigital X-rays.The size, complexity, and <strong>in</strong>novation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> made it <strong>the</strong> largest outsourced <strong>IT</strong>project from <strong>the</strong> public sector ever untaken. 6In view <strong>of</strong> previous difficulties <strong>in</strong>implement<strong>in</strong>g large scale health service <strong>IT</strong> projects, both <strong>in</strong> <strong>the</strong> United K<strong>in</strong>gdom ando<strong>the</strong>r countries, 7 ,8 progress <strong>in</strong> achiev<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> became a key focus <strong>of</strong> <strong>in</strong>terest. In2004, <strong>the</strong> Department <strong>of</strong> Health established a new agency, Connect<strong>in</strong>g for Health,with responsibility for manag<strong>in</strong>g <strong>the</strong> delivery <strong>of</strong> NPf<strong>IT</strong>.Figure 1: Elements that make up <strong>the</strong> National Programme for InformationTechnology5
Report to SDO for NCRS ProjectIntroductionTable 2: Relationship between orig<strong>in</strong>al and revised protocolsPolicy change Consequence Plan <strong>in</strong> orig<strong>in</strong>al protocol Revision to study protocol Impact on study outputsNCRSimplementationis now under <strong>the</strong>remit <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong> and <strong>IT</strong>applications areto be suppliedvia <strong>the</strong> LSPOrganisationaluncerta<strong>in</strong>tyTwo levels <strong>of</strong> qualitativeanalysis:1. Staff (use <strong>of</strong> EPRs)2. Patients (careprocess)Include a third level <strong>of</strong>qualitative analysis -1. Management team(organisational context)2. Staff (use <strong>of</strong> NCRS)3. Patients (care process)<strong>Evaluation</strong> <strong>of</strong> <strong>the</strong> organisationalimpact <strong>of</strong> NPf<strong>IT</strong> policy changes,on NCRS implementation, atacute trust level.Low levels <strong>of</strong>NCRSimplementationEvaluate 5 EPR functions1. e-book<strong>in</strong>g2. e-test order<strong>in</strong>g3. PACS4. e-communications5. e-prescrib<strong>in</strong>gEvaluate 3 NCRS – thosefunctions most widely <strong>in</strong> placedur<strong>in</strong>g <strong>the</strong> study time-frame.1. e-book<strong>in</strong>g2. e-test order<strong>in</strong>g3. PACSThe reduction <strong>in</strong> <strong>the</strong> number <strong>of</strong>functions evaluated meanssome macro level (acrossTrust) analysis will be replacedby micro (with<strong>in</strong> trust)evaluation, both for quantitativeand qualitative aspects <strong>of</strong> <strong>the</strong>study.Low levels <strong>of</strong>NCRSimplementationQualitatively evaluate <strong>the</strong>impact <strong>of</strong> EPRs on patientsby exam<strong>in</strong><strong>in</strong>g two types <strong>of</strong>patient journey, hipreplacement and stroke.Qualitatively evaluate <strong>the</strong>impact <strong>of</strong> e-functions bytarget<strong>in</strong>g patients whose carehas taken place <strong>in</strong> areas <strong>in</strong>which e-functions have beendeployed.Evaluat<strong>in</strong>g <strong>the</strong> process <strong>of</strong>patient care via specific NCRSe-functions expected to<strong>in</strong>fluence care will optimise <strong>the</strong>probability <strong>of</strong> captur<strong>in</strong>g change.NCRS – <strong>NHS</strong> Care Record Service; NPf<strong>IT</strong> – <strong>the</strong> National Programme for Information Technology; <strong>IT</strong> – <strong>in</strong>formation technology; LSP –local service provider; EPR – electronic patient record; PACS – picture archiv<strong>in</strong>g and communication system.6
Report to SDO for NCRS ProjectIntroductionRevisions to <strong>the</strong> study protocol necessitated by <strong>the</strong> policy change <strong>in</strong> modernis<strong>in</strong>g <strong>IT</strong><strong>in</strong> <strong>the</strong> <strong>NHS</strong> are set out <strong>in</strong> Table 2. Our revised objectives were to:1. Describe <strong>the</strong> context for implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> <strong>in</strong> England, exam<strong>in</strong><strong>in</strong>gactual and perceived barriers, and opportunities to facilitate implementation.2. Explore how new electronic functionality is experienced by end-users (<strong>NHS</strong> staff),describ<strong>in</strong>g any impact on work<strong>in</strong>g practices.3. Determ<strong>in</strong>e any quantitative benefits achieved by implement<strong>in</strong>g specific <strong>IT</strong>systems proposed by <strong>the</strong> NPf<strong>IT</strong>.4. Evaluate <strong>the</strong> economic evidence for <strong>the</strong> cost-effectiveness <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> healthcare.1.3. Additional changes dur<strong>in</strong>g <strong>the</strong> course <strong>of</strong> <strong>the</strong> projectThe level <strong>of</strong> implementation <strong>of</strong> applications dur<strong>in</strong>g <strong>the</strong> course <strong>of</strong> <strong>the</strong> project was low(see Tables 3, 4 and 5). In <strong>the</strong> orig<strong>in</strong>al specification <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>, <strong>IT</strong> applicationssuch as picture archiv<strong>in</strong>g and communication systems (PACS) and e-test order<strong>in</strong>gand brows<strong>in</strong>g (i.e. computerised physician order entry, CPOE) at <strong>the</strong> level <strong>of</strong> acutetrusts were to be founded on new, replacement PAS designed to be compliant with<strong>the</strong> national <strong>IT</strong> structure required to make <strong>the</strong> NPf<strong>IT</strong> a reality. However, noreplacement PAS were <strong>in</strong>stalled dur<strong>in</strong>g <strong>the</strong> time course <strong>of</strong> this research project.Because <strong>of</strong> <strong>the</strong> low level <strong>of</strong> implementation, we had to drop our <strong>in</strong>tention to evaluate<strong>the</strong> processes and consequences <strong>of</strong> electronic book<strong>in</strong>g, “choose and book”. Onlyone trust <strong>in</strong> our study attempted to implement electronic book<strong>in</strong>g, as a pilot.Unfortunately, implementation was slow due to technical difficulties, a lack <strong>of</strong> GPbuy-<strong>in</strong> to <strong>the</strong> scheme, and wider problems with <strong>the</strong> <strong>in</strong>terface between primary andsecondary care. Comments about electronic book<strong>in</strong>g made by <strong>in</strong>terviewees dur<strong>in</strong>g<strong>in</strong>terviews were noted, but this <strong>IT</strong> application could not be studied quantitatively.The switch from a local to national focus meant that our orig<strong>in</strong>al <strong>in</strong>tention to study <strong>the</strong>bus<strong>in</strong>ess cases set out by participat<strong>in</strong>g trusts to justify <strong>the</strong> <strong>in</strong>vestment required forEPRs was no longer relevant. The creation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> meant that <strong>the</strong> ma<strong>in</strong> costswere <strong>in</strong>tended to be shifted from acute trusts to <strong>the</strong> NPf<strong>IT</strong>, with decisions about7
Report to SDO for NCRS ProjectIntroductionimplementation effectively taken out <strong>of</strong> <strong>the</strong> hands <strong>of</strong> trust boards. Therefore, wedecided to carry out a systematic review <strong>of</strong> economic evaluations <strong>of</strong> large-scalehealth care <strong>IT</strong> implementations to meet our fourth objective, to evaluate <strong>the</strong>economic evidence for <strong>the</strong> cost-effectiveness <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> health care.Figure 2: Study OverviewFigure 2 Study OverviewReviews <strong>of</strong> <strong>the</strong> LiteratureEmpirical Study <strong>in</strong> four <strong>NHS</strong> TrustsCh.4 (Methods)Literature review tosupport <strong>the</strong> <strong>in</strong>vestigation<strong>of</strong> our strategy questions[Ch. 2]Systematic review <strong>of</strong> <strong>the</strong>economic implications<strong>of</strong> large scale <strong>IT</strong>implementation <strong>in</strong> healthcare.[Ch. 3]Qualitative studyLevel 1Stage a} ImplementationStage b} <strong>of</strong> NPfit[Ch. 5]Level 2Process and impact <strong>of</strong>implementation <strong>of</strong> eTOBand PACs[Ch. 6]Quantitative study <strong>of</strong>impact <strong>of</strong> eTOB andPACS[Ch. 7]8
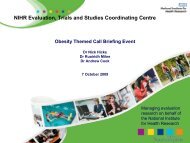
Report to SDO for NCRS ProjectIntroduction1.4. Outl<strong>in</strong>e <strong>of</strong> <strong>the</strong> reportFigure 2 provides an overview <strong>of</strong> <strong>the</strong> study. In chapter 2, <strong>the</strong> literature to supportour study is reviewed. In chapter 3, we report <strong>the</strong> methods and f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> <strong>the</strong>systematic review <strong>of</strong> <strong>the</strong> economic implications <strong>of</strong> large scale <strong>IT</strong> implementation <strong>in</strong>health care. In chapter 4, we describe <strong>the</strong> methods used for <strong>the</strong> qualitative andquantitative empirical elements <strong>of</strong> <strong>the</strong> study. Chapter 5 presents <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> ‘levelone’ <strong>of</strong> <strong>the</strong> qualitative study analys<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> at twodifferent po<strong>in</strong>ts <strong>in</strong> time. In chapter 6, we present f<strong>in</strong>d<strong>in</strong>gs from ‘level 2’ <strong>of</strong> <strong>the</strong>qualitative study on <strong>the</strong> implementation <strong>of</strong> specific <strong>IT</strong> applications. Chapter 7presents f<strong>in</strong>d<strong>in</strong>gs from <strong>the</strong> quantitative study <strong>of</strong> <strong>the</strong> impact <strong>of</strong> <strong>the</strong> implementation <strong>of</strong>PACS and CPOE. F<strong>in</strong>ally, <strong>in</strong> chapter 9, we summarise and discuss our f<strong>in</strong>d<strong>in</strong>gs,suggest implications for policy and practice, and areas for future research.9
Report to SDO for NCRS ProjectIntroductionTable 3: Implementation <strong>of</strong> Patient Adm<strong>in</strong>istration Systems (PAS) dur<strong>in</strong>g <strong>the</strong> project. Unshaded cells represent<strong>the</strong> “before” implementation period, light shaded cells <strong>the</strong> “dur<strong>in</strong>g” period and “dark” rows <strong>the</strong> “after”period.Trust 1 Trust 2 Trust 3 Trust 4Site 1 Site 2 Site 1 Site 2 S<strong>in</strong>gle site S<strong>in</strong>gle site2000 PAS type A No PAS PAS type B PAS type C PAS type D PAS type E200120022003 PAS type F PAS type F PAS type G20042005All sites had a trust-wide PAS <strong>in</strong> 2000 except for Trust 1. Site 2 <strong>of</strong> Trust 1 had a legacy system which did not <strong>in</strong>clude all patients and which did notoperate <strong>in</strong> ‘real-time’.Trusts 2 and 4 implemented new PAS <strong>in</strong> 2003.10
Report to SDO for NCRS ProjectIntroductionTable 4: Implementation <strong>of</strong> Picture Archiv<strong>in</strong>g and Communication Systems (PACS) dur<strong>in</strong>g <strong>the</strong> project.Unshaded cells represent <strong>the</strong> “before” implementation period, light shaded cells <strong>the</strong> “dur<strong>in</strong>g” periodand “dark” rows <strong>the</strong> “after” period.PACS Trust 1 Trust 2 Trust 3 Trust 4Site 1 Site 2 Site 1 Site 2 S<strong>in</strong>gle site S<strong>in</strong>gle site2000 RIS only None PACS type A, partonlyRIS only RIS only RIS only2001 PACS type B, partonlyPACS type C, A&Eand orthopaedics.2002 PACS type C, allo<strong>the</strong>r specialties2003 PACS enhanced, partonly20042005All sites had a radiology <strong>in</strong>formation system (RIS) <strong>in</strong> 2000, i.e. a database for logg<strong>in</strong>g tests ordered/carried out, except for Trust 1. Site 2 <strong>of</strong> Trust1 had no RIS.Trust 2 had a PACS only on part <strong>of</strong> one site. This PACS implementation existed at <strong>the</strong> start <strong>of</strong> <strong>the</strong> study period and rema<strong>in</strong>ed unchangedthroughout, except for an enhancement <strong>in</strong> 2003 to allow web view<strong>in</strong>g. Trust 2 attempted to implement a new system for order<strong>in</strong>g radiology tests <strong>in</strong>2002 but this was not successful and <strong>the</strong> system rema<strong>in</strong>ed predom<strong>in</strong>antly paper-based throughout <strong>the</strong> study.Trust 3 opened a new build<strong>in</strong>g <strong>in</strong> 2001 for paediatrics, with a limited implementation <strong>of</strong> a PACS (less than
Report to SDO for NCRS ProjectIntroductionTable 5: Implementation <strong>of</strong> e-Test Order<strong>in</strong>g and Brows<strong>in</strong>g (CPOE) dur<strong>in</strong>g <strong>the</strong> project. Unshaded cells represent<strong>the</strong> “before” implementation period, light shaded cells <strong>the</strong> “dur<strong>in</strong>g” period and “dark” rows <strong>the</strong> “after”period.Trust 1 Trust 2 Trust 3 Trust 4Site 1 Site 2 Site 1 Site 2 S<strong>in</strong>gle site S<strong>in</strong>gle site2000 LIS only None LIS only LIS only LIS only LIS only2001 CPOE type A New LIS New LIS2002 Roll-out completeexcept maternityCPOE type B(order<strong>in</strong>g) attempted2003 CPOE type B(brows<strong>in</strong>g) attemptedCPOE type B(brows<strong>in</strong>g) attempted20042005All sites had a laboratory <strong>in</strong>formation system (LIS) <strong>in</strong> 2000, i.e. a database for logg<strong>in</strong>g tests ordered/carried out, except for Trust 1. Site 2 <strong>of</strong> Trust1 had no LIS. Trust 1 implemented an e-Test on site 1 <strong>in</strong> 2001. The roll-out <strong>of</strong> this system on site 1 was completed across all specialties exceptmaternity by 2002.Trust 2 implemented <strong>the</strong> LIS component <strong>of</strong> a larger eTest <strong>in</strong> 2001 on both sites. Trust 2 attempted to implement <strong>the</strong> order<strong>in</strong>g component <strong>of</strong> a newe-Test <strong>in</strong> 2002 but this was not successful and <strong>the</strong> system rema<strong>in</strong>ed predom<strong>in</strong>antly paper-based throughout <strong>the</strong> study. Trust 2 implement <strong>the</strong> testbrow<strong>in</strong>g component <strong>of</strong> a new e-Test on both sites <strong>in</strong> 2003 but this was not successful and <strong>the</strong> system rema<strong>in</strong>ed predom<strong>in</strong>antly paper-based.Trusts 3 and 4 had a LIS only throughout <strong>the</strong> study period, although Trust 4 had a facility for communicat<strong>in</strong>g <strong>in</strong>dividual test results to generalpractitioners electronically.12
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literature2. Literature to support <strong>the</strong> <strong>in</strong>vestigation <strong>of</strong> <strong>the</strong> study objectives2.1. Literature search strategiesFor <strong>the</strong> literature review <strong>of</strong> quantitative and qualitative evaluations <strong>of</strong> <strong>IT</strong> systems<strong>in</strong> health care, an <strong>in</strong>itial search was conducted at <strong>the</strong> start <strong>of</strong> project betweenOctober 2003 and March 2004. (The literature review for <strong>the</strong> economic objectivewas conducted separately at a later date; see chapter 3.) After <strong>the</strong> <strong>in</strong>itial review,additional sources <strong>of</strong> <strong>in</strong>formation (from journals, media sources, conferences andexpert contacts) were syn<strong>the</strong>sised <strong>in</strong>to <strong>the</strong> review as <strong>the</strong> study progressed.The review sought to capture evaluations <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> health care and, moreparticularly, electronic patient records and e-test order<strong>in</strong>g and ‘brows<strong>in</strong>g’ <strong>of</strong> testresults (known <strong>in</strong> <strong>the</strong> United States as computerised physician order entry, orCPOE). The <strong>in</strong>itial databases searched were: Medl<strong>in</strong>e, Web <strong>of</strong> Science, Embase,Serfile, Sigle, HMIC, K<strong>in</strong>gs Fund and Ulrichs. MeSH and free text words wereused <strong>in</strong> a variety <strong>of</strong> comb<strong>in</strong>ations (with *).Medl<strong>in</strong>e MeSH terms used were:-• Information Systems• Medical-Informatics-Applications• Medical-Records• Qualitative• Knowledge• Attitudes• PracticeFree text words used were:-• Electronic patient records• Computerised patient records• Electronic health records• Computerised physician order entry• Patient adm<strong>in</strong>istration system• Master patient <strong>in</strong>dex• Integrated care record system13
Report to SDO for NCRS ProjectSupport<strong>in</strong>g LiteratureSpecific qualitative literature search terms used were:• Ethnography• Phenomenology• Grounded <strong>the</strong>ory• Discourse analysis• focus group• hermeneutic• narrative analysis or narrative psychology or narrative method• human science• new paradigm• action research• co-operative <strong>in</strong>quiry• humanistic• existential• experiential &• conversation analysisThe search also <strong>in</strong>cluded check<strong>in</strong>g references <strong>in</strong> references lists <strong>of</strong> papersalready identified, identify<strong>in</strong>g ma<strong>in</strong> researchers <strong>in</strong> <strong>the</strong> field and search<strong>in</strong>g underauthor names, and search<strong>in</strong>g general <strong>in</strong>ternet sites (Google). The articlesretrieved <strong>in</strong>cluded 380 MEDLINE abstracts and 325 Web <strong>of</strong> Knowledge abstracts.The results <strong>of</strong> this <strong>in</strong>itial search and subsequent additional sources <strong>of</strong> <strong>in</strong>formationare syn<strong>the</strong>sised below.2.2. Difficulties <strong>in</strong> evaluat<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> EPRsThere is considerable evidence that <strong>the</strong> implementation <strong>of</strong> large-scale healthservice <strong>IT</strong> projects is extremely difficult to achieve. 9 The problem <strong>of</strong> achiev<strong>in</strong>g<strong>in</strong>teroperability, <strong>the</strong> cornerstone <strong>of</strong> any <strong>in</strong>tegrated record system, still appearselusive. Hospitals <strong>of</strong>ten have small ‘own brand’ <strong>IT</strong> systems that will not l<strong>in</strong>k towider networks. The issue <strong>of</strong> confidentiality and security is ano<strong>the</strong>r <strong>IT</strong> problem <strong>in</strong>hospital medic<strong>in</strong>e that has not been completely resolved 10 . These factors,amongst o<strong>the</strong>rs, have led to <strong>IT</strong> implementation failure rates <strong>of</strong> around 30%,although this may be higher; many negative results are likely to be seen as14
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literaturepolitically unacceptable and do not become public. 11,12This said, examples <strong>of</strong> UK<strong>IT</strong> ‘disasters’, such as <strong>the</strong> Wessex Regional Health Authority <strong>in</strong>itiative end<strong>in</strong>g <strong>in</strong>losses to <strong>the</strong> taxpayer <strong>of</strong> £43M, 6 and <strong>the</strong> failed Computer Aided Dispatch ServiceSystem for <strong>the</strong> London Ambulance Service, 13 are not hard to uncover. Managersat <strong>the</strong> Ed<strong>in</strong>burgh Royal Infirmary, Scotland’s flagship hospital, were subject to apolitical <strong>in</strong>quiry, with questions raised <strong>in</strong> <strong>the</strong> new Scottish Parliament about <strong>the</strong>cost <strong>of</strong> <strong>the</strong> £30m McKesson system that was scheduled to be runn<strong>in</strong>g <strong>in</strong> April2002, and was never put <strong>in</strong> place. 14 In understand<strong>in</strong>g why <strong>the</strong> <strong>in</strong>troduction <strong>of</strong>EPRs <strong>in</strong> UK Hospitals has proved to be so difficult, and identify<strong>in</strong>g how potentialobstacles might be removed, evidence is scarce. 15remarkably rare. 12Analysis <strong>of</strong> <strong>IT</strong> failure isResults from economic analyses and randomised controlled trials <strong>of</strong> ‘successful’<strong>IT</strong> developments are limited, <strong>in</strong> that <strong>the</strong>y cover a fraction <strong>of</strong> <strong>the</strong> total number <strong>of</strong>health care applications developed, and address a limited number <strong>of</strong> questions. 16Two recent systematic reviews assessed <strong>the</strong> impact <strong>of</strong> health care <strong>IT</strong> <strong>in</strong> general,and <strong>the</strong> impact <strong>of</strong> pathology test order<strong>in</strong>g systems <strong>in</strong> particular. 17,18Both reviewsconcluded that, although <strong>the</strong> potential benefits <strong>of</strong> <strong>IT</strong> <strong>in</strong> health care rema<strong>in</strong> clear,fur<strong>the</strong>r research <strong>in</strong>to actual ga<strong>in</strong>s is urgently needed.Our research should <strong>in</strong>form those responsible for allocat<strong>in</strong>g <strong>of</strong>ten scarce funds to<strong>IT</strong> systems procurement, and should help to create realistic expectations about<strong>the</strong> benefits <strong>of</strong> <strong>the</strong>se systems, but EPRs are not likely to be a magic bullet. It maytake many years <strong>of</strong> heavy <strong>in</strong>vestment before any patient benefits or f<strong>in</strong>ancialsav<strong>in</strong>gs are visible enough to be evaluated. 19Equally, <strong>IT</strong> can only improvecl<strong>in</strong>ical practice <strong>in</strong> areas where lack <strong>of</strong> data or poor <strong>in</strong>formation process<strong>in</strong>g is <strong>the</strong>ma<strong>in</strong> problem. It cannot magically solve issues <strong>of</strong> a lack <strong>of</strong> staff or lack <strong>of</strong>capacity. 20Even if quantifiable benefits are demonstrable, this is only half <strong>the</strong>story. Economic accountability does not mean that end-users accept <strong>the</strong> system,or maximise <strong>the</strong> potential <strong>of</strong> <strong>the</strong> system <strong>in</strong> <strong>the</strong>ir work<strong>in</strong>g lives. 11,21<strong>IT</strong> systems acquisition is not solely a technical and economic choice, nor is it aquestion <strong>of</strong> staff persuasion and acquiescence. Even if hospital doctors were<strong>of</strong>fered f<strong>in</strong>ancial or pr<strong>of</strong>essional <strong>in</strong>centives to use computer technology, as hasbeen <strong>the</strong> case for GPs, <strong>the</strong> unique complexities <strong>of</strong> work<strong>in</strong>g <strong>in</strong> hospital medic<strong>in</strong>epresents huge challenges. 22Medical work is characterised by deep15
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literatureunpredictability that pre-empts <strong>the</strong> k<strong>in</strong>d <strong>of</strong> standardisation and automation found<strong>in</strong> o<strong>the</strong>r bureaucracies and <strong>in</strong>dustries. 23Hospital medic<strong>in</strong>e has complexworkflows, job specialisation and a division <strong>of</strong> labour that creates knowledge<strong>in</strong>tensiveand diverse patterns <strong>of</strong> <strong>in</strong>formation use and record keep<strong>in</strong>g. Yet, if <strong>IT</strong> isgo<strong>in</strong>g to support <strong>the</strong> ‘core bus<strong>in</strong>ess process’ <strong>of</strong> health, record keep<strong>in</strong>g rout<strong>in</strong>esmust be standardised <strong>in</strong> <strong>the</strong> first <strong>in</strong>stance. 23The difficulty <strong>of</strong> understand<strong>in</strong>g and manag<strong>in</strong>g this organisational complexity,whilst implement<strong>in</strong>g new levels <strong>of</strong> standardisation, is apparent when exam<strong>in</strong><strong>in</strong>g<strong>the</strong> spectacular <strong>IT</strong> failure that occurred <strong>in</strong> <strong>the</strong> public health system <strong>of</strong> New SouthWales (NSW), Australia. 9The essence <strong>of</strong> this case study concerns <strong>the</strong> mismatchbetween <strong>the</strong> facilities provided, i.e. <strong>the</strong> new <strong>IT</strong> system, and <strong>the</strong> social organisationit was supposed to support. 12In 1996, <strong>the</strong> NSW health care system embarked onan <strong>IT</strong> strategy to achieve better resource management. (The NSW health caresystem is large by world standards.) After a rigorous selection procedure, aPAS/cl<strong>in</strong>ical system was chosen that had been successfully implemented <strong>in</strong> over100 sites <strong>in</strong> <strong>the</strong> US, and a few sites across Europe. Despite careful systemselection, after a period <strong>of</strong> <strong>in</strong>creas<strong>in</strong>g staff dissent and protest, <strong>the</strong> system had tobe withdrawn. Losses were substantial and took several forms, <strong>in</strong>clud<strong>in</strong>gconsiderable f<strong>in</strong>ancial losses, <strong>the</strong> considerable distrust generated, and delays <strong>in</strong>future strategic plann<strong>in</strong>g. To uncover what went wrong, a research team<strong>in</strong>terviewed a total <strong>of</strong> 64 people across five implementation sites. Factors that ledto <strong>the</strong> failure were identified as organisational, cultural and technical. The systemdid not meet staff expectations <strong>in</strong> terms <strong>of</strong> ease <strong>of</strong> use, flexibility and <strong>the</strong> range <strong>of</strong>services <strong>of</strong>fered, with staff roles and expectations be<strong>in</strong>g very different <strong>in</strong> NSWthan <strong>in</strong> <strong>the</strong> US. In sites that had a more developed <strong>IT</strong> <strong>in</strong>frastructure, manycl<strong>in</strong>icians found that <strong>the</strong>y were actually los<strong>in</strong>g important functionality. This factorgenerated considerable discontent. In addition, <strong>the</strong> programme was so novel thatnearly all <strong>the</strong> key decision-makers were well outside <strong>the</strong>ir area <strong>of</strong> expertise. 122.3. Organisational research exam<strong>in</strong><strong>in</strong>g EPR implementationIn attempt<strong>in</strong>g to unpack how <strong>IT</strong> can be successfully implemented, <strong>the</strong> scientificliterature spans a diverse range <strong>of</strong> discipl<strong>in</strong>es and journals and covers a hugebreadth <strong>of</strong> issues. 13 Yet despite this wide <strong>in</strong>terest, very little evidence on <strong>the</strong>16
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literatureimpact <strong>of</strong> EPRs is available. A review <strong>of</strong> 1832 papers on EPR implementation byMoorman and van der Lei 24 found no obvious trends regard<strong>in</strong>g impact, except an<strong>in</strong>creased <strong>in</strong>terest <strong>in</strong> confidentiality. The field <strong>of</strong> <strong>in</strong>quiry is so scattered anddiverse, with different stakeholders both conduct<strong>in</strong>g and commission<strong>in</strong>g research,that little <strong>in</strong> <strong>the</strong> way <strong>of</strong> a coherent message emerges. A diverse range <strong>of</strong>methodologies have been used, with a lack <strong>of</strong> <strong>the</strong>oretical focus, and experts havebeen largely divided on what states are necessary for implementation success. 7Even more surpris<strong>in</strong>gly, <strong>in</strong> <strong>the</strong> review conducted by Moorman & van der Lei, none<strong>of</strong> <strong>the</strong> 1832 papers reviewed actually <strong>in</strong>volved an implementation <strong>of</strong> an EPR itself.A small coherent body <strong>of</strong> work focuses on understand<strong>in</strong>g <strong>the</strong> sociological process<strong>of</strong> implement<strong>in</strong>g EPRs, <strong>in</strong> small groups <strong>of</strong> health care workers. 25For example,vary<strong>in</strong>g resistance to us<strong>in</strong>g computerised care systems was <strong>in</strong>vestigatedqualitatively by Timmons. 26Twenty eight nurses and 3 project managers were<strong>in</strong>terviewed across three UK District General Hospitals. The researcher foundthat refusal to engage with <strong>the</strong> systems was best understood <strong>in</strong> terms <strong>of</strong> nurs<strong>in</strong>gculture, with non-compliance expressed <strong>in</strong> largely passive ways. Postponementra<strong>the</strong>r than outright refusal was used to negotiate nurses’ work patterns. Ano<strong>the</strong>rstudy used observational methods, study<strong>in</strong>g 8 doctors and 2 nurses, to identifypatterns <strong>of</strong> hospital <strong>IT</strong> communication. 27The authors concluded thatcommunication technology was most favoured by <strong>the</strong> medical staff when itactively <strong>in</strong>terrupted <strong>the</strong>ir work, with a preference for <strong>in</strong>formation that encourageddelivery via face-to-face communication. In an ethnographic study <strong>of</strong> <strong>the</strong> use <strong>of</strong>pre-operative risk-assessment forms, <strong>the</strong> researchers demonstrated how <strong>the</strong>practical use <strong>of</strong> documents by medical pr<strong>of</strong>essionals can be fundamentally atodds with how <strong>the</strong> organisation at large wants <strong>the</strong>m used. 28studies are extremely <strong>in</strong>formative <strong>in</strong> <strong>the</strong> local context <strong>in</strong> which <strong>the</strong>y areThese types <strong>of</strong> microundertaken and <strong>in</strong>crease our understand<strong>in</strong>g <strong>of</strong> how a small group <strong>of</strong> healthworkers react to, and shape <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>g a specific <strong>IT</strong> <strong>in</strong>novation.However, this micro level research is less applicable when attempt<strong>in</strong>g tounderstand <strong>the</strong> multiple processes <strong>in</strong>volved <strong>in</strong> large-scale implementation <strong>of</strong>EPRs, both with<strong>in</strong> and across a number <strong>of</strong> acute trusts.Research that addresses more macro levels <strong>of</strong> implementation <strong>of</strong> <strong>IT</strong> systems <strong>in</strong>health care is scarce, with most studies <strong>in</strong> medical care sett<strong>in</strong>gs tend<strong>in</strong>g to <strong>in</strong>volve17
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literaturesmall piecemeal development. Presumably, practical reasons <strong>of</strong> cost anddisruption prevent larger scale projects occurr<strong>in</strong>g. Larger studies are mostly <strong>of</strong>North American or Australasian orig<strong>in</strong> and focus on ‘users’ experiences. 29Currently, <strong>the</strong> only large study <strong>of</strong> EPR implementation is <strong>the</strong> deployment <strong>of</strong> 22Veterans Integrated Services Networks (VISNs) <strong>in</strong> <strong>the</strong> US department <strong>of</strong> VeteransAffairs (VA). 30The implementation programme <strong>in</strong>volved <strong>the</strong> adoption <strong>of</strong> anational computerized patient record system (CPRS) <strong>in</strong> 173 VA hospitals.F<strong>in</strong>d<strong>in</strong>gs from research <strong>in</strong>to <strong>the</strong> programme highlight ‘success’ factors such as ahav<strong>in</strong>g a strongly supportive team, user empowerment, and system flexibility.Researchers also emphasise <strong>the</strong> need to <strong>in</strong>corporate users’ specialist needs <strong>in</strong>toany s<strong>of</strong>tware development. 31Ano<strong>the</strong>r relatively large study was conducted <strong>in</strong> five community hospitals <strong>in</strong> BritishColumbia, Canada, 7 exam<strong>in</strong><strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> a patient care <strong>in</strong>formationsystem (PCIS) from <strong>the</strong> perspective <strong>of</strong> health care pr<strong>of</strong>essionals. The researcherconducted 85 <strong>in</strong>terviews across a range <strong>of</strong> staff. The study highlights <strong>the</strong>complexity <strong>of</strong> implement<strong>in</strong>g <strong>IT</strong> <strong>in</strong>novations, with many unexpected consequencesoccurr<strong>in</strong>g and many expected benefits not be<strong>in</strong>g realised. It was anticipated that<strong>in</strong>creased productivity would free up time but, <strong>in</strong> reality, any excess time was redirectedto new work programs and activities. This contributed to decreased jobsatisfaction. Workload and turnaround time for process<strong>in</strong>g medical orders also<strong>in</strong>creased, due to <strong>the</strong> additional <strong>in</strong>formation required; this was described by <strong>the</strong>authors as a “productivity paradox”. Overall, role changes and a number <strong>of</strong> o<strong>the</strong>rpractical problems meant that <strong>the</strong> implementation was far from ‘successful’.2.4. Organisational research exam<strong>in</strong><strong>in</strong>g CPOE implementationOne <strong>of</strong> our study aims was to explore how <strong>in</strong>novative pathology and radiologysystems, proposed by Connect<strong>in</strong>g for Health, are experienced by <strong>NHS</strong> staff, andto describe any impact on work<strong>in</strong>g practices. A body <strong>of</strong> work closely aligned to<strong>the</strong>se aims has been conducted <strong>in</strong> <strong>the</strong> United States by Joan Ash and her team.Ash studied CPOE extensively across three large health care sites (University <strong>of</strong>Virg<strong>in</strong>ia, The VA Puget Sound campuses encompass<strong>in</strong>g five hospitals, and <strong>the</strong> ElCam<strong>in</strong>o Hospital site). CPOE allows a cl<strong>in</strong>ician to sit at a computer and directlyenter care orders or browse test results. Observations, oral histories, focus18
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literaturegroups and <strong>in</strong>terviews enabled a comprehensive picture <strong>of</strong> a diverse range <strong>of</strong>‘users’ experiences to emerge. F<strong>in</strong>d<strong>in</strong>gs from <strong>the</strong> team’s <strong>in</strong>itial studies 32 outl<strong>in</strong>edunexpected problems. Initial <strong>in</strong>troduction <strong>of</strong> CPOE led to an <strong>in</strong>crease, not adecrease, <strong>in</strong> <strong>the</strong> amount <strong>of</strong> paper generated, with staff hav<strong>in</strong>g a sense that CPOE<strong>in</strong>terrupted <strong>the</strong>ir workflow and decreased decision-mak<strong>in</strong>g and educationalopportunities. 32Implementation also caused a disruption <strong>in</strong> <strong>the</strong> balance <strong>of</strong> powerwith<strong>in</strong> <strong>the</strong> organisations, with users <strong>of</strong>ten feel<strong>in</strong>g <strong>the</strong> organisation ga<strong>in</strong>ed morethan <strong>the</strong>y did. 33In addition, a separate study conducted on <strong>the</strong> same hospitalsites 34 found that CPOE had an adverse impact on team relationships, with teamspirit and cohesion underm<strong>in</strong>ed.Apart from uncover<strong>in</strong>g <strong>the</strong>se number <strong>of</strong> unexpected and unwanted disadvantagesto implementation, <strong>the</strong> researchers also found that qualitative evaluation <strong>of</strong> CPOEled to a complex array <strong>of</strong> methodological problems. 33First, when <strong>in</strong>terview<strong>in</strong>gstaff, <strong>the</strong> researchers found it was difficult, and <strong>of</strong>ten impractical, to isolate CPOEimplementation from o<strong>the</strong>r work processes. Secondly, <strong>the</strong> researchers found itcould not be assumed that people were always talk<strong>in</strong>g about <strong>the</strong> same th<strong>in</strong>g,even when <strong>the</strong>y used <strong>the</strong> same words, with existential differences <strong>in</strong> perceptionsand mean<strong>in</strong>gs. Lastly, <strong>the</strong> researchers found <strong>the</strong>re was <strong>of</strong>ten a lack <strong>of</strong>consistency between what <strong>the</strong>y observed and what <strong>the</strong>y were be<strong>in</strong>g told, mak<strong>in</strong>gfirm conclusions difficult.Despite <strong>the</strong>se problems, later work by <strong>the</strong> group 35 reported recommendations forsuccessful CPOE implementation based on four major <strong>the</strong>mes. The first <strong>the</strong>meconcerns organisational issues, and <strong>in</strong>dicates that a strong organisational culture<strong>of</strong> trust, collaboration and teamwork, comb<strong>in</strong>ed with supportive leadership, leadsto success. The second <strong>the</strong>me concerns cl<strong>in</strong>ical issues, and emphasises <strong>the</strong> role<strong>of</strong> system customisation and flexibility. A third <strong>the</strong>me, technical issues, cites <strong>the</strong>need for system speed. The last <strong>the</strong>me concerns <strong>the</strong> organisation <strong>of</strong> <strong>in</strong>formation,with people want<strong>in</strong>g <strong>in</strong>formation to be organised <strong>in</strong> a manner that mimics <strong>the</strong>irown th<strong>in</strong>k<strong>in</strong>g. People did not want to be forced to ‘th<strong>in</strong>k like a computer’. Fur<strong>the</strong>rresearch <strong>in</strong>to successful CPOE implementation at Ohio State University HealthSystem served to re<strong>in</strong>force <strong>the</strong>se conclusions. Similar factors emerged; <strong>the</strong> needfor a user-friendly <strong>in</strong>terface, senior management support, physician efficacy,regard<strong>in</strong>g <strong>the</strong> perceived ability to use <strong>the</strong> systems, and effective teamwork. In19
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literatureaddition, <strong>the</strong> researchers <strong>in</strong> Ohio suggested that <strong>the</strong> elim<strong>in</strong>ation <strong>of</strong> alternativemethods <strong>of</strong> order<strong>in</strong>g, and <strong>the</strong> abolition <strong>of</strong> all paper forms is useful; cl<strong>in</strong>icianscannot revert to manual order<strong>in</strong>g if it is not available. 36The f<strong>in</strong>d<strong>in</strong>gs from this body <strong>of</strong> work are generalisable to our study, whenevaluat<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> EPR implementation <strong>in</strong> <strong>the</strong> <strong>NHS</strong>, <strong>in</strong> highlight<strong>in</strong>g potentialprecursors for success and suggest<strong>in</strong>g potential obstacles. However, asdiscussed earlier <strong>in</strong> relation to <strong>the</strong> New South Wales study, it would be a mistaketo assume that <strong>the</strong>se factors will automatically translate to a different context.There are important differences between North American health care systemsand England’s current <strong>NHS</strong> EPR strategy. Some <strong>of</strong> <strong>the</strong>se differences are aquestion <strong>of</strong> organisational configuration, such as private and public sector f<strong>in</strong>anceand cost allocation, and <strong>the</strong> more rigid demarcation <strong>of</strong> clerical and cl<strong>in</strong>ical roles <strong>in</strong><strong>the</strong> US and Canada. 9organisational structure and strategy. 37O<strong>the</strong>r differences concern fundamental transformations <strong>in</strong>The CPOE studies <strong>in</strong>volve implement<strong>in</strong>ga s<strong>in</strong>gle form <strong>of</strong> electronic function across 7 or 8 hospitals. The NPf<strong>IT</strong> is likely toimpact on, and transform, every part <strong>of</strong> England’s current health care system.The research reviewed tends to ignore wider issues <strong>of</strong> organisational andtransformational change, preferr<strong>in</strong>g to concentrate on <strong>the</strong> utility <strong>of</strong> <strong>the</strong> <strong>in</strong>novationto <strong>the</strong> <strong>in</strong>dividual consumer. Research address<strong>in</strong>g <strong>in</strong>novation on <strong>the</strong> scale <strong>of</strong> <strong>the</strong>current NPf<strong>IT</strong> is simply not available anywhere because <strong>the</strong> national program is<strong>the</strong> largest and most ambitious public sector <strong>IT</strong> project ever undertaken. Noth<strong>in</strong>gon this scale has been attempted before. 102.5. Research exam<strong>in</strong><strong>in</strong>g implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong>Current research specifically concerned with <strong>the</strong> evaluation <strong>of</strong> implementation <strong>of</strong>EPRs and <strong>IT</strong> <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong> is limited. A review <strong>of</strong> this literature undertaken <strong>in</strong>1999 generated over 2000 citations, yet few <strong>in</strong>stances <strong>of</strong> <strong>in</strong>dependent externalevaluations were identified, with comparative quantitative studies virtuallyunknown. 38 The authors concluded that few reports gave a full account <strong>of</strong> <strong>the</strong>costs <strong>in</strong>volved, and that many evaluations were ‘simplistic, <strong>in</strong>adequate orprecipitate’. The messages that emerge are aga<strong>in</strong> general; most problems relateto human ra<strong>the</strong>r than technical factors, work processes must adapt as <strong>IT</strong> is<strong>in</strong>troduced, realistic expectations and timescales should allow for greater benefit20
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literaturerealisation, users should be <strong>in</strong>volved, and that flexibility and communicationcapabilities are key technical requirements. These messages, although useful,may not prove decisive. Many <strong>of</strong> <strong>the</strong> factors outl<strong>in</strong>ed could apply equally well <strong>in</strong>any organisation, and may not be prescriptive enough to address specificchallenges attached to <strong>the</strong> NPf<strong>IT</strong>.In 2003, <strong>the</strong> <strong>NHS</strong> Information Authority commissioned a large scale EPR pilotstudy <strong>in</strong> 16 <strong>NHS</strong> sites across England (ERDIP project), 39 perhaps <strong>in</strong> recognitionthat <strong>the</strong> implementation <strong>of</strong> widespread EPRs <strong>in</strong> <strong>the</strong> <strong>NHS</strong> might be challeng<strong>in</strong>g.The aim <strong>of</strong> <strong>the</strong> pilot study was to learn valuable lessons for <strong>the</strong> ma<strong>in</strong> EPR drivecommenc<strong>in</strong>g <strong>in</strong> 2004. Unfortunately, <strong>the</strong> qualitative and quantitative rigour <strong>of</strong> <strong>the</strong>evaluation is questionable, appear<strong>in</strong>g to yield little apart from <strong>the</strong> most basicanecdotal evidence. As <strong>the</strong> f<strong>in</strong>al report comments, without a targeted set <strong>of</strong>benefits, it is difficult to judge if an <strong>IT</strong> <strong>in</strong>itiative has been successful: “quantification<strong>of</strong> benefits by <strong>the</strong> ERDIP sites has been disappo<strong>in</strong>t<strong>in</strong>gly limited result<strong>in</strong>g <strong>in</strong> littleconcrete evidence.”A more systematic approach to EPR evaluation is available from The BayswaterInstitute, which for three years was part <strong>of</strong> a commissioned programme evaluat<strong>in</strong>gelectronic patient records and <strong>the</strong> <strong>in</strong>tegrated cl<strong>in</strong>ical workstation <strong>in</strong> five UKhospitals. 40The team aimed to capture <strong>the</strong> experience <strong>of</strong> liv<strong>in</strong>g and work<strong>in</strong>g at<strong>the</strong> implementation sites. They reported that, after EPR implementation, manystaff tasks had become easier. However, staff also found that mak<strong>in</strong>g adepartment or function more effective generated more work, and more paper. Forexample, when <strong>the</strong> EPR system for path lab orders went live, requests went up.In response to this <strong>in</strong>crease <strong>in</strong> work load, <strong>the</strong> pathology lab ‘defended itself’ bymak<strong>in</strong>g test order<strong>in</strong>g more difficult aga<strong>in</strong>. Staff also found that <strong>the</strong> formality <strong>of</strong>computer records made it difficult to express uncerta<strong>in</strong> responses such as an<strong>in</strong>struction to ‘keep an eye on him’. Much <strong>of</strong> <strong>the</strong> <strong>in</strong>formation used by staff was<strong>in</strong>complete and <strong>in</strong>formal, and paper seemed better suited for <strong>the</strong>se more openendedand nebulous massages. 41A project on <strong>the</strong> use <strong>of</strong> EPRs <strong>in</strong> UK maternity services has also found that paperrecords are valued, with current EPRs seen by staff as too rigid and <strong>in</strong>flexible. 42In this study, at least half <strong>of</strong> <strong>the</strong> respondents questioned had problems access<strong>in</strong>g<strong>the</strong> k<strong>in</strong>d <strong>of</strong> <strong>in</strong>formation <strong>the</strong>y needed to support patient care. Paper records have21
Report to SDO for NCRS ProjectSupport<strong>in</strong>g Literaturewhat Kle<strong>in</strong> has co<strong>in</strong>ed <strong>the</strong> ‘Mart<strong>in</strong>i factor’; once found <strong>the</strong>y can be used any time,any place, anywhere. 40,41This potential advantage <strong>of</strong> paper records may be onereason why <strong>the</strong> authors concluded that, although EPRs were <strong>in</strong> certa<strong>in</strong> casesbeneficial, on balance time saved versus time spent was at best equal. Theauthors propose that future EPR systems will have to do considerably better <strong>in</strong>recognis<strong>in</strong>g and balanc<strong>in</strong>g <strong>the</strong> potential conflicts between time saved and timespent. They also warn that current euphoric claims regard<strong>in</strong>g <strong>the</strong> effectiveness <strong>of</strong>EPRs are likely to result <strong>in</strong> widespread disappo<strong>in</strong>tment amongst <strong>NHS</strong> staff andpatients. 42Whe<strong>the</strong>r this prediction will be realised when implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> iscompleted is unknown. A report by <strong>the</strong> Institute for Public Policy Research 43described how <strong>the</strong> benefits <strong>of</strong> EPRs to health services could be huge, but <strong>the</strong>risks could also be substantial, because <strong>of</strong> <strong>the</strong> failure to provide evidence <strong>of</strong>impact. The research, based on exam<strong>in</strong><strong>in</strong>g large EPR pilots <strong>in</strong> <strong>the</strong> <strong>NHS</strong>,concluded that public and political support for unprecedented spend<strong>in</strong>g on <strong>IT</strong><strong>in</strong>vestment <strong>in</strong> health services will not be realised without better plann<strong>in</strong>g andevaluation. Trials <strong>of</strong> electronic patient records failed to demonstrate that <strong>the</strong>ywould lead to more flexible services, cost sav<strong>in</strong>gs or improvements <strong>in</strong> treatment <strong>of</strong>patients. In addition, pilots <strong>of</strong> electronic appo<strong>in</strong>tment book<strong>in</strong>g systems failed toshow clearly that <strong>the</strong>y helped to facilitate greater choice for patients about where,when and by whom <strong>the</strong>y are treated. A more recent National Audit Office reportalso raised concerns, with <strong>the</strong> current roll out <strong>of</strong> NPf<strong>IT</strong> reported as less thanoptimal. 44The report highlighted that <strong>the</strong> programme faced significant challenges<strong>in</strong> deliver<strong>in</strong>g systems to agreed timescales, ensur<strong>in</strong>g <strong>in</strong>volvement <strong>of</strong> <strong>NHS</strong>organisations <strong>in</strong> implementation and, importantly, ga<strong>in</strong><strong>in</strong>g <strong>the</strong> support <strong>of</strong> <strong>NHS</strong> staffand <strong>the</strong> public.2.6. ConclusionsOne aim <strong>of</strong> this study is to determ<strong>in</strong>e which organisational factors impact on <strong>the</strong>implementation <strong>of</strong> electronic patient records <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong>. Current researchreviewed <strong>of</strong>fers some useful <strong>in</strong>sights, <strong>in</strong> suggest<strong>in</strong>g that factors such as hav<strong>in</strong>g anorganisational culture <strong>of</strong> trust, plus good teamwork, supportive leadership, systemcustomisation, flexibility, userability and speed, will aid success. However, as22
Report to SDO for NCRS ProjectSupport<strong>in</strong>g LiteratureBerg po<strong>in</strong>ts out, ‘what a successful implementation is can only be discovered <strong>in</strong><strong>the</strong> very process <strong>of</strong> do<strong>in</strong>g <strong>the</strong> implementation’. 45Success is determ<strong>in</strong>ed by, andreliant on, so many dimensions that no simple formula will work for every case.There is no ‘recipe’ that guarantees success. In order to develop a detailedaccount <strong>of</strong> <strong>the</strong> processes underly<strong>in</strong>g EPR implementation with<strong>in</strong> our study sites,we drew on both <strong>the</strong> current organisational literature and <strong>the</strong>mes which emergedfrom our data.23
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3. Systematic review <strong>of</strong> <strong>the</strong> economic implications <strong>of</strong> large scale <strong>IT</strong>implementation <strong>in</strong> health care3.1. IntroductionThe scarcity <strong>of</strong> available health care resources means that <strong>the</strong>y need to beallocated so that <strong>the</strong>y generate <strong>the</strong> maximum possible health benefit. The goal <strong>of</strong>economic evaluation is to provide a comprehensive assessment <strong>of</strong> potential costsand benefits to provide <strong>the</strong> necessary support <strong>in</strong> this decision mak<strong>in</strong>g process.Drummond et al. def<strong>in</strong>e economic evaluation as “<strong>the</strong> comparative analysis <strong>of</strong>alternative courses <strong>of</strong> action <strong>in</strong> terms <strong>of</strong> both costs and consequences”. 46 Acomprehensive economic evaluation should conta<strong>in</strong> a number <strong>of</strong> key elements.These <strong>in</strong>clude <strong>the</strong> identification, measurement, valuation and comparison <strong>of</strong> allrelevant costs and consequences relat<strong>in</strong>g to <strong>the</strong> alternative technologies underconsideration. A competent economic evaluation will also assess <strong>the</strong> level <strong>of</strong>uncerta<strong>in</strong>ty surround<strong>in</strong>g <strong>the</strong>se results so that <strong>the</strong> decision-maker can assess <strong>the</strong>robustness <strong>of</strong> <strong>the</strong> results with respect to alternative assumptions. 47In <strong>the</strong>ory, all health care technologies should be subject to economic analysis.However, <strong>the</strong> need for robust and comprehensive economic evaluations becomeseven greater when <strong>the</strong> implementation <strong>of</strong> particularly costly technologies is be<strong>in</strong>gdebated. The current National Programme for <strong>IT</strong> (NPf<strong>IT</strong>) for <strong>the</strong> <strong>NHS</strong>, with anestimated <strong>in</strong>vestment outlay <strong>of</strong> £6.2 billion over ten years, certa<strong>in</strong>ly satisfies thiscriterion. 483.2. Background <strong>in</strong>formation on <strong>IT</strong> implementationThe economic implications <strong>of</strong> <strong>the</strong> <strong>in</strong>tegration <strong>of</strong> <strong>in</strong>formation technology (<strong>IT</strong>) <strong>in</strong>tohealth care and its consequences have been studied widely. Although <strong>the</strong>amount <strong>of</strong> literature on this subject is vast, it is difficult to f<strong>in</strong>d a consensus amongresearchers on <strong>the</strong> methods <strong>of</strong> evaluation and <strong>the</strong> effects <strong>of</strong> <strong>the</strong> implementedtechnology.The majority <strong>of</strong> <strong>the</strong> studies <strong>in</strong> this review compared <strong>the</strong> impact <strong>of</strong> an <strong>IT</strong><strong>in</strong>tervention, by study<strong>in</strong>g various outcome measures (e.g. costs, time saved,change <strong>in</strong> productivity) before and after <strong>in</strong>troduction <strong>of</strong> <strong>the</strong> <strong>in</strong>tervention. A small24
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implicationsnumber <strong>of</strong> studies 49-52 used f<strong>in</strong>ancial methods <strong>of</strong> evaluation, such as return on<strong>in</strong>vestment and net present value, both <strong>of</strong> which are a standard method forf<strong>in</strong>ancial evaluation <strong>of</strong> long-term projects. As with <strong>the</strong> methods <strong>of</strong> evaluation, <strong>the</strong>types <strong>of</strong> <strong>IT</strong> <strong>in</strong>terventions evaluated <strong>in</strong> <strong>the</strong> exist<strong>in</strong>g literature varied. We chose t<strong>of</strong>ocus on three broad categories; PACS, electronic medical/patient records (EMR)and CPOE. PACS refers to computers or networks dedicated to <strong>the</strong> storage,retrieval, distribution and presentation <strong>of</strong> images. EMR refers to several differenttypes <strong>of</strong> electronic health records.Considerable confusion still exists <strong>in</strong> <strong>the</strong>literature with respect to <strong>the</strong> scope <strong>of</strong> electronic record systems designated bydifferent terms, e.g. electronic medical or patient record. CPOE is “… <strong>the</strong> element<strong>of</strong> a cl<strong>in</strong>ical <strong>in</strong>formation system that enables a patient’s care provider to enter anorder for a medication, cl<strong>in</strong>ical laboratory or radiology test, or procedure directly<strong>in</strong>to <strong>the</strong> computer and ‘browse’ <strong>the</strong> results <strong>of</strong> <strong>in</strong>vestigations”.The dispersion <strong>in</strong> evaluation methods, paired with clear heterogeneity <strong>of</strong> <strong>the</strong><strong>in</strong>tervention types, creates difficulties <strong>in</strong> assess<strong>in</strong>g and draw<strong>in</strong>g conclusionsbased on <strong>the</strong> reported f<strong>in</strong>d<strong>in</strong>gs. While some researchers acknowledged <strong>the</strong>sedifficulties 53 , <strong>the</strong>y also recognised <strong>the</strong> potential for substantial improvements <strong>in</strong><strong>the</strong> quality <strong>of</strong> health care associated with <strong>the</strong> <strong>in</strong>troduction <strong>of</strong> a new <strong>IT</strong> system andpotential cost-sav<strong>in</strong>gs. 17,48The aim <strong>of</strong> this study was to conduct a systematic review <strong>of</strong> <strong>the</strong> literature on <strong>the</strong>economic implications <strong>of</strong> large scale <strong>IT</strong> implementation <strong>in</strong> a hospital or crossdepartmentalsett<strong>in</strong>g.3.3. MethodsThe focus <strong>of</strong> this review was on economic evaluations and cost analyses <strong>of</strong> largescale <strong>IT</strong> implementations <strong>in</strong> a hospital, or cross-departmental sett<strong>in</strong>gs <strong>in</strong> a number<strong>of</strong> hospitals. The methods and f<strong>in</strong>d<strong>in</strong>gs reported <strong>in</strong> such studies are most likely tobe relevant to <strong>the</strong> NPf<strong>IT</strong>. Therefore, we were not <strong>in</strong>terested <strong>in</strong> studies thatreviewed <strong>the</strong> effects <strong>of</strong> technologies such as telemedic<strong>in</strong>e, cl<strong>in</strong>ical decisionsupport <strong>in</strong>terventions, <strong>in</strong>ternet advice-based <strong>in</strong>terventions, or those that wereimplemented on a small scale, such as with<strong>in</strong> a s<strong>in</strong>gle department or generalpractice. The decision was also made only to review studies that conta<strong>in</strong>ed at25
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implicationsleast some primary data analysis, and which compared two or more <strong>IT</strong> systems orone sett<strong>in</strong>g before and after <strong>in</strong>troduction <strong>of</strong> an <strong>IT</strong> system.Due to <strong>the</strong> rapidchanges <strong>in</strong> <strong>IT</strong>, it was agreed that studies published <strong>in</strong> <strong>the</strong> last decade would best<strong>in</strong>form <strong>the</strong> aim <strong>of</strong> <strong>the</strong> review.In <strong>the</strong> process <strong>of</strong> develop<strong>in</strong>g <strong>the</strong> scope andmethods for this study, it became clear that <strong>the</strong>re is little consensus on <strong>the</strong>def<strong>in</strong>ition <strong>of</strong> large scale <strong>IT</strong> <strong>in</strong>tervention. Therefore, we used a broad set <strong>of</strong> terms<strong>in</strong> order to maximize <strong>the</strong> sensitivity <strong>of</strong> our search.We accepted at <strong>the</strong> outset that we were not aim<strong>in</strong>g to estimate <strong>the</strong> size <strong>of</strong> aspecific effect. Studies were likely to be very heterogeneous, e.g. <strong>in</strong> differentsett<strong>in</strong>gs, implement<strong>in</strong>g different <strong>IT</strong> systems, evaluat<strong>in</strong>g implementation aga<strong>in</strong>stdiverse outcomes etc., so calculat<strong>in</strong>g a pooled answer was, a priori, notappropriate. However, given <strong>the</strong> anticipated benefits <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> <strong>in</strong> <strong>the</strong><strong>NHS</strong>, 54 we wanted to identify <strong>the</strong> extent to which empirical evidence might support<strong>the</strong>se anticipated benefits.A fur<strong>the</strong>r source <strong>of</strong> heterogeneity is <strong>the</strong> different methods used <strong>in</strong> empiricalstudies. Thus a second objective <strong>of</strong> our review was to describe <strong>the</strong> diversity <strong>of</strong>methods used <strong>in</strong> <strong>the</strong> empirical evaluation <strong>of</strong> large scale <strong>IT</strong> implementation <strong>in</strong>health care. Although we <strong>in</strong>tend to describe <strong>the</strong> empirical f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> <strong>the</strong> mostrelevant papers, we were equally <strong>in</strong>terested <strong>in</strong> <strong>the</strong> methods that have been used.3.3.1. Inclusion / exclusion criteriaThe abstracts or titles <strong>of</strong> <strong>the</strong> complete set <strong>of</strong> references were reviewed by tworeviewers (EP and AH). The ma<strong>in</strong> exclusion criteria at this stage <strong>of</strong> <strong>the</strong> reviewwere studies report<strong>in</strong>g f<strong>in</strong>d<strong>in</strong>gs on micro-<strong>in</strong>terventions, cl<strong>in</strong>ical decisionsupport <strong>in</strong>terventions, <strong>in</strong>ternet advice-based <strong>in</strong>terventions, telemedic<strong>in</strong>e,op<strong>in</strong>ion papers and letters. Fur<strong>the</strong>rmore, reviewers classified all abstracts on<strong>the</strong> basis <strong>of</strong> <strong>the</strong> perceived likelihood that papers (a) conta<strong>in</strong>ed empirical data(empirical: probably empirical: possibly empirical. not empirical) or (b) used<strong>in</strong>novative methodology (methodological; probably methodological; notmethodological). All abstracts classified as be<strong>in</strong>g nei<strong>the</strong>r empirical normethodological by both reviewers, or “nei<strong>the</strong>r” by one reviewer and “possiblyempirical” by <strong>the</strong> o<strong>the</strong>r, were excluded at this stage.26
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsA short pro-forma checklist, completed by two reviewers, was used <strong>in</strong>review<strong>in</strong>g full papers. The aim <strong>of</strong> <strong>the</strong> checklist was to categorise <strong>the</strong> types <strong>of</strong><strong>IT</strong> <strong>in</strong>tervention and sett<strong>in</strong>g evaluated and whe<strong>the</strong>r or not a comparator(ano<strong>the</strong>r technology, or a comparison over time) was identified. When <strong>the</strong>classifications <strong>of</strong> <strong>the</strong> two reviewers differed, a third reviewer was consulted(AM or BR). Based on <strong>the</strong> checklist, only studies that identified all threeparameters clearly (i.e. eligible <strong>IT</strong> <strong>in</strong>tervention, implemented at least ‘acrossdepartments’, and with a comparator) were <strong>in</strong>cluded for data extraction.Follow<strong>in</strong>g <strong>the</strong> completion <strong>of</strong> <strong>the</strong> checklist, <strong>the</strong> reference list from an <strong>in</strong>cludedpaper was searched for any additional studies that might have been missed <strong>in</strong><strong>the</strong> <strong>in</strong>itial search. Agreement between <strong>the</strong> two reviewers was described by <strong>the</strong>kappa statistic.3.3.2. Search strategiesStudies were identified by search<strong>in</strong>g <strong>the</strong> Medl<strong>in</strong>e electronic bibliographicdatabase and <strong>the</strong> electronic Cochrane Library economic evaluation database.The Medl<strong>in</strong>e search was conducted us<strong>in</strong>g <strong>the</strong> follow<strong>in</strong>g MeSH terms: ‘medical<strong>in</strong>formatics applications’ (major head<strong>in</strong>g only), comb<strong>in</strong>ed with any <strong>of</strong> ‘costcontrol’, ‘cost-benefit analysis’ or ‘health care costs’. The Cochrane Librarywas searched us<strong>in</strong>g similar key terms. We limited our searches to Englishlanguage publications between 1995 and August 2006.3.3.3. Data extraction and syn<strong>the</strong>sisThe data-extraction table was designed to summarise <strong>the</strong> ma<strong>in</strong> attributes <strong>of</strong>each study, such as <strong>the</strong> sett<strong>in</strong>g, type <strong>of</strong> <strong>IT</strong> <strong>in</strong>tervention evaluated, year(s) <strong>of</strong>empirical data etc. We also extracted data on costs associated withimplementation (i.e. <strong>in</strong>itial capital outlay), ma<strong>in</strong>tenance (system upgrades etc.),operation and staff<strong>in</strong>g <strong>of</strong> a new <strong>IT</strong> system. All clearly def<strong>in</strong>ed outcomemeasures and reported cost <strong>of</strong>fsets were extracted. We used a standardchecklist for apprais<strong>in</strong>g <strong>the</strong> quality <strong>of</strong> economic evaluations. 46 . The f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong><strong>the</strong> review are reported <strong>in</strong> <strong>the</strong> form <strong>of</strong> a narrative syn<strong>the</strong>sis because <strong>of</strong> <strong>the</strong>extreme heterogeneity between <strong>in</strong>cluded studies.27
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3.4. ResultsThe <strong>in</strong>itial search identified 1725 studies from <strong>the</strong> Medl<strong>in</strong>e database and 529studies from <strong>the</strong> Cochrane Library. The comb<strong>in</strong>ed list <strong>of</strong> references from Medl<strong>in</strong>eand <strong>the</strong> Cochrane library was checked for duplicates and 118 were removed.Figure 3 summarises <strong>the</strong> selection process. A total <strong>of</strong> 149 papers were identifiedfor full text review. An additional 20 papers were identified from <strong>the</strong> bibliographies<strong>of</strong> <strong>the</strong> <strong>in</strong>cluded papers. Overall, 18 studies were identified for data extraction.Agreement between <strong>the</strong> two reviewers with respect to identification <strong>of</strong> papers forfull text review was ‘good’ 55 (weighted Kappa=0.68, CI (0.641, 0.737)), with simpleagreement on 98% <strong>of</strong> papers.Figure 3 : Search resultsTitles and Abstracts identified for review1725Rejected - 1576Full Text Articles Requested for fur<strong>the</strong>rscreen<strong>in</strong>g - 149Reference lists <strong>of</strong> 149 werescreened - additional 20 articleswere requested for fur<strong>the</strong>r screen<strong>in</strong>gRejected - 172 unable to obta<strong>in</strong>Rejected - 116Articles Selected for Data Extraction1Articles Selected for Data Extraction – 1828
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsThe full text review identified a total <strong>of</strong> eighteen studies for <strong>in</strong>clusion. Of thosen<strong>in</strong>e evaluated PACS, five evaluated EMR and four evaluated CPOE (i.e. studies<strong>of</strong> CPOE <strong>in</strong> <strong>the</strong> United States). It is important to note that two <strong>of</strong> <strong>the</strong> studies werebased on <strong>the</strong> same empirical data. 56,57 Fur<strong>the</strong>rmore, it was discovered that, apartfrom variations <strong>in</strong> titles and abstracts, three studies were virtually identical 58-60 ;<strong>the</strong>refore, only one <strong>of</strong> <strong>the</strong>se was <strong>in</strong>cluded.3.4.1. Study descriptionTable 6 summarises <strong>the</strong> studies <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> review. The majority wereconducted <strong>in</strong> <strong>the</strong> US 36,50-52,58,61-66 (11 <strong>of</strong> 16), three 49,53,67 <strong>in</strong> Scand<strong>in</strong>avia (two <strong>in</strong>F<strong>in</strong>land and one <strong>in</strong> Sweden) and two <strong>in</strong> <strong>the</strong> UK. 56,57 All but one study <strong>of</strong> <strong>the</strong>effects <strong>of</strong> PACS were conducted <strong>in</strong> a hospital or medical centre sett<strong>in</strong>g. Two<strong>of</strong> <strong>the</strong> four studies that looked at <strong>the</strong> effects <strong>of</strong> CPOE were conducted at adepartmental level across a number <strong>of</strong> hospitals 36,63 and <strong>the</strong> rema<strong>in</strong><strong>in</strong>g twowith<strong>in</strong> a s<strong>in</strong>gle hospital. 51,52 All studies evaluat<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> EMR wereconducted across a number <strong>of</strong> primary care practices.The evaluation design varied considerably across <strong>the</strong> <strong>in</strong>cluded studies. Fourstudies 49-52 used ei<strong>the</strong>r an account<strong>in</strong>g or f<strong>in</strong>ancial approach, such as activitybasedanalysis, return on <strong>in</strong>vestment (ROI) or value on <strong>in</strong>vestment. Twostudies were cost comparison, before and after implementation. 53,64 Onestudy only evaluated <strong>the</strong> effectiveness <strong>of</strong> <strong>IT</strong> implementation 65 and one studywas a pilot RCT. 62 The rema<strong>in</strong><strong>in</strong>g 8 studies used some form <strong>of</strong> ‘before andafter’ comparison <strong>of</strong> costs or benefits. 36,56-58,61,62,66,673.4.2. Methodological qualityTable 7 shows <strong>the</strong> results <strong>of</strong> <strong>the</strong> quality assessment <strong>of</strong> <strong>the</strong> identified studies.Ten studies clearly identified compet<strong>in</strong>g alternatives. 36,49,50,56-58,61,63,65,67 Apartfrom Bryan et al., 56 <strong>the</strong> studies reported ei<strong>the</strong>r partial <strong>in</strong>cremental analysis (i.e.just costs or benefits) or no analysis at all; 7 studies reported <strong>in</strong>crementalanalysis <strong>of</strong> <strong>the</strong> effects, and one <strong>of</strong> costs. 67 The results <strong>of</strong> sensitivity analysiswere reported <strong>in</strong> six studies. 49,53,56,57,63,6629
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3.4.3. Economic f<strong>in</strong>d<strong>in</strong>gs and methods <strong>of</strong> evaluationApart from <strong>the</strong> studies that used a f<strong>in</strong>ancial approach, o<strong>the</strong>r studies werepartial economic evaluations because <strong>the</strong>y only evaluated differences <strong>in</strong> costs,and not health benefits. Table 8 fur<strong>the</strong>r summarises <strong>the</strong> results <strong>of</strong> <strong>the</strong><strong>in</strong>cluded studies by <strong>in</strong>tervention type. The perspective was identified <strong>in</strong> fourstudies and implied <strong>in</strong> <strong>the</strong> text for four o<strong>the</strong>r studies. One adopted a societalperspective 53 and <strong>the</strong> rema<strong>in</strong><strong>in</strong>g seven adopted a hospital 52,56,57,63,65,67 ordepartmental perspective. 66 Only five studies applied discount<strong>in</strong>g. 51,53,56,57,65The majority <strong>of</strong> studies compared pre and post implementation effects. All buttwo evaluations <strong>of</strong> <strong>the</strong> effects <strong>of</strong> PACS used a pre and post comparison with<strong>the</strong> pre-PACS comparator identified as film-based imag<strong>in</strong>g. One studyreported changes <strong>in</strong> <strong>the</strong> outcome measure dur<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> PACSand once PACS was fully implemented, fur<strong>the</strong>r compar<strong>in</strong>g those f<strong>in</strong>d<strong>in</strong>gs withpre-PACS data. 65 Ano<strong>the</strong>r study compared <strong>the</strong> effects <strong>of</strong> PACS versus PACSwith <strong>the</strong> addition <strong>of</strong> CR (computer radiography). 50 Maass et al. evaluated <strong>the</strong>effects <strong>of</strong> implement<strong>in</strong>g PACS <strong>in</strong> addition to a film-based system and used<strong>the</strong>ir f<strong>in</strong>d<strong>in</strong>gs to estimate <strong>the</strong> costs <strong>of</strong> a full-scale PACS implementation. 67Similarly, studies evaluat<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> EMR and CPOE implementationscompared outcomes and costs before and after <strong>in</strong>troduction.3.4.4. CostsAll but one <strong>of</strong> <strong>the</strong> 7 studies <strong>of</strong> <strong>the</strong> effects <strong>of</strong> PACS reported <strong>the</strong> costs <strong>of</strong>ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g and operat<strong>in</strong>g <strong>the</strong> new system. In addition, two studies 49,67reported <strong>the</strong> <strong>in</strong>itial capital cost <strong>of</strong> implement<strong>in</strong>g PACS and staff<strong>in</strong>g costsassociated with us<strong>in</strong>g <strong>the</strong> system. Wagner et al. did not report any costs.Only two <strong>of</strong> <strong>the</strong> five studies <strong>of</strong> <strong>the</strong> effects <strong>of</strong> CPOE implementation reporteddata on costs. Both Wang et al. and Kaushal et al. <strong>in</strong>cluded <strong>the</strong> costs <strong>of</strong>ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g/operat<strong>in</strong>g and staff<strong>in</strong>g associated with <strong>the</strong> new system; <strong>the</strong> formeralso reported <strong>the</strong> <strong>in</strong>itial cost <strong>of</strong> implement<strong>in</strong>g CPOE. Most studies <strong>of</strong> <strong>the</strong>effects <strong>of</strong> EMR <strong>in</strong>cluded <strong>the</strong> <strong>in</strong>itial costs <strong>of</strong> implementation; three also <strong>in</strong>cluded<strong>the</strong> costs associated with EMR operation and ma<strong>in</strong>tenance. 53,61,6230
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsTable 6: Summary <strong>of</strong> <strong>the</strong> designs used, <strong>in</strong>terventions and health care sett<strong>in</strong>gs evaluated by <strong>in</strong>cluded studiesAuthorArias-Vimarlund et al.1996Barlow et al.2004Miller et al.2005Sachs2000Study Year(s)Country (Currency?)1995Sweden (SEK)2002-2003USA (USD)2004-2005USA (USD)?USA (USD)<strong>IT</strong> Intervention <strong>Evaluation</strong> Design Health Care sett<strong>in</strong>gEMR Comparative case study Two urban primary healthcentresEMREHRElectronic HealthRecordsEMRBefore and AfterCost –Sav<strong>in</strong>gsAnalysis <strong>of</strong> costs andbenefitsBefore and afterCost comparisonBefore and AfterMulti- Specialty Cl<strong>in</strong>icA group <strong>of</strong> primary carepracticesAmbulatory cl<strong>in</strong>icsWang et al.2003Kaushal et al.20065-year period (year notstated)USA (USD)1993-2002USA (USD)EMRCPOEF<strong>in</strong>ancial cost<strong>in</strong>g and cost<strong>of</strong>fsetanalysisBefore and afterReturn on InvestmentAnalysisA Hypo<strong>the</strong>tical Primary careproviderWomen’s hospitalMekhjian et al.2002Overhage et al.20022000-2001USA (USD)1995-1996USA (USD)CPOECPOEAnalysis <strong>of</strong> benefits andcost-<strong>of</strong>fsetBefore and AfterA pilot RCT – value <strong>of</strong>accessInpatient nurs<strong>in</strong>g unitEmergency departmentTaylor et al.20021999-2002USA ( USD)CPOEValue on InvestmentAnalysisUrban Medical centre31
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsTable 6: cont<strong>in</strong>uedAuthorAlanene et al.1998Study Year(s)Country (Currency?)1994F<strong>in</strong>land (FIM)<strong>IT</strong> Intervention <strong>Evaluation</strong> Design Health Care sett<strong>in</strong>gCR – m<strong>in</strong>i-PACSCost analysis us<strong>in</strong>g activitybasedaccount<strong>in</strong>gMid-size general hospitalBryan et al.2000Bryan et al.199991/92-96/97UK (GBP)1996-1997UK (GBP)PACSPACSAnalysis <strong>of</strong> costs andbenefitsBefore and afterCosts and sav<strong>in</strong>gs analysisTime series trend analysisSecondary Care HospitalSecondary Care HospitalChan et al.2002Maass et al.20011998-2001USA (USD)1998F<strong>in</strong>land (FIN)PACSPACSReturn on InvestmentBefore and afterassessment <strong>of</strong> productivityand satisfactionAnalysis <strong>of</strong> costs – beforeand afterHospitalUniversity Central hospitalSiegel et al.1998(also pub. 1998 and 2003)1993-1996USA (USD)PACSAnalysis <strong>of</strong> cost-<strong>of</strong>fsets andbenefitBefore and afterMedical CentreWanger et al.20021995-2000USA (USD)PACSAssessment <strong>of</strong> benefitsBefore and AfterDepartment <strong>of</strong> radiology32
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsTable 7: Results <strong>of</strong> <strong>the</strong> quality assessment <strong>of</strong> <strong>in</strong>cluded studiesWas a well-def<strong>in</strong>ed question posed <strong>in</strong> answerableform?Was a comprehensive description <strong>of</strong> <strong>the</strong> compet<strong>in</strong>galternative given?Was <strong>the</strong> effectiveness <strong>of</strong> <strong>the</strong> programme or servicesestablished (e.g. randomized, controlled cl<strong>in</strong>ical trial,overview <strong>of</strong> cl<strong>in</strong>ical literature etc.)?Were all <strong>the</strong> important and relevant costs andconsequences <strong>of</strong> each alternative identified?Were costs and consequences measured accurately<strong>in</strong> appropriate physical units (e.g. hours <strong>of</strong> nurs<strong>in</strong>gtime, number <strong>of</strong> physician visits, lost work-days)?Ref. 49 53 61 57 56 50 51 67 36 62 63 58 52 65 66 64Y Y Y Y Y Y Y Y Y Y Y Y/NC Y/NC Y Y YY NC Y Y Y Y NC Y Y NC Y Y NC Y NC NCY Y Y Y Y NC NC Y Y Y Y Y NC Y Y YP Y Y Y Y Y Y P P Y Y Y P Y Y YP Y NC Y Y Y Y Y P Y Y Y Y P Y NCWere costs and consequences valued credibly? Y Y NC Y Y NC Y Y Y Y P Y NC Y Y YWere costs and consequences adjusted for differentialtim<strong>in</strong>g?Was an <strong>in</strong>cremental analysis <strong>of</strong> costs and/orconsequences <strong>of</strong> alternatives performed?Was allowance made for uncerta<strong>in</strong>ty <strong>in</strong> <strong>the</strong> estimates<strong>of</strong> costs and consequences?Did <strong>the</strong> presentation and discussion <strong>of</strong> study results<strong>in</strong>clude all issued <strong>of</strong> concern to users?NC Y N Y Y N Y N N N N N N N Y YN N N P Y N N P P P P N P P P NY Y N Y Y N N N N N Y N N N Y NY Y Y Y Y Y Y Y Y Y Y NC Y Y Y YY – Yes; N- No; NC – Not Clear; P – Partially33
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsTable 8: Summary <strong>of</strong> <strong>the</strong> results <strong>of</strong> <strong>the</strong> <strong>in</strong>cluded studiesRef Perspective DiscountRateComparison Costs OutcomeMeasure(s)53 Societal 4% Not clear Implementation,Ma<strong>in</strong>tenance,Operational,Staff<strong>in</strong>g61 NS NS Pre-EMR vs. Storage andNAPost-EMRchart62 NS NS ? before andafter EHRma<strong>in</strong>tenanceImplementationandMa<strong>in</strong>tenanceCost OffsetResultsNA Time saved Total costs – SEK2,093,000Time-saved SEK72,900NPV - SEK2,020,100NASpace requirement;TranscriptionCompensation rates(records and staff)64 NS NS ? Implementation NA Paper andtranscription66 Health Care 5% 2 ? Implementation,NAAverted costs andOrg.Ma<strong>in</strong>tenance,revenuesand Staff<strong>in</strong>g51 NS 7% Not clear Operat<strong>in</strong>g andstaff tra<strong>in</strong><strong>in</strong>g36 NS NS Pre-CPOE vs.post- CPOE63 Hospital 1 NS Hosp. withCPOE vs.hosp. withoutCPOE52 Med. NS ? before andCentre 1 after CPOEADE; dosagenumberNA LoS Time saved;admissionsNATest order rate;charge perencounterNS- Not Stated; NA- Not Applicable; NPV – Net Present Value; ADE – Adverse Drug Event; LoS – Length <strong>of</strong> Stay1 Perspective implied from <strong>the</strong> text; * - assumed; 2 Assumed.Sav<strong>in</strong>gs – space req. $248,000; transcription exp.$380,000Sav<strong>in</strong>gs: Increased cod<strong>in</strong>g level - $16,929Efficiency-related sav<strong>in</strong>g or revenue ga<strong>in</strong>s - $16,929per FTE per provider; The total average benefit$32,737 per FTE per provider.Sav<strong>in</strong>g: transcription - $9,967/provider (1 st y); paper- $41,795; NPV – over 3 years $2,695Present value <strong>of</strong> annual costs over 5-year period -$42,900Present value <strong>of</strong> annual benefits - $108,500.Present value <strong>of</strong> net benefit - $86,400.Drug costs Sav<strong>in</strong>g: ADE prevention $3.7 million and $4.9million - specific or expensive drug Decrease <strong>in</strong> <strong>the</strong>mean LoS by 0.2 days (p=0.009) Decrease <strong>in</strong> ADEby 0.81 /1000 patient daysNADecrease <strong>in</strong> turn-around time decreased by 64%(p
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic ImplicationsTable 8: cont<strong>in</strong>uedRef. Perspective DiscountRateComparison Costs OutcomeMeasure(s)49 ? NS PACS vs. Film Implementation,Ma<strong>in</strong>tenance,Operational,Staff<strong>in</strong>g57 Hospital 6% PACS vs. pre- Ma<strong>in</strong>tenance andPACS Operational56 Hospital 6% PACS vs. pre-PACS50 NS NS PACS vs.PACS+CR67 Hospital 1 NS Film vs.Film+PACS58 NS NS Pre-PACS vs.Post-PACS65 RadiologyDept. 1 NS Pre-PACS vs.dur<strong>in</strong>g/postPACSMa<strong>in</strong>tenance,Operational andStaff<strong>in</strong>gFilm imag<strong>in</strong>grelated andPACSma<strong>in</strong>tenance,operat<strong>in</strong>g andf<strong>in</strong>anc<strong>in</strong>gImplementation,Ma<strong>in</strong>tenance,Operational,Staff<strong>in</strong>gMa<strong>in</strong>tenanceNACost OffsetResultsNA Image process<strong>in</strong>g PCAS Image process<strong>in</strong>g – FIM39Film-based image process. – FIM25The total cost <strong>of</strong> image process. – up by 9%NA Time saved Sav<strong>in</strong>gs: Prep-time - £36,000 per annum and noExam time £41,000 per annum. Image related time£9,000 per annum. Consultation time (4.3 versus3.7 m<strong>in</strong>utes).Rate <strong>of</strong> imagerejection andradiation dose;PhysicianSatisfactionPhysiciansatisfaction;change <strong>in</strong>productivityNA Decrease <strong>in</strong> image repeat rate by 2.6%Decrease <strong>in</strong> radiation dose by 20%Increase <strong>in</strong> physician satisfaction with image qualityby 10%NA General productivity benefit – 91%Radiologist productivity benefit – 100%Increased <strong>in</strong> technologist productivity by 58%Sav<strong>in</strong>g <strong>of</strong> $500,000 per annumNA Capital costs Decrease <strong>in</strong> personnel costs - FIM 800,000 ;decrease <strong>in</strong> supplies costs - FIM 190,000Increase <strong>in</strong> equipment expenditure - FIM 2,000,000Overall <strong>in</strong>crease <strong>of</strong> costs by 16%“unread” images;image retake rate;Rate <strong>of</strong> <strong>in</strong>cidentalf<strong>in</strong>d<strong>in</strong>g; number <strong>of</strong>follow-upsFilm, folders andchemicals; PersonnelNS- Not Stated; NA- Not Applicable; NPV – Net Present Value; ADE – Adverse Drug Event; LoS – Length <strong>of</strong> Stay1 Perspective implied from <strong>the</strong> text; * - assumed;2 Assumed.Decrease <strong>in</strong> “unread” images by 7.7%Decrease <strong>in</strong> image retake by 4.2%Decrease <strong>in</strong> film costs by $190,000 AdditionalSav<strong>in</strong>g <strong>in</strong> film folder and chemicals <strong>of</strong> $15,000.Sav<strong>in</strong>gs <strong>in</strong> personnel costs - $100,000 per year.NA Increase <strong>in</strong> <strong>the</strong> rate <strong>of</strong> <strong>in</strong>cidental f<strong>in</strong>d<strong>in</strong>gs - 163%(p
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3.4.5. Results <strong>of</strong> cost-<strong>of</strong>fset and o<strong>the</strong>r outcome measuresPACSThe results <strong>of</strong> studies <strong>of</strong> <strong>the</strong> effects <strong>of</strong> PACS implementation showed apositive effect on <strong>the</strong> quality <strong>of</strong> images taken. 50,57,58 Wagner et al. showed that<strong>the</strong> <strong>in</strong>creased quality <strong>of</strong> images had a positive effect on <strong>the</strong> rate <strong>of</strong> <strong>in</strong>cidentalf<strong>in</strong>d<strong>in</strong>gs (i.e. cl<strong>in</strong>ical f<strong>in</strong>d<strong>in</strong>gs outside <strong>of</strong> <strong>the</strong> primary area <strong>of</strong> <strong>in</strong>terest). 65Theseresults are supported by Maass et al., 67 and Bryan et al., 56 who reportedpositive changes <strong>in</strong> <strong>the</strong> productivity <strong>of</strong> physician and o<strong>the</strong>r staff and greatersatisfaction due to PACS implementation. Studies that used cost-<strong>of</strong>fset tomeasure <strong>the</strong>ir results showed a decrease <strong>in</strong> costs, which resulted from adecrease <strong>in</strong> <strong>the</strong> time allocated to image process<strong>in</strong>g. 56,58Two studies reportedan <strong>in</strong>crease <strong>in</strong> <strong>the</strong> total cost <strong>of</strong> imag<strong>in</strong>g after implementation <strong>of</strong> PACS. Alanenet al. found that <strong>the</strong> total cost <strong>of</strong> image process<strong>in</strong>g <strong>in</strong>creased by 9% over <strong>the</strong>study period when compared to conventional film-based imag<strong>in</strong>g. 49Similarly,Maass et al. reported that overall costs <strong>in</strong>creased by 16% after PACSimplementation, as a result <strong>of</strong> a substantial <strong>in</strong>itial capital outlay. 67EMRThree <strong>of</strong> <strong>the</strong> four studies evaluat<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> EMR 61,62,64 reported costsav<strong>in</strong>gs as a result <strong>of</strong> a decrease <strong>in</strong> <strong>the</strong> time needed for record transcriptionand space requirements. Arias-Vimarlund et al. reported a negative netpresent value (NPV) <strong>of</strong> EMR system implementation over <strong>the</strong> 12-mon<strong>the</strong>valuation period, whereas Sachs et al. showed a small, but positive NPVover <strong>the</strong> study period (3 years).CPOEFour <strong>of</strong> <strong>the</strong> five studies exam<strong>in</strong><strong>in</strong>g <strong>the</strong> consequences <strong>of</strong> CPOEimplementation 36 reported positive effects <strong>of</strong> <strong>the</strong> new system on <strong>the</strong> length <strong>of</strong>stay, adverse drug events (ADE) and prescription errors. 51,52 Two studies 36,52reported positive cost-<strong>of</strong>fsets as a result <strong>of</strong> a decrease <strong>in</strong> turn-around andorder completion times, and sav<strong>in</strong>gs from personnel and cl<strong>in</strong>ical staff. Wanget al. reported a positive net present benefit <strong>of</strong> CPOE implementation. 6636
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3.5. DiscussionThe f<strong>in</strong>ite nature <strong>of</strong> available resources mandates <strong>the</strong> need for thorougheconomic evaluation, which <strong>in</strong> turn will help a decision-maker determ<strong>in</strong>e whe<strong>the</strong>ra particular technology should be adopted. This need becomes even greaterwhen implementation <strong>of</strong> a technology <strong>in</strong>volves significant upfront <strong>in</strong>vestment. Theaim <strong>of</strong> this study was to review <strong>the</strong> exist<strong>in</strong>g literature on <strong>the</strong> economic implications<strong>of</strong> large scale <strong>IT</strong> implementations <strong>in</strong> health care. Specifically, we were <strong>in</strong>terested<strong>in</strong> <strong>the</strong> empirical results, methodological approach and rigour.Key f<strong>in</strong>d<strong>in</strong>gs from <strong>the</strong> review <strong>in</strong>cluded a positive effect on <strong>the</strong> quality <strong>of</strong> imag<strong>in</strong>gwith PACS, a decrease <strong>in</strong> <strong>the</strong> number <strong>of</strong> prescription errors and a decrease <strong>in</strong>adverse drug events (ADE) with CPOE, and a decrease <strong>in</strong> <strong>the</strong> time need forrecord upkeep with EMR. However, <strong>the</strong> results <strong>of</strong> <strong>the</strong> studies evaluat<strong>in</strong>g f<strong>in</strong>ancialimplications were mixed. Many studies noted that <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> time period overwhich <strong>the</strong> evaluation takes place fur<strong>the</strong>r <strong>in</strong>creases <strong>the</strong> benefit and/or decreasescosts. Overall, we found that <strong>the</strong>re is lack <strong>of</strong> empirical data on this subject, whichsignificantly impairs <strong>the</strong> quality <strong>of</strong> <strong>the</strong> research.We found that none <strong>of</strong> <strong>the</strong> studies directly evaluated <strong>the</strong> effects <strong>of</strong> implementation<strong>of</strong> a new <strong>IT</strong> system on health outcomes.However, based on some <strong>of</strong> <strong>the</strong>f<strong>in</strong>d<strong>in</strong>gs, such as an <strong>in</strong>crease <strong>in</strong> <strong>the</strong> rate <strong>of</strong> <strong>in</strong>cidental f<strong>in</strong>d<strong>in</strong>g 65 and decreaseddose <strong>of</strong> radiation 57 associated with implementation <strong>of</strong> PACS, <strong>the</strong> potential existsfor overall health benefits. Similarly, decreased rates <strong>of</strong> drug errors 52 and lengths<strong>of</strong> stay 36 reported <strong>in</strong> <strong>the</strong> studies evaluat<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> CPOE implementation<strong>in</strong>dicate potential health benefits.With respect to methodological rigour, <strong>the</strong> review identified a number <strong>of</strong> technicalconcerns with <strong>the</strong> exist<strong>in</strong>g evaluations.51-53,62 ,64,66clearly started <strong>in</strong> six <strong>of</strong> <strong>the</strong> identified studies. PartialThe comparative technology was not<strong>in</strong>crementalanalysis reported by <strong>the</strong> <strong>in</strong>cluded studies detracts from <strong>the</strong> quality <strong>of</strong> <strong>the</strong>evaluation.More than half <strong>of</strong> <strong>the</strong> reviewed studies did not report results <strong>of</strong>sensitivity analyses, which fur<strong>the</strong>r limits <strong>in</strong>terpretation <strong>of</strong> <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Reviews by Clapm et al. 48 and Chaudhry et al., 17 which focused on <strong>the</strong> effects <strong>of</strong>health <strong>in</strong>formation technology on quality, efficiency, and costs <strong>of</strong> health care,37
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implicationsfound similar results. They also highlighted that disparate evaluation methods andheterogeneity associated with <strong>the</strong> types <strong>of</strong> <strong>in</strong>tervention causes significantdifficulties <strong>in</strong> assess<strong>in</strong>g reported f<strong>in</strong>d<strong>in</strong>gs and draw<strong>in</strong>g conclusions.3.5.1. Strengths and weaknessThe ma<strong>in</strong> strength <strong>of</strong> this review is <strong>the</strong> systematic approach used to identifyand assess <strong>the</strong> methodological quality <strong>of</strong> <strong>the</strong> literature. We protected aga<strong>in</strong>streviewer bias by us<strong>in</strong>g two reviewers to select studies. However, <strong>the</strong>re arethree limitations that need to be acknowledged.Firstly, <strong>the</strong>re is <strong>the</strong> possibility that relevant literature was not identified due to<strong>the</strong> search strategy we used. We excluded non-English publications andfocused on <strong>the</strong> medical literature by us<strong>in</strong>g MedL<strong>in</strong>e and <strong>the</strong> Cochrane library.However, subsequent search<strong>in</strong>g <strong>of</strong> cited references produced little additionalliterature with<strong>in</strong> or beyond <strong>the</strong> <strong>in</strong>dexed medical literature. Therefore, webelieve that it is unlikely we missed any rigorously conducted economicevaluations and that any empirical studies we missed would probably havebeen <strong>of</strong> lower methodological quality than those we identified.Secondly, it could be argued that <strong>the</strong> potential for publication bias is high,particularly for retrospectively conducted studies. Possible reasons <strong>in</strong>clude(retrospectively) elect<strong>in</strong>g not to study 'unsuccessful' implementations, fail<strong>in</strong>g tosubmit or publish non-positive studies, or select<strong>in</strong>g outcome measures <strong>in</strong>order to obta<strong>in</strong> positive f<strong>in</strong>d<strong>in</strong>gs. We identified one case <strong>of</strong> multiple publication<strong>of</strong> <strong>the</strong> same study. 58-60Thirdly, we only considered studies that conta<strong>in</strong>ed at least some element <strong>of</strong>primary analysis, so that purely hypo<strong>the</strong>tical analyses were not reviewed. Therationale for this dist<strong>in</strong>ction is that empirical studies have demonstrated that<strong>the</strong> expected/<strong>the</strong>oretical sav<strong>in</strong>gs assumed for non-empirical models are nottypically realised. 68 However, it should be noted that <strong>the</strong>se excluded analyses,if taken at face value, do suggest that <strong>IT</strong> programmes <strong>of</strong> this nature could becost-sav<strong>in</strong>g. 6938
Report to SDO for NCRS ProjectReview <strong>of</strong> Economic Implications3.5.2. ConclusionIn conclusion, based on <strong>the</strong> studies we found, <strong>the</strong> economic consequences <strong>of</strong><strong>in</strong>tegrat<strong>in</strong>g a major <strong>IT</strong> system <strong>in</strong>to health care services are extremelyuncerta<strong>in</strong>. Moreover, we found no consensus among studies with respect toan appropriate methodological approach <strong>of</strong> evaluat<strong>in</strong>g a complex <strong>in</strong>tervention(i.e. <strong>IT</strong> systems). Few studies assessed <strong>the</strong> potential for substantialimprovements <strong>in</strong> <strong>the</strong> quality <strong>of</strong> health care associated with <strong>the</strong> <strong>in</strong>troduction <strong>of</strong> anew <strong>IT</strong> system and potential cost-sav<strong>in</strong>gs. Yet, decisions to implement suchsystems (e.g. NPf<strong>IT</strong>/Connect<strong>in</strong>g for Health) are <strong>in</strong>fluenced by claims orexpectations <strong>of</strong> health benefits as well as ga<strong>in</strong>s <strong>in</strong> <strong>the</strong> efficiency <strong>of</strong> <strong>the</strong>provision <strong>of</strong> health care. The need for a comprehensive assessment <strong>of</strong> <strong>the</strong>economic consequences <strong>of</strong> implement<strong>in</strong>g large scale <strong>IT</strong> systems is necessarybecause such system have substantial f<strong>in</strong>ancial implications. Until such anassessment is undertaken, considerable uncerta<strong>in</strong>ty will rema<strong>in</strong> about <strong>the</strong>efficiency and health ga<strong>in</strong>s, and <strong>the</strong> cost-effectiveness, <strong>of</strong> such programmes.39
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study4. Methods for <strong>the</strong> qualitative and quantitative empirical elements <strong>of</strong> <strong>the</strong> study4.1. EthicsEthics approval for <strong>the</strong> study was granted by <strong>the</strong> Trent Multi-centre ResearchEthics Committee <strong>in</strong> June 2003 (ref. MREC/03/4/017). A subsequent amendmentwas submitted <strong>in</strong> October 2004, seek<strong>in</strong>g approval for <strong>the</strong> study to obta<strong>in</strong> andanalyse anonymised data for <strong>in</strong>dividual patients. This amendment was approved.Annual progress reports were submitted to <strong>the</strong> Multi-centre Research EthicsCommittee <strong>in</strong> 2004, 2005 and 2006, and a f<strong>in</strong>al report <strong>in</strong> May 2007.4.2. Methods for <strong>the</strong> qualitative studyQualitative methods were used to provide an <strong>in</strong>-depth organisational analysis <strong>of</strong><strong>the</strong> processes and impacts <strong>of</strong> implement<strong>in</strong>g electronic patient records (i.e. localand national solutions that form part <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>) <strong>in</strong> four acute Trusts <strong>in</strong> England.Specifically, <strong>the</strong> qualitative element <strong>of</strong> <strong>the</strong> study addressed <strong>the</strong> follow<strong>in</strong>g twoobjectives:1. To describe <strong>the</strong> context for implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> <strong>in</strong> England,exam<strong>in</strong><strong>in</strong>g actual and perceived barriers, and opportunities to facilitateimplementation.2. To explore how new electronic applications, <strong>of</strong> <strong>the</strong> k<strong>in</strong>d which will beimplemented by <strong>the</strong> NPf<strong>IT</strong>, are experienced by end-users (<strong>NHS</strong> staff),describ<strong>in</strong>g any impact on work<strong>in</strong>g practices.4.2.1. Theoretical frameworkWe <strong>in</strong>tended to carry out <strong>the</strong> evaluation <strong>in</strong> a way that took <strong>in</strong>to account <strong>the</strong>complexity both <strong>of</strong> <strong>the</strong> ‘programme’ (i.e. implementation <strong>of</strong> EPRs) and <strong>the</strong>‘context’ with<strong>in</strong> which it is <strong>in</strong>troduced (i.e. a number <strong>of</strong> acute <strong>NHS</strong> Trusts).This approach is similar to that <strong>of</strong> ‘contextualism’ which takes account <strong>of</strong> <strong>the</strong>content, process and context <strong>in</strong> studies <strong>of</strong> organisational change andemphasises that <strong>the</strong> effects <strong>of</strong> organisational change are multi-layered andcomplex. 70,71 We have used methods based on those used by organisationalprocess research 72 which explores patterns with<strong>in</strong> organisations, and identifies40
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studytrends or tendencies over time. To address <strong>the</strong>se complexities, multiple levels<strong>of</strong> analysis have been used to study process phenomena which are fluid <strong>in</strong>character and which “spread out over both time and space”. 73This type <strong>of</strong>research uses comparative and longitud<strong>in</strong>al case studies to explore variation<strong>in</strong> ‘outcome’ (i.e. consequences). In this case, <strong>the</strong> ‘comparison’ element <strong>of</strong> <strong>the</strong>study is with<strong>in</strong> and between organisations implement<strong>in</strong>g EPRs. In o<strong>the</strong>rwords, we aimed to document and analyse change over time, and compare<strong>the</strong> impact <strong>of</strong> implementation <strong>of</strong> EPRs between different organisations us<strong>in</strong>gboth quantitative and qualitative methods. Similar methods have been usedsuccessfully before. 68Research <strong>in</strong>to <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong> health care is characterised bydiversity. The field <strong>of</strong> <strong>in</strong>quiry is fragmented and suffers from a lack <strong>of</strong> cohesionand <strong>the</strong>oretical focus. 7 Sociological approaches to medical work <strong>of</strong>fer someguidance, <strong>in</strong> provid<strong>in</strong>g shared start<strong>in</strong>g po<strong>in</strong>ts considered necessary for<strong>in</strong>creas<strong>in</strong>g scientific understand<strong>in</strong>g <strong>of</strong> <strong>IT</strong> development. Primarily this approachsees technological <strong>in</strong>novation as a social process. The focus is on <strong>the</strong> nature<strong>of</strong> medical work and <strong>the</strong> <strong>in</strong>terrelated and dynamic relationship betweentechnology and <strong>the</strong> social environment. 74In tak<strong>in</strong>g this approach whencollect<strong>in</strong>g and analys<strong>in</strong>g our data, <strong>the</strong> ‘<strong>the</strong> user’ is seen as play<strong>in</strong>g a centralrole – with technological development not seen as ‘l<strong>in</strong>ear’, but altoge<strong>the</strong>r morehuman and messy. The impact <strong>of</strong> <strong>the</strong> <strong>in</strong>novation on <strong>the</strong> organisation hasrepercussions that feed back on <strong>the</strong> shape, use and function <strong>of</strong> <strong>the</strong> <strong>IT</strong>, mak<strong>in</strong>git important to see EPR development <strong>in</strong> terms <strong>of</strong> a dynamic whole. 26technology and user <strong>in</strong>teract and mutually transform each o<strong>the</strong>r, <strong>of</strong>ten <strong>in</strong>unexpected ways.There were two sociological approaches to technology implementation thatappeared particularly useful when attempt<strong>in</strong>g to focus our data collection andsubsequent analysis. Theories <strong>of</strong> organisational change and strategicdevelopment have been developed to provide a better understand<strong>in</strong>g <strong>of</strong> <strong>the</strong>full range <strong>of</strong> organisational factors affect<strong>in</strong>g <strong>the</strong> strategic development <strong>of</strong> <strong>IT</strong>.They see <strong>IT</strong> as one key component <strong>of</strong> <strong>the</strong> wider organisational context. Wedrew upon a range <strong>of</strong> organisational process research <strong>in</strong> an attempt toaddress both <strong>in</strong>dividual and organisational patterns <strong>of</strong> change, with<strong>in</strong> andThe41
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studyacross our sites, and identify trends or tendencies over time. 75 However, <strong>in</strong>develop<strong>in</strong>g <strong>the</strong> first <strong>in</strong>terview schedule (level 1), <strong>the</strong> work <strong>of</strong> McKersie andWalton (<strong>the</strong> M<strong>IT</strong>90s framework <strong>of</strong> organisational change and effectiveimplementation <strong>of</strong> <strong>IT</strong>) 76was particularly useful. Us<strong>in</strong>g this framework, <strong>the</strong>impact <strong>of</strong> EPRs is seen as be<strong>in</strong>g crucially affected by three central forces - <strong>the</strong>structure <strong>of</strong> <strong>the</strong> organisation, management processes, and <strong>the</strong> personality androles <strong>of</strong> <strong>in</strong>dividual project leaders.The M<strong>IT</strong>90s framework also outl<strong>in</strong>esfactors - such as policies, <strong>the</strong> <strong>IT</strong> systems itself, and behavioural conditions(such as motivation) as determ<strong>in</strong>ant for success. In develop<strong>in</strong>g <strong>the</strong> <strong>in</strong>terviewschedules, <strong>the</strong> work <strong>of</strong> Pettigrew et al 77 is ano<strong>the</strong>r key text. From study<strong>in</strong>gstrategic service change <strong>in</strong> <strong>the</strong> <strong>NHS</strong>, <strong>the</strong> author derived a set <strong>of</strong> eight<strong>in</strong>terl<strong>in</strong>ked contextual factors necessary for build<strong>in</strong>g receptive change:• Environmental pressure• Supportive organisational culture• Change agenda and its locale• Simplicity and clarity <strong>of</strong> goals and priorities• Cooperative <strong>in</strong>ter-organisation networks• Managerial-cl<strong>in</strong>ical relations• Key people lead<strong>in</strong>g change• Quality and coherence <strong>of</strong> policyData collection from <strong>the</strong> second stage <strong>of</strong> analysis (level 2) draws on <strong>the</strong>diffusion <strong>of</strong> <strong>in</strong>novations <strong>the</strong>ory (DOI). 78This work is useful because it wasdeveloped to expla<strong>in</strong> <strong>the</strong> acceptance, or o<strong>the</strong>rwise, <strong>of</strong> product <strong>in</strong>novations byend-users or consumers. DOI primarily concerns <strong>the</strong> study <strong>of</strong> “<strong>the</strong> process bywhich an <strong>in</strong>novation is communicated through certa<strong>in</strong> channels over timeamong members <strong>of</strong> a social system” (p.5). The first element that determ<strong>in</strong>esdiffusion is <strong>the</strong> <strong>in</strong>novation itself, <strong>in</strong> our case <strong>the</strong> EPR. DOI <strong>the</strong>ory sets out fiveattributes which are important <strong>in</strong> assess<strong>in</strong>g <strong>the</strong> potential <strong>of</strong> this <strong>in</strong>novation i.e.how quickly and successfully it will be adopted. These <strong>in</strong>clude:• The relative advantage <strong>of</strong> <strong>the</strong> <strong>in</strong>novation – such as <strong>the</strong> economic value,social value, convenience, and satisfaction <strong>the</strong> EPR affords.• Compatibility - <strong>the</strong> extent to which <strong>the</strong> EPR is seen as consistent wi<strong>the</strong>xist<strong>in</strong>g values, experiences, and needs <strong>of</strong> <strong>the</strong> adopters (hospital staff).42
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study• Complexity – <strong>the</strong> degree to which <strong>the</strong> EPR is difficult to understand anduse.• Trialability – <strong>the</strong> degree to which <strong>the</strong> EPR can be experimented with andtested and• Observability – <strong>the</strong> degree to which <strong>the</strong> results <strong>of</strong> <strong>the</strong> EPR are visible too<strong>the</strong>rs.The second factor <strong>in</strong> diffusion is communication, i.e. <strong>the</strong> process <strong>of</strong> shar<strong>in</strong>gideas. Time is <strong>the</strong> third element, i.e. <strong>the</strong> rate <strong>of</strong> spread <strong>of</strong> <strong>the</strong> <strong>in</strong>novation. Therelative time at which an <strong>in</strong>novation is diffused is based on adopter categories– how quickly <strong>the</strong> <strong>in</strong>dividual takes on <strong>the</strong> new idea. The fourth ma<strong>in</strong> element is<strong>the</strong> social system <strong>in</strong> which <strong>the</strong> <strong>in</strong>novation is embedded. F<strong>in</strong>d<strong>in</strong>gs from this<strong>the</strong>ory are particularly useful when shap<strong>in</strong>g questions such as why a particularhealth technology, or EPR, has not diffused more widely. Ano<strong>the</strong>r advantage<strong>of</strong> this approach is its firm root<strong>in</strong>g <strong>in</strong> <strong>the</strong> perspective <strong>of</strong> <strong>the</strong> user, and its centralfocus is on <strong>the</strong> utility <strong>of</strong> <strong>the</strong> <strong>in</strong>novation to <strong>the</strong> <strong>in</strong>dividual consumer. Build<strong>in</strong>g onthis approach, Greenhalgh et al, 79 developed a conceptual framework for <strong>the</strong>factors <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> diffusion and implementation <strong>of</strong> <strong>in</strong>novations. In thisframework, Greenhalgh et al 79 identified n<strong>in</strong>e <strong>in</strong>teract<strong>in</strong>g elements relat<strong>in</strong>g to,for example: attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation; characteristics <strong>of</strong> <strong>the</strong> adopter; systemread<strong>in</strong>ess for <strong>in</strong>novation; implementation process.4.2.2. Design for qualitative study elementsAs expla<strong>in</strong>ed <strong>in</strong> chapter 1, follow<strong>in</strong>g our orig<strong>in</strong>al research proposal,Department <strong>of</strong> Health policy shifted from locally-suplied to nationally-supplied<strong>IT</strong> applications. To accommodate this change, and to take <strong>in</strong>to accountcurrent levels <strong>of</strong> EPR implementation at <strong>the</strong> four study sites, <strong>the</strong> researchteam revised <strong>the</strong> orig<strong>in</strong>al study design.Basel<strong>in</strong>e <strong>in</strong>formation for each study site data was collected through meet<strong>in</strong>gswith key <strong>IT</strong>, f<strong>in</strong>ance and cl<strong>in</strong>ical directorate staff, as well as document review,and from rout<strong>in</strong>ely published data. Two levels <strong>of</strong> <strong>in</strong>terviews were conductedover three stages (see Appendices 1-9). Level 1 <strong>in</strong>terviews took place over43
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studytwo separate time <strong>in</strong>tervals (towards <strong>the</strong> beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> <strong>the</strong> project and eighteenmonths later):• Level 1 (stage A) <strong>in</strong>terviews took place between July and October 2004;• Level 1 (stage B) <strong>in</strong>terviews took place between February and April 2006;• Level 2 <strong>in</strong>terviews took place between January and October 2005.Level 1 research questions:-1. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> applications?2. How have recent Connect<strong>in</strong>g for Health policy changes impacted onimplementation processes?Level 2 research questions:-1. How are specific <strong>IT</strong> applications (CPOE and PACS), which have beenproposed by <strong>the</strong> new NPf<strong>IT</strong>, experienced by end-users (<strong>NHS</strong> staff)?2. How do <strong>the</strong>se new <strong>IT</strong> applications impact on work<strong>in</strong>g practices?Level 3 <strong>in</strong>terviews outl<strong>in</strong>ed <strong>in</strong> <strong>the</strong> orig<strong>in</strong>al proposal (how specific <strong>IT</strong>applications impact on patient care) were not conducted due to low levels <strong>of</strong>EPR function <strong>in</strong> our study sites.4.2.3. SampleThe study sample consists <strong>of</strong> four <strong>NHS</strong> Acute Trusts. Qualitative data werecollected over a two-year period ma<strong>in</strong>ly through semi-structured <strong>in</strong>terviewswith a range <strong>of</strong> stakeholders <strong>in</strong>volved <strong>in</strong> implement<strong>in</strong>g and us<strong>in</strong>g EPRs,<strong>in</strong>clud<strong>in</strong>g cl<strong>in</strong>icians (medical, nurs<strong>in</strong>g etc.) and managers at both junior andsenior levels (see Table 9).44
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyTable 9: Total number <strong>of</strong> <strong>in</strong>terviews conducted across <strong>the</strong> four study sitesNumber <strong>of</strong> participants Trust 1 Trust 2 Trust 3 Trust 4 TotalLevel 1Stage a 6 6 6 6 24Stage b 6 6 7 6 25Level 2e-book<strong>in</strong>g 0* 0 0 6 6PACS 0 7 3 7 17e-test order<strong>in</strong>g 10 11 0 0 21Total 22 30 16 25 93*Zero <strong>in</strong>dicates that <strong>the</strong> application was not implemented <strong>in</strong> <strong>the</strong> study siteLevel 1 <strong>in</strong>terviews were conducted with <strong>the</strong> follow<strong>in</strong>g personnel <strong>in</strong> eachparticipat<strong>in</strong>g Trust:Senior managers• Chief Executive• Director <strong>of</strong> IM & TMiddle managers• Project Manager (IM & T)• Cl<strong>in</strong>ical Director (Laboratory Medic<strong>in</strong>e or equivalent); this job title varied asstaff roles at this organisational level differ.Senior cl<strong>in</strong>icians and staff with a particular <strong>in</strong>terest/ role <strong>in</strong> EPRimplementation• Medical Director• Director <strong>of</strong> Nurs<strong>in</strong>g45
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyIn <strong>the</strong> 18 months between stages A and B <strong>the</strong>re were several changes <strong>in</strong>personnel; <strong>of</strong> <strong>the</strong> 23 staff orig<strong>in</strong>ally <strong>in</strong>terviewed <strong>in</strong> 2004, only 11 were still <strong>in</strong>post <strong>in</strong> 2006 (2 out <strong>of</strong> 4 chief executives, all 4 directors <strong>of</strong> nurs<strong>in</strong>g, 2 medicaldirectors and 3 directors <strong>of</strong> IM & T).Level 2 <strong>in</strong>terviews were conducted with <strong>NHS</strong> staff us<strong>in</strong>g <strong>the</strong> <strong>IT</strong> applicationsbe<strong>in</strong>g studied, as follows:• Project manager• EPR Tra<strong>in</strong>er• Three cl<strong>in</strong>icians (doctors, nurses, radiographers, pharmacists, orpathologists)• Allied health pr<strong>of</strong>essional• Adm<strong>in</strong>istrative/clerical staffTables 10 to 14 show <strong>the</strong> numbers <strong>of</strong> <strong>in</strong>terviews conducted across <strong>the</strong> fourstudy sites by staff occupation for <strong>the</strong> different stages <strong>of</strong> <strong>the</strong> project.For each stage <strong>of</strong> <strong>the</strong> analysis, Trust staff were ‘purposively’ recruited. For <strong>the</strong>level 1 <strong>in</strong>terviews, each role was matched as closely as possible acrossTrusts, i.e. <strong>the</strong> same set <strong>of</strong> questions be<strong>in</strong>g posed to <strong>the</strong> director <strong>of</strong> IM & T ateach Trust. To ga<strong>in</strong> an understand<strong>in</strong>g <strong>of</strong> how <strong>the</strong> contextual-organisationalfactors changed over time, each staff member hold<strong>in</strong>g that role was<strong>in</strong>terviewed twice, once <strong>in</strong> <strong>the</strong> early phases <strong>of</strong> implementation and aga<strong>in</strong>eighteen months later. For level 2 <strong>in</strong>terviews about end-users’ experiences,staff across Trusts were aga<strong>in</strong> matched as closely as possible; however, <strong>the</strong>primary consideration was recruit<strong>in</strong>g staff with user-knowledge <strong>of</strong> <strong>the</strong> <strong>IT</strong>application be<strong>in</strong>g evaluated. Because some electronic applications were notimplemented <strong>in</strong> any <strong>of</strong> our study sites across <strong>the</strong> study time frame, <strong>the</strong> number<strong>of</strong> participants recruited was lower than expected. This was particularly <strong>the</strong>case for electronic book<strong>in</strong>g, which was timetabled to have been fullyimplemented <strong>in</strong> all acute trusts <strong>in</strong> England by 2005. However, at <strong>the</strong> time <strong>of</strong>this fieldwork, <strong>the</strong> roll out <strong>of</strong> this service was runn<strong>in</strong>g a year beh<strong>in</strong>d schedule,which meant that front-l<strong>in</strong>e staff us<strong>in</strong>g this application were not available.46
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study4.2.4. Procedure<strong>NHS</strong> staff were recruited by <strong>the</strong> researcher, who directly approached <strong>the</strong>relevant person. Each potential participant was given an <strong>in</strong>formation sheetabout <strong>the</strong> study, which described what participation <strong>in</strong>volved. The researcheralso expla<strong>in</strong>ed <strong>the</strong> study <strong>in</strong> person and <strong>in</strong>vited <strong>the</strong> person to take part. To helpwith recruitment, <strong>the</strong> researcher sent a global e-mail to hospital staff (outl<strong>in</strong><strong>in</strong>g<strong>the</strong> study and what participation <strong>in</strong>volved) and presented an <strong>in</strong>formal overview<strong>of</strong> <strong>the</strong> study at a medical committee meet<strong>in</strong>g <strong>of</strong> each Trust. Written <strong>in</strong>formedconsent to be <strong>in</strong>terviewed was obta<strong>in</strong>ed <strong>in</strong> every case. The <strong>in</strong>terviews weresemi-structured, and conducted on a one-to-one basis at each Trust by aqualitative researcher (JH). The <strong>in</strong>terview was conducted at <strong>the</strong> hospital at atime convenient to <strong>the</strong> participant, and lasted about an hour. Interviews weretaped and transcribed. Participants were guaranteed that both <strong>the</strong>y and <strong>the</strong>irorganisation would be anonymised.Table 10: Level 1 stage ANumber <strong>of</strong> participants Trust 1 Trust 2 Trust 3 Trust 4 TotalSenior managers 2 2 2 2 8Middle managers 2 2 2 2 8Senior Cl<strong>in</strong>icians 2 2 2 2 8Senior Cl<strong>in</strong>icians 2 2 2 2 8Table 11: Level 1 stage BNumber <strong>of</strong> participants Trust 1 Trust 2 Trust 3 Trust 4 TotalSenior managers 2 2 2 2 8Middle managers 2 2 2 2 8Senior Cl<strong>in</strong>icians 2 2 2 2 8Senior Cl<strong>in</strong>icians 3 2 2 2 947
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyTable 12: Level 2 e-book<strong>in</strong>gChiefexecutiveProjectmanagerCl<strong>in</strong>icaldirectorEPR tra<strong>in</strong>erAdm<strong>in</strong>istrativestaffTrust 4 1 1 1 1 2Table 13: Level 2 – Picture Archiv<strong>in</strong>g and Communication SystemNumber <strong>of</strong> participants Trust 1 Trust 2 Trust 3 Trust 4 TotalProject manager 0 1 1 1 3EPR tra<strong>in</strong>er 0 1 0 1 2Cl<strong>in</strong>icians 0 3 2 3 8AHPs 0 1 0 1 2Adm<strong>in</strong>istrative staff 0 1 0 1 2Table 14: Level 2 – e-Test Order<strong>in</strong>g and Brows<strong>in</strong>gNumber <strong>of</strong> participants Trust 1 Trust 2 Trust 3 Trust 4 TotalProject manager 1 2 0 0 2EPR tra<strong>in</strong>er 1 1 0 0 2Cl<strong>in</strong>icians 7 6 0 0 1AHPs 1 0 0 0 1Adm<strong>in</strong>istrative staff 1 1 0 0 14.2.5. Topics addressedFor <strong>the</strong> Level 1 <strong>in</strong>terviews (stages A and B), we developed a set <strong>of</strong> corequestions applicable across all <strong>the</strong> trusts (see <strong>in</strong>terview schedule,Appendices 1 and 2). This generic approach allowed <strong>the</strong> researchers to ga<strong>in</strong>a detailed overview <strong>of</strong> different factors <strong>in</strong>fluential to understand<strong>in</strong>g why EPR<strong>in</strong>novation may have been difficult to achieve <strong>in</strong> <strong>the</strong> past, and to identifyprecursors for future implementation success. The follow<strong>in</strong>g are examples <strong>of</strong><strong>the</strong> contextual factors explored:48
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study• Organisational structure: <strong>the</strong> physical, <strong>in</strong>formational and organisationalresources (costs) that facilitate or h<strong>in</strong>der <strong>IT</strong> use.• Project management and stag<strong>in</strong>g: The perception <strong>of</strong> clear, reasonablegoals, staff consultation and good plann<strong>in</strong>g, <strong>in</strong> particular perceptions <strong>of</strong>change management associated with prepar<strong>in</strong>g for <strong>the</strong> national solutions.• Organisational commitment to implementation: The role <strong>of</strong> constantchange <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally and exploration <strong>of</strong>whe<strong>the</strong>r this change has impacted on <strong>IT</strong> focus and staff commitment(seem<strong>in</strong>gly exacerbated by <strong>the</strong> LSP appear<strong>in</strong>g to poach <strong>NHS</strong> <strong>IT</strong> staff).• Organisational ‘fit’ and <strong>the</strong> question <strong>of</strong> differ<strong>in</strong>g agendas, issues such as<strong>the</strong> perceptions <strong>of</strong> priorities and EPR implementation meet<strong>in</strong>g <strong>the</strong> needs <strong>of</strong>‘everyman’, i.e. <strong>the</strong> acute Trust, <strong>the</strong> SHA, and <strong>the</strong> NPf<strong>IT</strong>; <strong>the</strong> role <strong>of</strong> <strong>in</strong>house<strong>IT</strong> <strong>in</strong>novations and <strong>the</strong>ir future, <strong>in</strong>clud<strong>in</strong>g any proposal to substitutestand-alone systems with standard, perhaps less immediately functional,LSP solutions.• Conceptions <strong>of</strong> what constitutes EPR implementation success or failure:questions such as <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success, at what level, and for whom,i.e. <strong>the</strong> Trust, <strong>the</strong> LSP or <strong>the</strong> NPf<strong>IT</strong>.• The current relationship between Trust Managers and <strong>the</strong> <strong>in</strong>formationsystem <strong>in</strong> use.• The impact <strong>of</strong> <strong>the</strong> <strong>IT</strong> <strong>in</strong>novation on <strong>the</strong> relationship between TrustManagers and o<strong>the</strong>r employees.• Cultural/ social /organisational identity issues: past and currentexperiences and values, and <strong>the</strong> residual impact <strong>of</strong> previousimplementations (e.g. previous <strong>in</strong>-house <strong>IT</strong> failures), and specific medical/legal/ staff<strong>in</strong>g problems.• Perceptions <strong>of</strong> what <strong>the</strong> NPf<strong>IT</strong> should deliver, compared to what iscurrently perceived as be<strong>in</strong>g rolled out: explor<strong>in</strong>g any organisational dividebetween mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and <strong>the</strong> deliverables.• The role <strong>of</strong> leaders and super-users: <strong>the</strong> organisational impact <strong>of</strong> keyplayers.49
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study• Individual differences and categorisation <strong>of</strong> <strong>the</strong> person: levels <strong>of</strong>motivation, efficacy, <strong>in</strong>volvement; <strong>the</strong> organisational impact <strong>of</strong> personal<strong>in</strong>vestment (or lack <strong>of</strong> it).For <strong>the</strong> level 2 <strong>in</strong>terviews, sample-specific questions were developed tocapture organisational change <strong>in</strong> areas where implementation <strong>of</strong> specific <strong>IT</strong>applications has occurred, or is <strong>in</strong> <strong>the</strong> process or occurr<strong>in</strong>g (see <strong>in</strong>terviewschedules, Appendices 3 to 9).Us<strong>in</strong>g purposive sampl<strong>in</strong>g, staff wi<strong>the</strong>xperience <strong>of</strong> us<strong>in</strong>g particular <strong>IT</strong> applications were recruited, i.e.Radiographers at Trust 4 us<strong>in</strong>g PACS (digital filmless radiology). Because <strong>the</strong>second level analysis was concerned with end-users’ experiences (<strong>the</strong>process and impact <strong>of</strong> implementation) questions focused on:• Knowledge <strong>of</strong> <strong>the</strong> <strong>IT</strong> application – tra<strong>in</strong><strong>in</strong>g, support and <strong>in</strong>formation given.• Technical capabilities - attributes such as <strong>the</strong> functionality, compatibility,complexity, ‘userability’, speed, and ‘trialability’ <strong>of</strong> <strong>the</strong> <strong>IT</strong> application.• Nature <strong>of</strong> <strong>the</strong> change <strong>in</strong> behaviour – how easy or difficult was it tolearn/do? Changes <strong>in</strong> cognitive process<strong>in</strong>g – how <strong>the</strong>y need to th<strong>in</strong>k?• The relationship between electronic and paper records. Perceivedadvantages and disadvantages <strong>of</strong> each - regard<strong>in</strong>g <strong>the</strong> availability,<strong>in</strong>tegrity, completeness, and compliance with best practice.• Changes <strong>in</strong> work<strong>in</strong>g practices. Issues such as changes <strong>in</strong> communicationpatterns, decision-mak<strong>in</strong>g, and role. Did <strong>the</strong> <strong>IT</strong> application impact on <strong>the</strong>cl<strong>in</strong>ician-to-cl<strong>in</strong>ician relationship, cl<strong>in</strong>ician-to-managers relationship, andcl<strong>in</strong>ician-to-patient relationship.• The process <strong>of</strong> shar<strong>in</strong>g ideas and learn<strong>in</strong>g <strong>the</strong> <strong>IT</strong> application – useracceptance, satisfaction and organisation <strong>of</strong> work.• Users’ organisational expectations <strong>of</strong> <strong>the</strong> <strong>IT</strong> application versus <strong>the</strong> currentreality.o Individual differences - categorisation <strong>of</strong> <strong>the</strong> person – how motivated,efficacious, and <strong>in</strong>volved are <strong>the</strong>y. For example, certa<strong>in</strong> groups <strong>of</strong>cl<strong>in</strong>icians may resist changes <strong>in</strong> work<strong>in</strong>g patterns – not want<strong>in</strong>g to moveaway from standalone/exist<strong>in</strong>g systems to more standardised LSPsolutions.50
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studyo The perceived impact <strong>of</strong> <strong>the</strong> <strong>IT</strong> application and changes to it from NPf<strong>IT</strong>on future work<strong>in</strong>g practices, cl<strong>in</strong>ical management and <strong>in</strong>dividual patientcare. How can <strong>the</strong> positive effects <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications bemaximised? What are staff perceptions <strong>of</strong> <strong>the</strong> best way forward?4.2.6. AnalysisQualitative data from <strong>in</strong>terviews and observations <strong>of</strong> meet<strong>in</strong>gs were analysed<strong>in</strong> accordance with <strong>the</strong> prelim<strong>in</strong>ary framework outl<strong>in</strong>ed above, with <strong>the</strong> analysisdivided <strong>in</strong>to two levels (organisational context and staff experiences). The aim<strong>of</strong> this division was to unpack <strong>the</strong> impact and processes <strong>of</strong> EPRimplementation associated with each level. However, we also needed topresent <strong>the</strong> ‘messy’ reality <strong>of</strong> association and causation that exists between<strong>the</strong> organisation, <strong>the</strong> <strong>IT</strong>, <strong>the</strong> EPR user and <strong>the</strong> patient. In reach<strong>in</strong>g conclusionsand untangl<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> <strong>the</strong> structure <strong>of</strong> a system, from <strong>the</strong> effects <strong>of</strong><strong>in</strong>dividuals that make up that system and use it, we applied a modifiedgrounded <strong>the</strong>ory analytic strategy, 80 which comb<strong>in</strong>ed draw<strong>in</strong>g on <strong>the</strong> literatureon organisational change, and more user-centred sociological <strong>the</strong>ories <strong>of</strong><strong>in</strong>novation adoption and implementation, with <strong>the</strong>mes emerg<strong>in</strong>g from <strong>the</strong> data,to present an analysis <strong>of</strong> processes over time.Accord<strong>in</strong>g to grounded <strong>the</strong>ory pr<strong>in</strong>ciples, <strong>the</strong> analytic strategy <strong>in</strong>volvedanalys<strong>in</strong>g <strong>the</strong> data at three separate time po<strong>in</strong>ts, with different levels <strong>of</strong>analysis and types <strong>of</strong> process applied to each stage. This separation alloweddevelop<strong>in</strong>g categories to emerge <strong>in</strong> <strong>the</strong> first batch <strong>of</strong> texts, <strong>the</strong>se ideas to befur<strong>the</strong>r compared, contrasted and developed <strong>in</strong> <strong>the</strong> second batch <strong>of</strong> texts, and<strong>the</strong> emerg<strong>in</strong>g <strong>the</strong>ory to be tested aga<strong>in</strong>st <strong>the</strong> data collected <strong>in</strong> <strong>the</strong> third batch.The f<strong>in</strong>al <strong>the</strong>mes reported were fur<strong>the</strong>r verified by ano<strong>the</strong>r member <strong>of</strong> <strong>the</strong> team(NF) <strong>in</strong>dependently read<strong>in</strong>g <strong>the</strong> transcripts, <strong>the</strong>n <strong>the</strong> two team memberswork<strong>in</strong>g toge<strong>the</strong>r (JH & NF) to agree f<strong>in</strong>al mean<strong>in</strong>gs.Ano<strong>the</strong>r requirement was to use a qualitative method that was complementaryto <strong>the</strong> epistemological position <strong>of</strong> a multi-methods project. Few appliedresearchers would disagree that <strong>the</strong> question must be “which methodologicalapproach is most suited to <strong>the</strong> research question or problem at hand” 81(p.115). In apply<strong>in</strong>g Grounded Theory techniques <strong>the</strong>re is “no fundamental51
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studyclash” between <strong>the</strong> purposes and capacities <strong>of</strong> qualitative and quantitativemethods or data. 82There is <strong>the</strong> belief that different methodologies pitched atdifferent levels <strong>of</strong> analysis and types <strong>of</strong> research question, can uniquelycontribute to measur<strong>in</strong>g different facets <strong>of</strong> a given question. Each method isconsidered useful <strong>in</strong> <strong>the</strong> verification and generation <strong>of</strong> <strong>the</strong>ory, with <strong>the</strong> ma<strong>in</strong>po<strong>in</strong>t <strong>of</strong> emphasis be<strong>in</strong>g <strong>the</strong> cont<strong>in</strong>ued generation <strong>of</strong> ideas and knowledge.4.3. Methods for <strong>the</strong> quantitative study4.3.1. Study designOur study used a quasi-experimental controlled design, i.e. a “controlled prepost‘cohort’ design”, 83 also <strong>of</strong>ten called a “controlled before-and-after” design.The pr<strong>in</strong>ciple <strong>of</strong> <strong>the</strong> design is described <strong>in</strong> detail below. We tested for effects<strong>of</strong> implement<strong>in</strong>g CPOE and PACS by mak<strong>in</strong>g comparisons between Trusts(<strong>the</strong> control group comprised those Trusts <strong>in</strong> which CPOE or PACS had notbeen implemented), and by mak<strong>in</strong>g comparisons with<strong>in</strong> Trusts (<strong>the</strong> controlgroup comprised those specialties <strong>in</strong> which CPOE or PACS had not beenimplemented).4.3.2. OutcomesThe outcomes used <strong>in</strong> our study are summarized <strong>in</strong> Tables 15a and 15b.These outcomes evolved from a larger set <strong>of</strong> <strong>in</strong>dicators which had beendef<strong>in</strong>ed a priori, based partly on consideration <strong>of</strong> <strong>the</strong> <strong>NHS</strong> Efficiency Map. 54Our study outcomes evolved dur<strong>in</strong>g data collection and analysis, as it becameapparent which would meet <strong>the</strong> criteria <strong>of</strong> feasibility (data availability),reliability (data quality), and comparability (between and with<strong>in</strong> Trusts, andwith studies <strong>in</strong> o<strong>the</strong>r sett<strong>in</strong>gs). The outcomes also had to be mean<strong>in</strong>gful, <strong>in</strong>terms <strong>of</strong> <strong>in</strong>terpret<strong>in</strong>g <strong>the</strong> effects <strong>of</strong> implement<strong>in</strong>g CPOE and PACS.We classified outcomes as primary or secondary based ma<strong>in</strong>ly on aconsideration <strong>of</strong> <strong>the</strong> causal pathway between implementation <strong>of</strong> an <strong>IT</strong> systemand <strong>the</strong> outcome. Hence, an <strong>IT</strong> system which facilitates cl<strong>in</strong>icians’ access toprevious pathology test results or radiological images, and which also reduces<strong>the</strong> likelihood <strong>of</strong> results or images be<strong>in</strong>g lost, might be expected to have a52
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studydirect impact on primary outcomes such as <strong>the</strong> number <strong>of</strong> tests ordered orexams requested per <strong>in</strong>patient day or per outpatient appo<strong>in</strong>tment, and <strong>the</strong><strong>in</strong>terval between repeat tests or exams. Secondary outcomes such as<strong>in</strong>patient length-<strong>of</strong>-stay, emergency re-admission follow<strong>in</strong>g <strong>in</strong>patient stay, ornon-attendance at outpatient appo<strong>in</strong>tments, might be <strong>in</strong>directly affected byimprovements <strong>in</strong> pathology and radiology <strong>IT</strong> systems, but would also be<strong>in</strong>fluenced by operational changes with<strong>in</strong> <strong>the</strong> hospital unrelated toimplementation <strong>of</strong> <strong>the</strong>se systems.comparative analyses be<strong>in</strong>g carried out.All outcomes were def<strong>in</strong>ed prior toFor <strong>the</strong> CPOE analysis, we considered three types <strong>of</strong> pathology test: full bloodcount (FBC), urea and electrolytes (UE), and ur<strong>in</strong>e culture (UC). For <strong>the</strong> PACSanalysis, we considered three types <strong>of</strong> radiological exam<strong>in</strong>ation: pla<strong>in</strong> film(PF), computed tomography (CT), and ultrasound (US).4.3.3. Data sourcesInpatient and outpatient data were obta<strong>in</strong>ed from IM&T departments <strong>in</strong> eachTrust. These data were a subset <strong>of</strong> <strong>the</strong> Commission<strong>in</strong>g Data Set (CDS) whicheach Trust sends on a regular basis to <strong>the</strong> <strong>NHS</strong>-wide Clear<strong>in</strong>g Service(NWCS), from which Hospital Episode Statistics (HES) and o<strong>the</strong>r statistics aregenerated for <strong>the</strong> Department <strong>of</strong> Health (DoH). We used <strong>the</strong> <strong>NHS</strong> DataDictionary to identify variables relevant to our study (Appendix 10), and <strong>the</strong>data were extracted by IM&T staff from <strong>the</strong>ir archives. 84 Pathology andradiology data were obta<strong>in</strong>ed from <strong>the</strong> pathology and radiology departments <strong>in</strong>each Trust. All <strong>of</strong> <strong>the</strong>se departments ma<strong>in</strong>ta<strong>in</strong>ed electronic records from whichdata for <strong>the</strong> study period could be extracted. In two <strong>in</strong>stances (Trust 2pathology and Trust 3 radiology), data were extracted under a contractualarrangement with <strong>the</strong> commercial provider <strong>of</strong> <strong>the</strong> radiology/pathology system.53
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyTable 15a: Primary study outcomes: derivation and <strong>in</strong>terpretationPrimary outcome Derivation Analysis(measure <strong>of</strong> effect) 1Interpretation <strong>of</strong> resultInpatientTests per <strong>in</strong>patient (nonzerovs zero response)Likelihood <strong>of</strong> an <strong>in</strong>patient hav<strong>in</strong>g one or moretests/exams ordered/requested.Logistic regression(odds ratio, OR)OR
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyTable 15b: Secondary study outcomes: derivation and <strong>in</strong>terpretationSecondary outcome Derivation Analysis(measure <strong>of</strong> effect) 1Interpretation <strong>of</strong> resultInpatientLength-<strong>of</strong>-stay (exclud<strong>in</strong>gday cases)(Hospital provider spell end date - hospital providerspell start date) for all <strong>in</strong>patients.Cox regression(hazard ratio, HR)HR>1 <strong>in</strong>dicates shorter <strong>in</strong>patientlength-<strong>of</strong>-stay (i.e. greaterlikelihood <strong>of</strong> be<strong>in</strong>g discharged)Inpatient treated as a daycase (i.e. zero length <strong>of</strong>stay)Likelihood <strong>of</strong> an <strong>in</strong>patient be<strong>in</strong>g discharged on <strong>the</strong> day<strong>of</strong> admission.Logistic regression(odds ratio, OR)OR>1 <strong>in</strong>dicates <strong>in</strong>crease <strong>in</strong> daycase admissionsIntended day case patientadmitted overnightLikelihood <strong>of</strong> an <strong>in</strong>tended day case (i.e. <strong>in</strong>tendedmanagement = “day case”) be<strong>in</strong>g admitted overnight.Logistic regression(odds ratio, OR)OR
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study4.3.4. Data analysisEach patient who received care from a Trust was rout<strong>in</strong>ely allocated a ‘localpatient identifier’ which was unique with<strong>in</strong> that Trust. This patient identifiertypically comprised a six or seven digit number, preceded or followed by oneor two characters correspond<strong>in</strong>g to a hospital with<strong>in</strong> <strong>the</strong> Trust. The <strong>in</strong>patientand outpatient datasets comprised one row for each episode <strong>of</strong> admittedpatient care or outpatient appo<strong>in</strong>tment. The radiology and pathology datasetscomprised one row for each test or exam. All datasets conta<strong>in</strong>ed <strong>the</strong> localpatient identifier, which we used to jo<strong>in</strong> <strong>the</strong> <strong>in</strong>patient and outpatient datasetswith <strong>the</strong> pathology and radiology datasets, and so derive <strong>the</strong> primaryoutcomes. Secondary outcomes were derived directly from <strong>the</strong><strong>in</strong>patient/outpatient data. All analyses were performed us<strong>in</strong>g Stata v9(StataCorp. 2003. Stata Statistical S<strong>of</strong>tware: Release 9. College Station, TX,USA).Between-Trust comparisonsThe effect <strong>of</strong> an <strong>IT</strong> system on an outcome could be detected by compar<strong>in</strong>gtrends <strong>in</strong> that outcome <strong>in</strong> a Trust <strong>in</strong> which a new system had beenimplemented (<strong>the</strong> ‘<strong>in</strong>tervention’ Trust) with trends <strong>in</strong> <strong>the</strong> outcome <strong>in</strong> Trusts <strong>in</strong>which no new system had been implemented (<strong>the</strong> ‘control’ Trusts). Modelswere based on time periods correspond<strong>in</strong>g to <strong>the</strong> periods before, dur<strong>in</strong>g, andafter implementation <strong>of</strong> <strong>the</strong> <strong>IT</strong> system.For primary outcomes, separate models were required for pathology andradiology systems. In each <strong>of</strong> <strong>the</strong>se models, <strong>the</strong> effect <strong>of</strong> <strong>the</strong> new <strong>IT</strong> system isestimated by <strong>the</strong> regression model term for <strong>the</strong> <strong>in</strong>teraction between <strong>the</strong><strong>in</strong>tervention Trust and time period, specifically by <strong>the</strong> <strong>in</strong>teraction parametercorrespond<strong>in</strong>g to <strong>the</strong> post-<strong>in</strong>tervention period. The basel<strong>in</strong>e <strong>in</strong> this model is <strong>the</strong>outcome <strong>in</strong> ‘control’ Trusts dur<strong>in</strong>g <strong>the</strong> pre-<strong>in</strong>tervention period. The model alsogenerates a parameter which estimates <strong>the</strong> change <strong>in</strong> <strong>the</strong> outcome compar<strong>in</strong>g<strong>the</strong> post- and pre-<strong>in</strong>tervention periods <strong>in</strong> <strong>the</strong> ‘control’ Trusts. This parameter56
Report to SDO for NCRS ProjectMethods <strong>of</strong> Studyprovides a context <strong>in</strong> which to assess <strong>the</strong> magnitude and direction <strong>of</strong> <strong>the</strong>change <strong>in</strong> <strong>the</strong> outcome attributable to <strong>the</strong> <strong>in</strong>tervention.For secondary outcomes, a s<strong>in</strong>gle model with two such <strong>in</strong>teraction terms wasused; one <strong>in</strong>teraction term estimated <strong>the</strong> effect <strong>of</strong> <strong>the</strong> new CPOE system (<strong>in</strong>Trust 1), <strong>the</strong> o<strong>the</strong>r estimates <strong>the</strong> effect <strong>of</strong> <strong>the</strong> new PACS system (<strong>in</strong> Trust 4).The time periods for implementation <strong>of</strong> CPOE and PACS <strong>in</strong> Trusts 1 and 4respectively were, co<strong>in</strong>cidentally, approximately <strong>the</strong> same (see Tables 3 to 5).The time period dur<strong>in</strong>g which <strong>the</strong> systems were implemented was reta<strong>in</strong>ed <strong>in</strong><strong>the</strong> model but is not reported.Between-Trust comparisons were controlled for case-mix differences betweenTrusts by <strong>in</strong>clud<strong>in</strong>g cl<strong>in</strong>ical specialty (CDS data element ‘treatment function’)as a categorical variable <strong>in</strong> <strong>the</strong> models, and by restrict<strong>in</strong>g our analyses to <strong>the</strong>ma<strong>in</strong> specialties common to all Trusts. Common <strong>in</strong>patient specialties weregeneral surgery, general medic<strong>in</strong>e, urology, trauma & orthopaedics, accident& emergency, paediatrics, obstetrics & gynaecology. Common outpatientspecialties were all <strong>of</strong> <strong>the</strong> above plus ENT, ophthalmology, endocr<strong>in</strong>ology,haematology, cardiology, dermatology, nephrology, oncology, neurology,rheumatology, and geriatric medic<strong>in</strong>e.Effects on b<strong>in</strong>ary outcomes were assessed us<strong>in</strong>g logistic regression, andeffects on cont<strong>in</strong>uous outcomes by ord<strong>in</strong>ary least squares l<strong>in</strong>ear regression,with a natural logarithmic transformation to obta<strong>in</strong> a near-normal distribution.Cont<strong>in</strong>uous outcomes with a high proportion <strong>of</strong> zero values, e.g. test/examsper <strong>in</strong>patient day, were analysed us<strong>in</strong>g logistic regression to model <strong>the</strong>probability <strong>of</strong> a zero response, and l<strong>in</strong>ear regression to model <strong>the</strong> non-zerocont<strong>in</strong>uous response. 85Effects on length-<strong>of</strong>-stay and time-to-death wereassessed by Cox regression, after check<strong>in</strong>g <strong>the</strong> proportional hazardsassumption. We analysed each type <strong>of</strong> pathology test and each type <strong>of</strong>radiological exam separately. Ultrasound was not an element <strong>of</strong> <strong>the</strong> PACS <strong>in</strong>Trust 4, but data on ultrasound exam<strong>in</strong>ations were analysed by way <strong>of</strong>comparison with trends <strong>in</strong> PF and CT exam<strong>in</strong>ations. Robust standard errorswere calculated to take <strong>in</strong>to account cluster<strong>in</strong>g <strong>of</strong> observations by Trust and bycl<strong>in</strong>ical specialty.57
Report to SDO for NCRS ProjectMethods <strong>of</strong> StudyWith<strong>in</strong>-Trust comparisonsThe effect <strong>of</strong> an <strong>IT</strong> system on an outcome could also be detected bycompar<strong>in</strong>g trends <strong>in</strong> that outcome with<strong>in</strong> a Trust <strong>in</strong> specialties which hadadopted a new system (<strong>the</strong> ‘<strong>in</strong>tervention’ specialties) with trends <strong>in</strong> <strong>the</strong>outcome <strong>in</strong> specialties which had not adopted <strong>the</strong> new system (<strong>the</strong> ‘control’specialties). Models were based on time periods correspond<strong>in</strong>g to <strong>the</strong> periodsbefore and after implementation <strong>of</strong> <strong>the</strong> <strong>IT</strong> system.The effect <strong>of</strong> <strong>the</strong> new <strong>IT</strong> system is isolated <strong>in</strong> <strong>the</strong> regression model term for<strong>in</strong>teraction between <strong>the</strong> <strong>in</strong>tervention specialties and time period. The basel<strong>in</strong>e<strong>in</strong> this model is <strong>the</strong> outcome <strong>in</strong> ‘control’ specialties dur<strong>in</strong>g <strong>the</strong> pre-<strong>in</strong>terventionperiod. As with Between-Trust comparisons, logistic regression was used forb<strong>in</strong>ary outcomes, l<strong>in</strong>ear regression for cont<strong>in</strong>uous outcomes, and acomb<strong>in</strong>ation <strong>of</strong> logistic and l<strong>in</strong>ear regression for zero-<strong>in</strong>flated cont<strong>in</strong>uousoutcomes.The follow<strong>in</strong>g with<strong>in</strong>-Trust comparisons were performed: for CPOE with<strong>in</strong> Trust1, a comparison <strong>of</strong> obstetrics with all o<strong>the</strong>r specialties; for PACS with<strong>in</strong> Trust4, a comparison <strong>of</strong> trauma and orthopaedics with all o<strong>the</strong>r specialties. In Trust1, CPOE was never implemented <strong>in</strong> obstetrics, hence this specialty serves asa constant control. With<strong>in</strong> Trust 4, PACS was implemented first <strong>in</strong> trauma andorthopaedics, and <strong>the</strong>n <strong>in</strong> all o<strong>the</strong>r specialties (see Table 16). For <strong>the</strong> purpose<strong>of</strong> our analyses, six time periods were def<strong>in</strong>ed correspond<strong>in</strong>g to <strong>the</strong> <strong>in</strong>tervals:before implementation <strong>of</strong> PACS (period#1 01/2000-05/2001), dur<strong>in</strong>gimplementation <strong>of</strong> PACS <strong>in</strong> A&E and orthopaedics, split <strong>in</strong>to two periods(period#2 06/2001-11/2001 and period#3 12/2001-05/2002), dur<strong>in</strong>gimplementation <strong>of</strong> PACS <strong>in</strong> all o<strong>the</strong>r specialties, also split <strong>in</strong>to two periods(period#4 06/2002-10/2002 and period#5 11/2002-03/2003), and after Trustwideimplementation <strong>of</strong> PACS (period#6 04/2003-12/2005). We comparedoutcomes <strong>in</strong> A&E and orthopaedics before and after implementation <strong>of</strong> PACS,adjusted for <strong>the</strong> underly<strong>in</strong>g trend <strong>in</strong> <strong>the</strong> same outcomes <strong>in</strong> all o<strong>the</strong>r specialties,us<strong>in</strong>g period#1 and period#2 comb<strong>in</strong>ed as <strong>the</strong> pre-<strong>in</strong>tervention period (noPACS) and period#3 and period#4 comb<strong>in</strong>ed as <strong>the</strong> post-<strong>in</strong>tervention period58
Report to SDO for NCRS ProjectMethods <strong>of</strong> Study(PACS <strong>in</strong> A&E and orthopaedics, no PACS <strong>in</strong> any o<strong>the</strong>r specialties). We <strong>the</strong>ncompared outcomes <strong>in</strong> all o<strong>the</strong>r specialties before and after implementation <strong>of</strong>PACS, adjusted for <strong>the</strong> underly<strong>in</strong>g trend <strong>in</strong> <strong>the</strong> same outcomes <strong>in</strong> A&E andorthopaedics, us<strong>in</strong>g period#3 and period#4 comb<strong>in</strong>ed as <strong>the</strong> pre-<strong>in</strong>terventionperiod (PACS <strong>in</strong> A&E and orthopaedics, but no PACS <strong>in</strong> any o<strong>the</strong>r specialties)and period#5 and period#6 comb<strong>in</strong>ed as <strong>the</strong> post-<strong>in</strong>tervention period (PACS <strong>in</strong>all specialties). Standard errors were adjusted for cluster<strong>in</strong>g by cl<strong>in</strong>icalspecialty.Table 16: PACS with<strong>in</strong>-Trust 4 comparison periods.PeriodStartdateEnddatePACS <strong>in</strong> A&E +orthopaedicsPACS <strong>in</strong> o<strong>the</strong>rspecialties“1 st PACS”comparison“2 nd PACS”comparison1 04/2000 05/20012 06/2001 11/1001PreimplementationDur<strong>in</strong>gPreimplementationNo PACS <strong>in</strong>any specialtyData not used3 12/2001 05/2002implementationPACS <strong>in</strong> A&EPACS <strong>in</strong> A&E4 06/2002 10/20025 11/2002 03/20036 04/2003 12/2005PostimplementationDur<strong>in</strong>gimplementationPostimplementation+orthopaedicsData not used+orthopaedicsPACS <strong>in</strong> allspecialties59
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 15. Qualitative f<strong>in</strong>d<strong>in</strong>gs from Level 1: Implementation <strong>of</strong> NPf<strong>IT</strong> at local levelThis chapter presents f<strong>in</strong>d<strong>in</strong>gs from both stages <strong>of</strong> ‘level 1’ i.e. our study <strong>of</strong> <strong>the</strong>implementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> <strong>in</strong> four trusts over a two year period. Stage A,consist<strong>in</strong>g <strong>of</strong> 24 <strong>in</strong>terviews, took place between July and October 2004. Stage B,consist<strong>in</strong>g <strong>of</strong> 25 <strong>in</strong>terviews, took place between February and April 2006. Thesef<strong>in</strong>d<strong>in</strong>gs have been published or are about to be published 86 ,87 and this chapterdraws heavily on <strong>the</strong>se papers.5.1. Stage a.: resultsTable 17 shows <strong>the</strong> basel<strong>in</strong>e characteristics <strong>of</strong> each trust and <strong>the</strong> expected datefor replac<strong>in</strong>g <strong>the</strong>se with <strong>the</strong> NCRS/NPf<strong>IT</strong>. Data from <strong>the</strong> first round <strong>of</strong> <strong>in</strong>terviewsshow <strong>the</strong> potential impact <strong>of</strong> <strong>the</strong> factors that emerged on implement<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong>.Table 17: Trust characteristicsTrustCharacteristic 1 2 3 4Size Large Large Large SmallNumber <strong>of</strong>ma<strong>in</strong> sites2[earlier merger]2[earlier merger]1 1F<strong>in</strong>ancialsituation aModeratedeficit
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 15.1.1. Multiple sites with<strong>in</strong> trustsTwo <strong>of</strong> <strong>the</strong> trusts have multiple sites, result<strong>in</strong>g from recent mergers, andproblems <strong>of</strong> poor communication and coord<strong>in</strong>ation between sites rema<strong>in</strong>.Differences <strong>in</strong> work<strong>in</strong>g practices and organisational culture seem to havecreated tensions that may make <strong>the</strong> job <strong>of</strong> gett<strong>in</strong>g ready for <strong>the</strong> <strong>NHS</strong> carerecord service especially challeng<strong>in</strong>g (see box 1). Major changes result<strong>in</strong>gfrom <strong>the</strong> recent mergers seem to have affected staff morale, <strong>in</strong>creas<strong>in</strong>g <strong>the</strong>likelihood that staff will become resistant to <strong>the</strong> changes required dur<strong>in</strong>gimplementation.Box 1: Issues <strong>of</strong> multiple Trust sites and change overload“There’s <strong>the</strong> difference <strong>in</strong> cultures between <strong>the</strong> two ends <strong>of</strong> <strong>the</strong> same Trust, <strong>the</strong>culture where <strong>the</strong> whole senior management team transported <strong>the</strong>mselves over. Andso I th<strong>in</strong>k at one end with<strong>in</strong> <strong>the</strong> Trust, <strong>the</strong> [name] end, <strong>the</strong> cl<strong>in</strong>icians and <strong>the</strong> nursesand o<strong>the</strong>rs are all used to a different way <strong>of</strong> work<strong>in</strong>g, which <strong>the</strong> people here are not.So I th<strong>in</strong>k <strong>the</strong>re is a big difference actually between—if you ask people at that end Ith<strong>in</strong>k you’ll f<strong>in</strong>d a very different philosophy <strong>the</strong>re.”—Cl<strong>in</strong>ical director, Trust 2“One <strong>of</strong> <strong>the</strong> th<strong>in</strong>gs that def<strong>in</strong>itely makes life much easier is that we’re a s<strong>in</strong>gle siteorganisation, so <strong>the</strong>re is a s<strong>in</strong>gle culture around this place; we’re not a difficultpolitical be<strong>in</strong>g with eight or n<strong>in</strong>e hospital sites spread around. From an <strong>IT</strong> po<strong>in</strong>t <strong>of</strong>view that’s very difficult to support and manage.”—<strong>IT</strong> manager, Trust 4“So, like I said, I th<strong>in</strong>k <strong>the</strong> organisation, leav<strong>in</strong>g aside <strong>the</strong> <strong>IT</strong>, has quite a few issuesstill <strong>in</strong> terms <strong>of</strong> <strong>the</strong> changes it’s gone through. Then add <strong>in</strong> <strong>the</strong> national programmeand that’s just, just ano<strong>the</strong>r th<strong>in</strong>g on top, and that’s go<strong>in</strong>g to affect work<strong>in</strong>g practicesacross <strong>the</strong> whole organisation … It is yet ano<strong>the</strong>r change, and I th<strong>in</strong>k certa<strong>in</strong>ly peopleare fed up <strong>of</strong> change and people do identify <strong>the</strong> national programme as be<strong>in</strong>g yetano<strong>the</strong>r <strong>IT</strong> project that is probably not go<strong>in</strong>g to work, that’s go<strong>in</strong>g to cost a great deal<strong>of</strong> money, and why should <strong>the</strong>y really cooperate with it?”—Cl<strong>in</strong>ician <strong>in</strong>volved <strong>in</strong>development <strong>of</strong> electronic patient records, Trust 15.1.2. Communication between <strong>the</strong> NPf<strong>IT</strong> and <strong>the</strong> <strong>NHS</strong>The lack <strong>of</strong> clarity from <strong>the</strong> NPf<strong>IT</strong> about future developments—with poorcommunication between NPf<strong>IT</strong> headquarters, <strong>the</strong> local service provider, andTrust managers—was reported to be a major concern <strong>in</strong> all four Trusts.Managers felt that local needs and advice have been ignored and expressedsentiments <strong>in</strong> <strong>in</strong>terviews <strong>of</strong> feel<strong>in</strong>g ignored, be<strong>in</strong>g “done unto,” anddisempowered (box 2). Participants’ views suggest a divide between <strong>the</strong>central NPf<strong>IT</strong> <strong>of</strong>fice and Trusts, with <strong>the</strong> latter perceiv<strong>in</strong>g <strong>the</strong> former as fail<strong>in</strong>gto understand local issues. This lack <strong>of</strong> communication seems to have filtered61
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1down, with managers report<strong>in</strong>g a reluctance to communicate <strong>the</strong> benefits <strong>of</strong><strong>the</strong> NPf<strong>IT</strong> to front l<strong>in</strong>e staff without hav<strong>in</strong>g answers to questions about what <strong>IT</strong>services will be supplied and when (box 2).Box 2:Issues <strong>of</strong> communication with NPf<strong>IT</strong> headquarters and lack <strong>of</strong> cl<strong>in</strong>icalengagement“So I th<strong>in</strong>k we’ve not had, you know, we had some <strong>of</strong> <strong>the</strong> <strong>in</strong>teraction, and I th<strong>in</strong>k whatwe’ve been ask<strong>in</strong>g for is clarity about, um, gett<strong>in</strong>g th<strong>in</strong>gs done, what isn’t com<strong>in</strong>g,th<strong>in</strong>gs like. There was really someth<strong>in</strong>g last week about … <strong>the</strong> radiology systems,about <strong>the</strong> radiology <strong>in</strong>formation system and PACS, and <strong>in</strong> <strong>the</strong> application <strong>the</strong>re’s noradiology <strong>in</strong>formation system, <strong>the</strong>re’s just PACS.”—Executive director, Trust 2“The communication has been appall<strong>in</strong>g, absolutely appall<strong>in</strong>g. They’ve done somewonderful events, and I’ve met some people who are great, NPf<strong>IT</strong>, who are veryfacilitative and very enabl<strong>in</strong>g, and <strong>the</strong> next week you’re told you’re not allowed to talkto <strong>the</strong>m. I’ve been to some meet<strong>in</strong>gs where I’ve met people who are very very good,and we’ve been ordered not, <strong>in</strong>structed, <strong>the</strong>y’ve been ordered and we’ve been<strong>in</strong>structed that it’s <strong>in</strong>appropriate to talk to <strong>the</strong>m.—<strong>IT</strong> manager, Trust 4“Despite what people say <strong>the</strong>re’s a lack <strong>of</strong>, <strong>the</strong>re’s a lack <strong>of</strong> engagement and, youknow, even as chief executives, I th<strong>in</strong>k we’ve been <strong>in</strong>volved and been asked topromote someth<strong>in</strong>g <strong>the</strong>y, we’re promot<strong>in</strong>g—we say it’s a bit like try<strong>in</strong>g to go and sell,probably <strong>in</strong> <strong>IT</strong> terms, vapourware and that’s really what it felt like.”—Chief executive,Trust 3“I would say that <strong>the</strong> cl<strong>in</strong>icians are sort <strong>of</strong> wait<strong>in</strong>g to see what’s go<strong>in</strong>g to happenbefore <strong>the</strong>y commit <strong>the</strong>mselves.”—Assistant director <strong>of</strong> nurs<strong>in</strong>g, Trust 45.1.3. F<strong>in</strong>ancial circumstances <strong>of</strong> TrustsTwo <strong>of</strong> <strong>the</strong> Trusts had substantial f<strong>in</strong>ancial deficits, which were reported ascontribut<strong>in</strong>g to slow progress on local <strong>IT</strong> projects (box 3). Central fund<strong>in</strong>g doesnot cover all <strong>of</strong> <strong>the</strong> costs <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> care record service, and local <strong>IT</strong>spend<strong>in</strong>g must be susta<strong>in</strong>ed or <strong>in</strong>creased to provide <strong>the</strong> <strong>in</strong>frastructurenecessary to support it. 88 For participants, fund<strong>in</strong>g for <strong>the</strong> changemanagement associated with <strong>the</strong> care record service was a key concern. Upto March 2004, <strong>in</strong>stead <strong>of</strong> <strong>in</strong>creas<strong>in</strong>g spend<strong>in</strong>g, participants <strong>in</strong> “cash strapped”Trusts reported that scheduled <strong>IT</strong> implementation had been halted to awaitdetails <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> to be made public (box 3). Understandably, Trusts may bereluctant to spend on <strong>IT</strong> if some <strong>of</strong> <strong>the</strong> cost will be covered centrally. This lack<strong>of</strong> certa<strong>in</strong>ty seems to have created “plann<strong>in</strong>g blight,” with participants report<strong>in</strong>g62
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1that few <strong>IT</strong> <strong>in</strong>itiatives have been championed (box 3), thus potentially widen<strong>in</strong>g<strong>the</strong> <strong>IT</strong> gap between “cash rich” and “cash poor” Trusts.5.1.4. Performance rat<strong>in</strong>gsFor Trusts with a low performance rat<strong>in</strong>g (0 or 1 star), improv<strong>in</strong>g this rat<strong>in</strong>gwas reported as a press<strong>in</strong>g concern (box 4). (Although <strong>the</strong> future <strong>of</strong>performance rat<strong>in</strong>gs is under review, performance <strong>in</strong>dicators are likely tocont<strong>in</strong>ue to be a key focus for Trust managers.) Benefits <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> (whichhas a 10 year roll out), such as f<strong>in</strong>ancial sav<strong>in</strong>gs and improved patient care,will not be realised until after money has been spent on implementation. Thiswill probably require <strong>in</strong>vestment <strong>in</strong> staff tra<strong>in</strong><strong>in</strong>g as well as <strong>the</strong> <strong>IT</strong> <strong>in</strong>frastructure,perhaps temporarily reduc<strong>in</strong>g staff time available for cl<strong>in</strong>ical care. Trusts arelikely to avoid any activity that decreases ra<strong>the</strong>r than <strong>in</strong>creases productivityunless sufficient extra f<strong>in</strong>ancial and human resources are provided (box 4).Box 3: Issues <strong>of</strong> f<strong>in</strong>ancial deficits“I mean our first, our number one priority <strong>in</strong> this Trust been stated by <strong>the</strong> [chiefexecutive], and is quite clear to anybody, is money. We have to claw back our deficit,a huge deficit; [name] has an ever bigger one, and we are a very, um, broke strategichealth authority, actually, but particularly this local health community. We’re verystrapped for cash, and we have to f<strong>in</strong>d millions and millions <strong>of</strong> pounds worth <strong>of</strong>sav<strong>in</strong>g this year alone and <strong>in</strong>deed over <strong>the</strong> next three years.”—<strong>IT</strong> and NPf<strong>IT</strong> projectmanager, Trust 3“And we have a senior management that have too much on <strong>the</strong>ir plate to cope with at<strong>the</strong> moment, and EPR [electronic patient records] and <strong>IT</strong>, as well as between [largefigure] million pound underly<strong>in</strong>g deficit. We’re certa<strong>in</strong>ly not a Trust that can <strong>in</strong>vestfrom our own resources.”—Medical director, Trust 1“We’ve made real progress, um, <strong>in</strong> <strong>the</strong> development <strong>of</strong> our EPR programme, andthose who’ve done so much work <strong>in</strong> that particular programme are naturally quitedistressed if our particular EPR programme is simply go<strong>in</strong>g to go on hold for two,three, or four years, while we wait for a national programme to be implemented.”—Medical director, Trust 1“You know, <strong>the</strong> abandonment, <strong>the</strong> abandonment <strong>of</strong> <strong>the</strong> EPR has had an affect onpeople’s desire to get <strong>in</strong>volved too much <strong>in</strong> that way—let’s wait until a bit later … Ith<strong>in</strong>k <strong>the</strong>re’s a ‘Let’s just not <strong>in</strong>vest too much time’ attitude at <strong>the</strong> moment and seehow it goes from here.”—Assistant director <strong>of</strong> nurs<strong>in</strong>g, Trust 463
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 4: Issues <strong>of</strong> performance rat<strong>in</strong>gs“At <strong>the</strong> moment, you know, a lot <strong>of</strong> chief [executives], a lot <strong>of</strong> your short term focus ison star rat<strong>in</strong>gs and performance management because that’s where, you know, <strong>the</strong>carrot, that’s why you’re driven down that route. So, you know, we’re paid to do thatand keep <strong>the</strong> strategic vision go<strong>in</strong>g, but it depends how much pressure you get aboutwhere your focus could be.”—Executive director, Trust 2“So if that national programme wants this to happen <strong>the</strong>y, <strong>the</strong> government, whoever,must make sure any moneys that come down through whatever route are r<strong>in</strong>gfenced, and <strong>the</strong>y’re r<strong>in</strong>g fenced right down to Trust level, so that creative f<strong>in</strong>ancedirectors and o<strong>the</strong>rs cannot divert <strong>the</strong>m for o<strong>the</strong>r purposes.”—<strong>IT</strong> and NPf<strong>IT</strong> projectmanager, Trust 35.1.5. Support<strong>in</strong>g “legacy” <strong>IT</strong> systemsThe <strong>NHS</strong> has traditionally devolved <strong>IT</strong> procurement, result<strong>in</strong>g <strong>in</strong> a proliferation<strong>of</strong> <strong>IT</strong> architecture. This approach contrasts with centralised standard sett<strong>in</strong>gand procurement under <strong>the</strong> NPf<strong>IT</strong>. Potential legacy problems reported byparticipants are <strong>the</strong> loss <strong>of</strong> exist<strong>in</strong>g electronic functionality and concerns oversupport for exist<strong>in</strong>g systems dur<strong>in</strong>g any transition period.All Trusts <strong>in</strong> our study reported hav<strong>in</strong>g highly effective customised pockets <strong>of</strong><strong>IT</strong>. If <strong>the</strong>se systems cannot be <strong>in</strong>tegrated with national “standards” somefunctionality may be lost (box 5). Loss <strong>of</strong> exist<strong>in</strong>g <strong>IT</strong> function may stallprogress and is likely to be resisted. <strong>IT</strong> literate cl<strong>in</strong>icians <strong>in</strong> our samplereported work<strong>in</strong>g hard to develop systems that best support <strong>the</strong>ir needs and<strong>the</strong> needs <strong>of</strong> <strong>the</strong>ir patients (box 5).Replac<strong>in</strong>g exist<strong>in</strong>g systems will require contracts with exist<strong>in</strong>g suppliers to beredrawn. Ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g goodwill and cont<strong>in</strong>ued support for such systems may bedifficult. Trusts that actively pursued <strong>the</strong> orig<strong>in</strong>al plan for electronic patientrecords 5 may be particularly disadvantaged if <strong>the</strong>y are bound <strong>in</strong>to long termcontracts with suppliers not awarded contracts under <strong>the</strong> national procurementprocess.64
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 5: Issues <strong>of</strong> loss <strong>of</strong> functionality and resistance from cl<strong>in</strong>icians“There’s a feel<strong>in</strong>g <strong>of</strong> loss <strong>of</strong> autonomy, um, and possibly lack <strong>of</strong> or loss <strong>of</strong>functionality, because some <strong>of</strong> <strong>the</strong> systems that we’ve got are, have been developedover a period <strong>of</strong> time, and <strong>the</strong>y’re pretty well customised and people get used to thatlevel <strong>of</strong> customisation.”—Chief executive, Trust 4“Where it needs tailor<strong>in</strong>g to local Trusts—I don’t th<strong>in</strong>k that’s be<strong>in</strong>g listened to at all,and that’s where <strong>the</strong>y’re go<strong>in</strong>g to f<strong>in</strong>d <strong>the</strong> biggest amount <strong>of</strong> resistance, which iswhere local systems will always be better than <strong>the</strong> national solution.”—Electronicpatient records and NPf<strong>IT</strong> programme manager, Trust 2“Our <strong>IT</strong>U consultant writes programmes: he wrote <strong>the</strong> <strong>IT</strong>U one here, and he’s writ<strong>in</strong>gus a little program for duty doctor handover. It’s like swimm<strong>in</strong>g <strong>in</strong> treacle to get it<strong>in</strong>tegrated <strong>in</strong>to our system. You can’t get it if you’re <strong>in</strong> a, you know, <strong>in</strong> a regimentedsystem that is becom<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>gly.”—Medical director, Trust 1“If we’re say<strong>in</strong>g to people, ‘You have to drop what you’ve got to a lower function,’ wellthat’s go<strong>in</strong>g to be very hard to sell.”—<strong>IT</strong> director, Trust 4“Until we can get that level <strong>of</strong> functionality built <strong>in</strong>to <strong>the</strong> national solution nobody isgo<strong>in</strong>g to use it, well not from our Trust anyway.”—Electronic patient records andNPf<strong>IT</strong> programme manager, Trust 2“So, yeah, <strong>the</strong>y may have been work<strong>in</strong>g overtime develop<strong>in</strong>g <strong>the</strong>ir own system andnow are be<strong>in</strong>g told, ‘No, you can’t use it.’ And you have someth<strong>in</strong>g which isn’t asgood or doesn’t allow as much functionality or flexibility perhaps as someth<strong>in</strong>gelse.”—Research and development bus<strong>in</strong>ess manager, Trust 2“As a tax payer, I’m furious, as a cl<strong>in</strong>ician who’s dedicated time speak<strong>in</strong>g on behalf <strong>of</strong>o<strong>the</strong>r pr<strong>of</strong>essionals who’ve spent hours <strong>of</strong> unpaid time try<strong>in</strong>g to make this work, <strong>the</strong>yfeel devalued, marg<strong>in</strong>alised, and ignored. So <strong>the</strong>re’s enormous anger <strong>in</strong> thisorganisation, particularly at [name], with <strong>the</strong> way <strong>in</strong> which we’ve been dismissivelytreated.”—Medical director, Trust 15.1.6. Timetable for replacement <strong>of</strong> patient adm<strong>in</strong>istration systemsTo implement <strong>the</strong> care records service s<strong>of</strong>tware, most Trusts will need toreplace <strong>the</strong>ir exist<strong>in</strong>g patient adm<strong>in</strong>istration systems. The new adm<strong>in</strong>istrationsystem will act as a foundation on which additional “bundles” <strong>of</strong> cl<strong>in</strong>icalfunctions can be added. However, patient adm<strong>in</strong>istration systems cannot bereplaced immediately <strong>in</strong> all Trusts. For example, <strong>in</strong> London this activity aloneis projected to take up to five years. The tim<strong>in</strong>g <strong>of</strong> this replacement is caus<strong>in</strong>gconcern, and participants reported that <strong>the</strong>ir Trusts have been jostl<strong>in</strong>g for aslot that meets <strong>the</strong>ir particular needs (box 6).Three Trusts have reported an urgent need to replace exist<strong>in</strong>g adm<strong>in</strong>istrationsystems for radiology or pathology. Accord<strong>in</strong>g to participants, <strong>the</strong> previouslyscheduled implementation <strong>of</strong> such replacement systems has been put on hold65
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1until details <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> have been made public (box 6). Such delay maymean a risk <strong>of</strong> system failure, but buy<strong>in</strong>g a temporary solution is seen ascostly. Be<strong>in</strong>g first <strong>in</strong> <strong>the</strong> queue for implement<strong>in</strong>g <strong>the</strong> care records service may<strong>in</strong>crease <strong>the</strong> risk <strong>of</strong> delays and teeth<strong>in</strong>g problems, with details <strong>of</strong> forthcom<strong>in</strong>gsupport from <strong>the</strong> local service provider for change management still unclear.However, be<strong>in</strong>g at <strong>the</strong> end <strong>of</strong> <strong>the</strong> queue may lead to “plann<strong>in</strong>g blight,” with nonew local <strong>IT</strong> development until <strong>the</strong> new adm<strong>in</strong>istration system is provided (box6). 88Box 6: Jostl<strong>in</strong>g for a new patient adm<strong>in</strong>istration system (PAS), concern overdelays, and “plann<strong>in</strong>g blight”“And so, obviously everybody wants <strong>the</strong> [new] PAS straight away, and you’reobviously <strong>in</strong> <strong>the</strong> queue for that with everybody else.”—Divisional manager, Trust 4“It’s go<strong>in</strong>g to be an absolute scrabble, you know, and I’m a bit annoyed. We went to alaunch day for <strong>the</strong>, for <strong>the</strong> [local service provider] and one <strong>of</strong> questions I said, ‘Youknow, <strong>the</strong>re’s 77 Trusts, a limited number <strong>of</strong> slots [for PAS replacement], you know, itis go<strong>in</strong>g to be a big bun fight.’”—<strong>IT</strong> director, Trust 4“If we aren’t one <strong>of</strong> <strong>the</strong> first PAS’s, which I don’t th<strong>in</strong>k we are, it could be 2010 orsometh<strong>in</strong>g before we even get a PAS, and <strong>the</strong>n, you know, we’ve got to implementall <strong>the</strong> various compliant systems. So it could be a, over a decade before anybody,you know, and it will be over a decade <strong>in</strong> some places before anybody at someTrusts see any difference.—Chief executive, Trust 4“Our biggest sort <strong>of</strong> stopp<strong>in</strong>g block for tak<strong>in</strong>g anyth<strong>in</strong>g from NPf<strong>IT</strong> is <strong>the</strong> fact that n<strong>in</strong>etimes out <strong>of</strong> 10 we’ve got to have <strong>the</strong> [new] PAS <strong>in</strong>, so, as much as we would like totake some <strong>of</strong> <strong>the</strong> modules, we can’t—Electronic patient records and NPf<strong>IT</strong>programme manager, Trust 2“It’s, well, it’s been delayed basically. I mean <strong>in</strong> implementation, purchase andimplementation <strong>of</strong> <strong>the</strong> system by a year and a half, I th<strong>in</strong>k, while we’re <strong>in</strong>evitablywait<strong>in</strong>g for <strong>the</strong> [local service provider] to be sorted, and now we’re wait<strong>in</strong>g for <strong>the</strong>process to go though … It’s a bit <strong>of</strong> a mish-mash go<strong>in</strong>g on <strong>the</strong>re, I must say. Um, Ith<strong>in</strong>k, you know, you’ve got to k<strong>in</strong>d <strong>of</strong> look at your local priorities <strong>in</strong> this case and say,‘We need a new system <strong>in</strong> for risk factors and for manag<strong>in</strong>g demand and record<strong>in</strong>gdata better, um, and we need to go ahead and purchase as soon as we can.’”—Divisional manager, Trust 4“NPf<strong>IT</strong> for London said, ‘No, you have to do it this way.’ And it’s not, it’s just not up fornegotiation, it is a very centrally driven mandate. ‘You will take PAS, you will takesome m<strong>in</strong>imum orders that <strong>in</strong>clude maternity and <strong>the</strong>atres, and <strong>the</strong>n you can takesome prescrib<strong>in</strong>g and some pathways.’ So, we were def<strong>in</strong>itely aim<strong>in</strong>g to do <strong>the</strong>cl<strong>in</strong>ical end <strong>of</strong> th<strong>in</strong>gs first … it is frustrat<strong>in</strong>g because that’s—you’re right, <strong>in</strong> terms <strong>of</strong>strategy we did not want to do our PAS next and we did not want to do <strong>the</strong>atres andmaternity.”—<strong>IT</strong> director, Trust 466
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 15.2. Stage b.: resultsSix ma<strong>in</strong> <strong>the</strong>mes emerged from our phase a <strong>of</strong> this part <strong>of</strong> <strong>the</strong> study 86 :1. The impact <strong>of</strong> multiple sites result<strong>in</strong>g from recent mergers2. Poor communication between Connect<strong>in</strong>g for Health (CfH) and localmanagers3. The impact <strong>of</strong> f<strong>in</strong>ancial deficits4. The need to prioritise performance targets5. Support<strong>in</strong>g exist<strong>in</strong>g ‘legacy’ <strong>IT</strong> systems6. The delayed timetable for replacement patient adm<strong>in</strong>istration systemsEighteen months later, three <strong>of</strong> <strong>the</strong> previous concerns were still apparent (<strong>the</strong>mes2, 4, 5 below) and five new issues were raised:1. Increased support for <strong>the</strong> overall goals <strong>of</strong> <strong>the</strong> programme2. Cont<strong>in</strong>u<strong>in</strong>g impact <strong>of</strong> f<strong>in</strong>ancial deficits3. Managers distracted from implement<strong>in</strong>g <strong>the</strong> programme by o<strong>the</strong>r priorities4. Cont<strong>in</strong>u<strong>in</strong>g poor communication between CfH and local managers5. Cont<strong>in</strong>u<strong>in</strong>g delay <strong>in</strong> replac<strong>in</strong>g patient adm<strong>in</strong>istration systems6. Grow<strong>in</strong>g risk to patient safety associated with delays7. Loss <strong>of</strong> <strong>in</strong>tegration <strong>of</strong> components <strong>of</strong> <strong>the</strong> programme8. Discontent with Choose & BookThe issues raised <strong>in</strong> <strong>in</strong>terviews were similar among staff who had taken part <strong>in</strong><strong>the</strong> first round <strong>of</strong> <strong>in</strong>terviews and among staff who not been <strong>in</strong>terviewedpreviously.5.2.1. Increased support for <strong>the</strong> goals <strong>of</strong> <strong>the</strong> programmeS<strong>in</strong>ce <strong>the</strong> first round <strong>of</strong> <strong>in</strong>terviews, we found that support for <strong>the</strong> conceptunderly<strong>in</strong>g <strong>the</strong> programme had grown. The overrid<strong>in</strong>g view was that <strong>the</strong> <strong>NHS</strong>urgently needs <strong>the</strong> benefits that can be ga<strong>in</strong>ed from <strong>IT</strong> <strong>modernisation</strong>implemented <strong>in</strong> a standardised way. (Box 7) We found very little resistance to<strong>IT</strong> <strong>modernisation</strong>, with <strong>in</strong>terviewees report<strong>in</strong>g that <strong>the</strong>ir staff are ready, andsometimes “desperate”, for progress. However, alongside this grow<strong>in</strong>gsupport, we also found concern about <strong>the</strong> ability <strong>of</strong> programme managers todeliver <strong>the</strong> programme. To ma<strong>in</strong>ta<strong>in</strong> momentum, <strong>in</strong>terviewees said that CfH67
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1needed to deliver products that work very soon. They also emphasised <strong>the</strong>need for <strong>in</strong>dependent evaluation to measure <strong>the</strong> benefits and costs (Box 8).Box 7: Increased support for <strong>the</strong> overall goals <strong>of</strong> <strong>the</strong> <strong>NHS</strong> <strong>IT</strong> programme“I still ma<strong>in</strong>ta<strong>in</strong> it’s <strong>the</strong> right th<strong>in</strong>g to do. I th<strong>in</strong>k <strong>the</strong> pr<strong>in</strong>ciple, <strong>the</strong> pr<strong>in</strong>ciples, <strong>the</strong>philosophy and <strong>the</strong> vision I th<strong>in</strong>k are absolutely sound. The challenge has beendeliverability …” [Chief executive, Trust 4]“two years on I still believe <strong>in</strong> <strong>the</strong> concept, um, because I th<strong>in</strong>k <strong>the</strong> biggest s<strong>in</strong>gleproblem we have is shar<strong>in</strong>g <strong>in</strong>formation between organisations and actually evenwith<strong>in</strong> organisations, so <strong>the</strong> idea <strong>of</strong> hav<strong>in</strong>g a s<strong>in</strong>gle system or common systems as an<strong>IT</strong> concept only makes sense” [Director <strong>of</strong> IM & T, Trust 4]“The consequences are, um, a complete re-th<strong>in</strong>k about <strong>the</strong> way that, um, <strong>IT</strong> is<strong>in</strong>troduced and it’s needed it desperately…<strong>NHS</strong> <strong>IT</strong> programme is visionary, brilliant”[Director <strong>of</strong> IM & T, Trust 2]Box 8: More product placement and benefits realisation“We have to get some confidence back <strong>in</strong>to <strong>the</strong> programme and that has to be aboutdelivery because <strong>the</strong>y can talk until <strong>the</strong> cows come home, but unless we seesometh<strong>in</strong>g happen<strong>in</strong>g on our own patch with a real cl<strong>in</strong>ical w<strong>in</strong> to keep peopleonboard…” [Director <strong>of</strong> IM & T, Trust 4]“I th<strong>in</strong>k one <strong>of</strong> <strong>the</strong> th<strong>in</strong>gs that <strong>the</strong>y haven’t done very well is clarify some <strong>of</strong> <strong>the</strong>benefits <strong>the</strong>y th<strong>in</strong>k that you’re go<strong>in</strong>g to get out <strong>of</strong> it. …I haven’t seen, you know, agood list <strong>of</strong> benefits… I mean, you know, about between GPs and consultants, Imean actually th<strong>in</strong>gs like manag<strong>in</strong>g a wait<strong>in</strong>g list” [Director <strong>of</strong> performance andimprovement <strong>of</strong> <strong>in</strong>formation, Trust 1]“I th<strong>in</strong>k <strong>the</strong>…two big difficulties, <strong>the</strong> two big issues will be affordability, is it reallygo<strong>in</strong>g to deliver <strong>the</strong> benefits, um, for <strong>the</strong> cost and is it, is it a cost pressure ra<strong>the</strong>r thanan enabler <strong>of</strong> better efficiency across <strong>the</strong> organisation as a whole? …we aredependent on gett<strong>in</strong>g benefits out <strong>of</strong> it. …and I’m not confident at this stage thisstage that <strong>the</strong> system <strong>in</strong> operation will be so beneficial that it will really drive loads <strong>of</strong>th<strong>in</strong>gs forward” [Chief executive, Trust 3]5.2.2. Cont<strong>in</strong>u<strong>in</strong>g impact <strong>of</strong> f<strong>in</strong>ancial deficitsIn our earlier <strong>in</strong>terviews, senior staff <strong>in</strong> Trusts fac<strong>in</strong>g f<strong>in</strong>ancial difficulties wereconcerned about how to pay for <strong>the</strong> implementation costs associated with <strong>IT</strong><strong>modernisation</strong>. Currently, f<strong>in</strong>ancial difficulties with<strong>in</strong> <strong>the</strong> <strong>NHS</strong> are even morewidespread and this issue has become more important. Respondentsreported that mak<strong>in</strong>g sav<strong>in</strong>gs is now more critical and that applications whichare part <strong>of</strong> <strong>the</strong> programme are not <strong>the</strong> barga<strong>in</strong> <strong>the</strong>y were expected to be.Implementation <strong>of</strong> picture archive and communication systems (PACS) is also68
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1caus<strong>in</strong>g disquiet.Some respondents reported that PACS applicationssupplied through <strong>the</strong> programme appear to be more expensive than marketalternatives (Box 3) but a central CfH mandate has left <strong>the</strong>m with no choicebut to implement <strong>the</strong> more expensive programme option. (Box 9)Box 10: Expensive solutions especially PACS implementation“a lot <strong>of</strong> <strong>the</strong> th<strong>in</strong>gs are be<strong>in</strong>g sold to us at a much higher price than we would havebeen able to get if we’d been <strong>in</strong> a real market situation, so <strong>the</strong> total costs to <strong>the</strong> <strong>NHS</strong>have been very high <strong>in</strong>deed.” [Medical director, Trust 4]“You know, we went out to procure a PACS system that was not part <strong>of</strong> <strong>the</strong> nationalprogramme, and, you know, got told we couldn’t do it. That’s resulted <strong>in</strong> more, a lotmore expenditure for <strong>the</strong> Trust than <strong>the</strong> local solution, so I th<strong>in</strong>k that <strong>the</strong>n heapsano<strong>the</strong>r layer <strong>of</strong> problems on… where we have a deficit, um, to be forced down aroute that’s more expensive without…f<strong>in</strong>ancial support that really we should begett<strong>in</strong>g about that, you know, it’s just ano<strong>the</strong>r dis<strong>in</strong>centive really.” [Chief executive,Trust 2]“it’s certa<strong>in</strong>ly extensive costs, um, and it’s compulsory acquisition, we have to have it<strong>in</strong> by March, that’s it. So, it’s, it’s just a cost pressure, it’s ano<strong>the</strong>r, ano<strong>the</strong>r one <strong>of</strong>many cost pressures at <strong>the</strong> Trust.” [Head <strong>of</strong> system delivery, Trust 1]5.2.3. Managers distracted from implement<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> by o<strong>the</strong>rprioritiesF<strong>in</strong>ancial deficits not only cause concern about how to pay for implementation<strong>of</strong> <strong>the</strong> programme but also act as significant distractions for managers. In <strong>the</strong>earlier <strong>in</strong>terviews, some Trust staff reported that recent mergers and <strong>the</strong> needto prioritise atta<strong>in</strong>ment <strong>of</strong> performance rat<strong>in</strong>gs made it difficult to prepare for<strong>the</strong> programme. Eighteen months later, <strong>the</strong> priority <strong>of</strong> Trust f<strong>in</strong>ancesdom<strong>in</strong>ated. Two <strong>of</strong> our four Trusts have had ‘turnaround teams’ <strong>in</strong> place(external consultants brought <strong>in</strong> to help Trusts resolve f<strong>in</strong>ancial crises). OneTrust also had <strong>the</strong> Department <strong>of</strong> Health’s performance support team work<strong>in</strong>gwith it. The dom<strong>in</strong>ant and immediate need to elim<strong>in</strong>ate any overspend, whilstma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g performance, appears to leave managers little time to commit toimplement<strong>in</strong>g <strong>the</strong> programme or any o<strong>the</strong>r new services or products. (Box 11)The programme was only reported to be a press<strong>in</strong>g priority <strong>in</strong> Trusts wheremanagers perceived a significant risk to patient safety from hav<strong>in</strong>g to ma<strong>in</strong>ta<strong>in</strong>exist<strong>in</strong>g legacy systems while wait<strong>in</strong>g for new systems to arrive. (Box 15)69
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 15.2.4. Poor communication between Connect<strong>in</strong>g for Health and localmanagersPreviously, <strong>in</strong>terviewees <strong>in</strong> all four Trusts were concerned with a lack <strong>of</strong> clarityfrom CfH about <strong>the</strong> timetable for implementation.Eighteen months later,although respondents were enthusiastic about <strong>the</strong> goals <strong>of</strong> <strong>the</strong> programme,<strong>the</strong> perception <strong>of</strong> poor communication was unchanged.There is stilluncerta<strong>in</strong>ty about <strong>the</strong> timetable for delivery <strong>of</strong> key components <strong>of</strong> <strong>the</strong>programme (e.g. core hospital adm<strong>in</strong>istration systems compliant with <strong>the</strong>hardware and s<strong>of</strong>tware applications that will make up <strong>the</strong> programme) andabout <strong>the</strong> extent <strong>of</strong> f<strong>in</strong>ancial assistance for ‘required’ components.Respondents reported that much <strong>of</strong> <strong>the</strong> decision mak<strong>in</strong>g has been betweenCfH and <strong>the</strong> local <strong>IT</strong> service provider. This lack <strong>of</strong> local <strong>in</strong>volvement appearsto have <strong>in</strong>creased feel<strong>in</strong>gs <strong>of</strong> disempowerment and frustration. (Box 12) Theuncerta<strong>in</strong>ty has also resulted <strong>in</strong> some Trusts adopt<strong>in</strong>g policies that activelydiscourage staff from engag<strong>in</strong>g with <strong>the</strong> programme (Box 13).Box 11:Managers distracted from implement<strong>in</strong>g <strong>the</strong> <strong>NHS</strong> <strong>IT</strong> programme byo<strong>the</strong>r priorities“Actually motivat<strong>in</strong>g people <strong>in</strong> this particular Trust at this particular time to have <strong>the</strong>vision to get <strong>in</strong>volved <strong>in</strong> a nation-wide project, which isn’t delivery, is virtuallyimpossible. The majority <strong>of</strong> my colleagues are surviv<strong>in</strong>g day to day with no beds,cuts… There are real immediate issues, <strong>the</strong>re isn’t <strong>the</strong>, um, <strong>the</strong> luxury, I suppose, <strong>of</strong>people hav<strong>in</strong>g <strong>the</strong> time and <strong>the</strong> <strong>in</strong>tellectual capacity to pursue a ten year vision. Wetry to, we’re try<strong>in</strong>g to survive.” [Medical director, Trust 2]“I would like to see good <strong>IT</strong> systems with<strong>in</strong> <strong>the</strong> <strong>NHS</strong>…where I’m com<strong>in</strong>g from <strong>in</strong> aTrust that’s got <strong>the</strong> Performance Support Team <strong>in</strong> and we’ve got <strong>the</strong> TurnaroundTeam <strong>in</strong>, um, we are try<strong>in</strong>g to pull out a great deal <strong>of</strong> expenditure about ten percent<strong>of</strong> our budget…it does feel a little unreal try<strong>in</strong>g to implement a large <strong>IT</strong> system on top<strong>of</strong> that… <strong>the</strong>re’s no real plans yet because we haven’t got that far. And, to behonest, <strong>the</strong> whole o<strong>the</strong>r agenda [mak<strong>in</strong>g sav<strong>in</strong>gs] is just tak<strong>in</strong>g my time up.” [Director<strong>of</strong> nurs<strong>in</strong>g, Trust 1]70
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 12: Cont<strong>in</strong>ued uncerta<strong>in</strong>ty and feel<strong>in</strong>g <strong>of</strong> disempowerment“The frustration is we’re not <strong>the</strong> customers, as far as <strong>the</strong> suppliers are concerned….CfH pull <strong>the</strong> str<strong>in</strong>gs, it’s <strong>the</strong>ir contract, we’re just <strong>the</strong> entity that takes <strong>the</strong> solution”[Director <strong>of</strong> IM & T, Trust 2]“The communication has been bloody awful really…we’ve k<strong>in</strong>d <strong>of</strong> been <strong>the</strong> recipients<strong>of</strong> those relationships as opposed to be<strong>in</strong>g directly as <strong>in</strong>fluential as we would like tobe <strong>in</strong> those relationships. I’m say<strong>in</strong>g is every two months we say “Where’s mypathology system?” “Oh, well, we’ve got to f<strong>in</strong>ish this …” so you k<strong>in</strong>d <strong>of</strong> tune out,that’s how it has felt, you’ve felt a little bit I guess disempowered really, um, because,you don’t have <strong>the</strong> <strong>in</strong>ternal levers to actually, most problems I’ve got I can sort out alot, but I feel it’s not with<strong>in</strong> my power to sort <strong>the</strong>m out.” [Chief executive Trust 4 ]“so ourselves k<strong>in</strong>d <strong>of</strong> at <strong>the</strong> bottom <strong>of</strong> <strong>the</strong> food cha<strong>in</strong> we just, we don’t get <strong>in</strong>volved <strong>in</strong>any <strong>of</strong> this and it has been two-and-a-half years, it seems to be solid negotiation andre-negotiation between <strong>NHS</strong> <strong>IT</strong> programme and BT.” [Director <strong>of</strong> IM & T, Trust 4]Box 13: Lack <strong>of</strong> cl<strong>in</strong>ician engagement“I’m not driv<strong>in</strong>g <strong>the</strong> national programme forward at all…. We’re not do<strong>in</strong>g anyenabl<strong>in</strong>g at all as far as that process is concerned. I’m def<strong>in</strong>itely not go<strong>in</strong>g to do whatsome <strong>of</strong> my colleagues have and that’s work on <strong>the</strong> basis that <strong>the</strong>y were gett<strong>in</strong>g <strong>the</strong>irslots and have ended up with staff employed, ready to go and noth<strong>in</strong>g to go with.”[Director <strong>of</strong> IM & T, Trust 2]“we’ve actively discouraged it here [engagement], which is a strange th<strong>in</strong>g to do, <strong>in</strong> away, but because we didn’t want to raise expectations…<strong>the</strong>re is no s<strong>of</strong>tware back<strong>in</strong>gthat up at <strong>the</strong> moment, or not that we’ve seen…I don’t encourage our cl<strong>in</strong>icians to get<strong>in</strong>volved on <strong>the</strong> demonstration days.” [Director <strong>of</strong> IM & T, Trust 4]“I wouldn’t go out and sell it to people because I don’t know when it’s go<strong>in</strong>g to arrive.…gett<strong>in</strong>g people too enthusiastic on specific timescales would have been verydangerous.” [Chief executive, Trust 4]“I th<strong>in</strong>k <strong>the</strong> biggest problem we’ve had, as an organisation, is, um, you have to havea product to sell to <strong>the</strong> cl<strong>in</strong>ical staff to get <strong>the</strong>m enthused, to get <strong>the</strong>m to use it, and<strong>the</strong> biggest problem we’ve had is that <strong>the</strong> product has not revealed itself to us yet.”[Medical director, Trust 3]5.2.5. Cont<strong>in</strong>u<strong>in</strong>g delay <strong>in</strong> replac<strong>in</strong>g PASIn <strong>the</strong> first <strong>in</strong>terviews, respondents were concerned about when <strong>the</strong>ir PASwould be replaced. Orig<strong>in</strong>ally, <strong>the</strong> national programme planned for PAS to be<strong>in</strong>stalled before any cl<strong>in</strong>ical applications. Due to delays <strong>in</strong> develop<strong>in</strong>g a PASthat can achieve connectivity with <strong>the</strong> ‘sp<strong>in</strong>e’ (a nationally accessible summarypatient record) 89 , this plan has had to be revised and <strong>in</strong>terim <strong>of</strong>f-<strong>the</strong>-shelfapplications are now be<strong>in</strong>g <strong>of</strong>fered. The revised plan has slowed progress71
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1and Trusts are still unsure when <strong>the</strong>ir replacement PAS will be implemented.Interim applications will allow Trusts to move forward to some extent, but willnot achieve <strong>the</strong> promised wider connectivity with o<strong>the</strong>r <strong>NHS</strong> hospital Trustsand primary care teams. (Box 14)5.2.6. Grow<strong>in</strong>g risk to patient safety associated with delaysBefore <strong>the</strong> NPf<strong>IT</strong> was conceived, <strong>NHS</strong> hospitals bought <strong>the</strong>ir own <strong>IT</strong> systems.When first <strong>in</strong>terviewed, senior cl<strong>in</strong>icians were worried that <strong>the</strong> replacement <strong>of</strong><strong>the</strong>se systems (<strong>of</strong>ten carefully customised to meet local needs) might result <strong>in</strong>a loss <strong>of</strong> functionality. This concern, though still evident <strong>in</strong> stage b. <strong>in</strong>terviews,has been largely superseded by <strong>the</strong> urgent need to replace legacy systems.When details <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong> were announced <strong>in</strong> late 2002, many Trusts stopped<strong>in</strong>vest<strong>in</strong>g <strong>in</strong> <strong>the</strong>ir exist<strong>in</strong>g <strong>IT</strong> systems, choos<strong>in</strong>g <strong>in</strong>stead to spend money ono<strong>the</strong>r priorities while wait<strong>in</strong>g for applications compliant with <strong>the</strong> programmesystems to be supplied. Delays mean that Trusts <strong>in</strong> our study are still wait<strong>in</strong>gfor new systems. Where replacement systems were needed <strong>in</strong> 2002, <strong>the</strong>delay is now perceived to represent an unacceptable risk to patient safety,with Trusts consider<strong>in</strong>g buy<strong>in</strong>g <strong>in</strong>terim systems outside <strong>the</strong> NPf<strong>IT</strong>. (Box 15)Box 14 Cont<strong>in</strong>ued delays and re-plann<strong>in</strong>g“<strong>the</strong> dates keep gett<strong>in</strong>g re-planned because we’re not allowed to say delayedanymore we joke <strong>in</strong> this Trust that <strong>NHS</strong> <strong>IT</strong> programme is never closer than two yearsaway and just when you th<strong>in</strong>k it’s actually go<strong>in</strong>g to be closer it suddenly goes….aga<strong>in</strong> and it’s two years away aga<strong>in</strong>.” [Systems tra<strong>in</strong><strong>in</strong>g manager, Trust 3]“I see all <strong>the</strong> sort <strong>of</strong> stuff, <strong>the</strong> propaganda that comes out from CfH and <strong>the</strong>y’realways say<strong>in</strong>g how a lot <strong>of</strong> <strong>the</strong>se th<strong>in</strong>gs are actually on time, despite what <strong>the</strong> presssays, um, hundreds <strong>of</strong> people are us<strong>in</strong>g <strong>the</strong> new systems and all that sort <strong>of</strong>, and Imust say, you know, <strong>the</strong>re’s not an awful lot <strong>of</strong> evidence <strong>of</strong> that across <strong>the</strong> country, Idon’t th<strong>in</strong>k.” [Cl<strong>in</strong>ician lead for CfH, Trust 2]“They obviously, <strong>the</strong>y know that <strong>the</strong> CRS isn’t go<strong>in</strong>g to deliver <strong>in</strong> a sort timelymanner, so <strong>the</strong>y’re k<strong>in</strong>d <strong>of</strong> look<strong>in</strong>g at this o<strong>the</strong>r product to work with exist<strong>in</strong>g PASs.”[Assist. director <strong>of</strong> IM & T, Trust 4]“so we’ve got <strong>the</strong>se tactical solutions com<strong>in</strong>g <strong>in</strong> and that helps because we’re seen tobe mov<strong>in</strong>g forward. My only problem with tactical solutions is that <strong>in</strong> a few year’stime one expects that tactical solutions to be replaced with whatever IDX is go<strong>in</strong>g todemand and I don’t know that I really want to put my Trust through implement<strong>in</strong>g atactical PAS and <strong>the</strong>n do<strong>in</strong>g it aga<strong>in</strong>.” [Director <strong>of</strong> IM & T, Trust 2]72
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 15: Concern over grow<strong>in</strong>g risk to patient safety, some Trust may go italone.“…our path system is extremely out <strong>of</strong> date, it’s not just obsolescent, it’s obsolete.When we had to buy some new bits for it recently we had to buy <strong>the</strong>m through Ebayfrom someone <strong>in</strong> America because <strong>the</strong>re’s just no bits <strong>in</strong> this country, so it’s a hugerisk to <strong>the</strong> Trust that we’re still carry<strong>in</strong>g this path system…” [Medical director, Trust 4]“It’s been urgent that it’s replaced all <strong>the</strong> time I’ve been here, which is about threeand-a-halfyears, so I mean <strong>the</strong> first th<strong>in</strong>g I heard about when I arrived was <strong>the</strong> factthat <strong>the</strong> PAS system needed to be replaced. It is a cl<strong>in</strong>ical risk” [Director <strong>of</strong> nurs<strong>in</strong>g,Trust 1]“And <strong>the</strong>re are a number <strong>of</strong> risks that are associated with our old system, some veryserious risks and risks <strong>in</strong> development and progress with<strong>in</strong> <strong>the</strong> organisation andbetween <strong>the</strong> organisations due to this lack <strong>of</strong> putt<strong>in</strong>g a good idea <strong>in</strong>to practice.[Divisional manager for diagnostic <strong>the</strong>rapies and outpatients, Trust 4]“that’s a risk we, that is a risk. I mean it could, you know, die tomorrow, it’s such anold system and <strong>the</strong>n we are really stuffed, basically.” [Director <strong>of</strong> nurs<strong>in</strong>g, Trust 2]“People are say<strong>in</strong>g ’Thank god we’re go<strong>in</strong>g to get a new system that will replace thisload <strong>of</strong> old, you know, cobblers.’…Americans use <strong>the</strong> expression “You need aburn<strong>in</strong>g platform to get change.” Well, I th<strong>in</strong>k from an <strong>IT</strong> perspective we’ve probablygot one.” [Director <strong>of</strong> IM & T, Trust 2]“One <strong>of</strong> <strong>the</strong> options I have is to say ’To hell with it, I’ll just go and buy one.’ Well,that’s a k<strong>in</strong>d <strong>of</strong> tricky decision and that’s <strong>the</strong> decision some <strong>of</strong> my peers are mak<strong>in</strong>gelsewhere, <strong>the</strong>y’re say<strong>in</strong>g ’Well, sod that, I’ll go elsewhere.’” [Divisional manager fordiagnostic <strong>the</strong>rapies and outpatients, Trust 4]5.2.7. Loss <strong>of</strong> <strong>in</strong>tegration <strong>of</strong> components <strong>of</strong> <strong>the</strong> programmeThe orig<strong>in</strong>al goal <strong>of</strong> access to <strong>in</strong>formation across <strong>the</strong> <strong>NHS</strong>, that underp<strong>in</strong>ned<strong>the</strong> <strong>NHS</strong> <strong>IT</strong> programme appears to have been lost. 90 The lack <strong>of</strong> <strong>in</strong>tegration<strong>of</strong>fered by <strong>in</strong>terim applications has left senior Trust staff question<strong>in</strong>g whe<strong>the</strong>r<strong>NHS</strong>-wide connectivity will ever be achieved and, if not, why Trusts have hadto wait several years for <strong>the</strong> new systems. The purchase <strong>of</strong> <strong>in</strong>terimapplications does not seem very far removed from how <strong>the</strong> <strong>NHS</strong> acquired <strong>IT</strong>before <strong>the</strong> programme, with <strong>the</strong> problems <strong>of</strong> this approach seem<strong>in</strong>glyperpetuated, such as databases that cannot be accessed from outside <strong>the</strong>Trust. (Box 16) Managers also questioned how <strong>the</strong> Government vision <strong>of</strong>decentralis<strong>in</strong>g cl<strong>in</strong>ical services, by <strong>in</strong>creas<strong>in</strong>g private sector provision, alignswith a centralised approach to <strong>in</strong>formation shar<strong>in</strong>g. (Box 16)73
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 16: Loss <strong>of</strong> <strong>in</strong>tegration <strong>of</strong> components <strong>of</strong> <strong>the</strong> <strong>NHS</strong> <strong>IT</strong> programme“I th<strong>in</strong>k it is back-peddl<strong>in</strong>g big time because I don’t th<strong>in</strong>k <strong>the</strong>, right now <strong>the</strong>y’re <strong>in</strong> aposition to deliver that orig<strong>in</strong>al vision and so even th<strong>in</strong>gs like <strong>the</strong> PACS was go<strong>in</strong>g tobe an <strong>NHS</strong>-wide archive and <strong>the</strong>n it was go<strong>in</strong>g to be a cluster archive and now<strong>the</strong>y’re just talk<strong>in</strong>g about hav<strong>in</strong>g a Trust archive” [Director <strong>of</strong> IM & T, Trust 4]I’m just worried that <strong>the</strong> ideas are actually drift<strong>in</strong>g away from <strong>the</strong> way that <strong>in</strong>itialstrategy, from <strong>the</strong> way <strong>the</strong> Trust is work<strong>in</strong>g, whereas at one time you k<strong>in</strong>d <strong>of</strong> <strong>of</strong>fered anice way forward I’m worried it’s k<strong>in</strong>d <strong>of</strong> diverg<strong>in</strong>g” [Divisional manager for diagnostic<strong>the</strong>rapies and outpatients, Trust 4]“One <strong>of</strong> <strong>the</strong> th<strong>in</strong>gs that’s become apparent is that <strong>the</strong> orig<strong>in</strong>al vision <strong>of</strong> a sharedrecord between primary and secondary care is not at <strong>the</strong> moment on <strong>the</strong>, on <strong>the</strong>design, aim and design….what <strong>the</strong>y’re look<strong>in</strong>g to do is to use messag<strong>in</strong>g systemsbetween primary and secondary care, so effectively you’ll have electronic letters anddischarge summaries and those sorts <strong>of</strong> reports …and <strong>the</strong> sp<strong>in</strong>e won’t, <strong>the</strong> sp<strong>in</strong>e iscurrently go<strong>in</strong>g to be quite th<strong>in</strong>, so it’s not go<strong>in</strong>g to be data rich.” [Cl<strong>in</strong>ician lead forCfH, Trust 2]“we’ve got foundation Trusts, we’ve got perhaps more importantly <strong>the</strong> mixedeconomy so, um, are we say<strong>in</strong>g that a condition <strong>of</strong> a private provider receiv<strong>in</strong>g <strong>NHS</strong>work is that <strong>the</strong>y have to be signed up to <strong>the</strong> national programme? …we’re not go<strong>in</strong>gto have a national solution that actually is fit for purpose <strong>in</strong> a mixed economy andproviders.” [Chief executive, Trust 2]“I genu<strong>in</strong>ely am not sure whe<strong>the</strong>r <strong>the</strong> solutions are solutions to yesterday’s analysisra<strong>the</strong>r than today’s analysis…. I th<strong>in</strong>k what’s happened over <strong>the</strong> last few years is wehave moved from <strong>NHS</strong> PLC to health care, as an <strong>in</strong>dustry, which has lots <strong>of</strong> differentplayers <strong>in</strong> it” [Chief executive, Trust 3]5.2.8. Discontent with Choose & BookFollow<strong>in</strong>g <strong>the</strong> stage A <strong>in</strong>terviews, acute Trusts and local primary care teamshave proceeded with implementation <strong>of</strong> Choose & Book, a system whichallows GPs to make patient appo<strong>in</strong>tments and referrals <strong>in</strong>to acute Trustselectronically. We found little support for <strong>the</strong> patient choice element <strong>of</strong>Choose & Book (patients be<strong>in</strong>g able to choose to be referred to one <strong>of</strong> a range<strong>of</strong> hospitals) among <strong>the</strong> staff we <strong>in</strong>terviewed. (Box 10) The technical problemsaffect<strong>in</strong>g electronic book<strong>in</strong>g have also underm<strong>in</strong>ed confidence <strong>in</strong> o<strong>the</strong>rplanned applications. None <strong>of</strong> <strong>the</strong> managers or cl<strong>in</strong>icians we <strong>in</strong>terviewed wereoptimistic about <strong>the</strong> ability <strong>of</strong> CfH to deliver <strong>the</strong> systems. The doubtsexpressed were tw<strong>of</strong>old; whe<strong>the</strong>r it was technically possible, and whe<strong>the</strong>r <strong>the</strong>products would be delivered <strong>in</strong> a reasonable time frame. Feel<strong>in</strong>gs <strong>of</strong>frustration were expressed at <strong>the</strong> slow progress. (Box 17)74
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1Box 17: Discontent with Choose & Book & loss <strong>of</strong> confidence <strong>in</strong> <strong>the</strong>programme“I’ve not really talked to <strong>the</strong> cl<strong>in</strong>icians about, about whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k it’s a good ideaor not [Care Records Service]. They certa<strong>in</strong>ly th<strong>in</strong>k choose, choose and book is acrap idea, <strong>the</strong>y hate it” [Director <strong>of</strong> performance and improvement <strong>of</strong> <strong>in</strong>formation,Trust 1]“we’ll call it choose and book because it helps with politics. The s<strong>of</strong>tware is not fit forpurpose…. We have an unstable middle-ware server because <strong>the</strong> sp<strong>in</strong>e keepsvanish<strong>in</strong>g…what happens is <strong>the</strong> synchronisation messages from <strong>the</strong>m to <strong>the</strong> o<strong>the</strong>rdoesn’t happen, th<strong>in</strong>gs get lost, so you end up with patients booked, but we don’tknow about <strong>the</strong>m…We’re gett<strong>in</strong>g a fifty-three, sorry fifty-seven percent error rate at<strong>the</strong> moment” [Director <strong>of</strong> IM & T, Trust 2]“technically I’m not sure that <strong>the</strong>y can deliver it at <strong>the</strong> moment. I don’t th<strong>in</strong>k <strong>the</strong>y’re, Idon’t th<strong>in</strong>k <strong>the</strong>y have <strong>the</strong> architecture <strong>in</strong> place to actually deliver it on a national scale,let alone, actually even a cluster scale, to be honest, so I th<strong>in</strong>k <strong>the</strong>y are struggl<strong>in</strong>gwith it.” [Director <strong>of</strong> IM & T, Trust 4]“somebody, not here, but at <strong>the</strong> PCT level is try<strong>in</strong>g to <strong>in</strong>crease that all <strong>the</strong> time [usageby GPs]…I know that some GPs absolutely hate it and I get <strong>the</strong> impression that<strong>the</strong>y’re us<strong>in</strong>g it under duress and that <strong>the</strong> slightest fault is a case <strong>of</strong> ’Well, what arubbish system, would never work anyway.’” [Chief executive Trust 4]if it doesn’t start deliver<strong>in</strong>g soon people will beg<strong>in</strong> to say it can’t deliver …<strong>the</strong>y, um,<strong>the</strong>y just feel resentment or that it’s irrelevant or, worse still, it looks like moneypoured down <strong>the</strong> dra<strong>in</strong> while <strong>the</strong>y’re hav<strong>in</strong>g to make staff redundant ……<strong>the</strong>n <strong>the</strong>rewill gradually be a sort <strong>of</strong> almost a “We’re go<strong>in</strong>g to make sure it doesn’t work”mentality com<strong>in</strong>g. [Chief executive, Trust 4]5.3. Summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gsThe first round <strong>of</strong> <strong>in</strong>terviews with senior managers and cl<strong>in</strong>icians highlighted fourkey issues:(a) Trusts vary <strong>in</strong> <strong>the</strong>ir circumstances, which affect <strong>the</strong>ir ability to implement <strong>the</strong>NPf<strong>IT</strong>.(b) The process <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> was suboptimal, lead<strong>in</strong>g to low moraleamong <strong>NHS</strong> staff responsible for implementation.(c) The overall timetable for implementation was unrealistic, with Trusts fac<strong>in</strong>gmajor uncerta<strong>in</strong>ties. The need to renew <strong>the</strong> PAS represented a bottleneckand <strong>the</strong> schedule for this activity could not be reconciled with targets forimplementation <strong>of</strong> substantive <strong>IT</strong> applications.75
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 1(d) Short term benefits <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> are unlikely to be sufficient topersuade <strong>NHS</strong> staff to support <strong>the</strong> NPf<strong>IT</strong> unreservedly, particularly if newapplications deliver lower levels <strong>of</strong> functionality.Although it was far too early at <strong>the</strong> time <strong>of</strong> <strong>the</strong>se <strong>in</strong>terviews to assess <strong>the</strong> success<strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>, <strong>the</strong> process <strong>of</strong> implementation was already clearly caus<strong>in</strong>g concern.Unrealistic and shift<strong>in</strong>g timetables, lack <strong>of</strong> consultation and communication withCfH managers, and unperceived short-term benefits was affect<strong>in</strong>g staff morale.In <strong>the</strong> second round <strong>of</strong> <strong>in</strong>terviews, it was clear that <strong>the</strong> NPf<strong>IT</strong> is a highly desirableobjective; <strong>in</strong> l<strong>in</strong>e with <strong>the</strong> National Audit Office report (which was published dur<strong>in</strong>g<strong>the</strong> <strong>in</strong>terven<strong>in</strong>g period), 44 <strong>in</strong>terviewees were enthusiastic about, andoverwhelm<strong>in</strong>gly supportive <strong>of</strong>, <strong>the</strong> goals <strong>of</strong> <strong>the</strong> programme.However, senior Trust staff still raised serious concerns, several <strong>of</strong> which were<strong>the</strong> same as dur<strong>in</strong>g <strong>the</strong> first <strong>in</strong>terviews.Cont<strong>in</strong>u<strong>in</strong>g uncerta<strong>in</strong>ty about <strong>the</strong>programme was mak<strong>in</strong>g key managerial decisions more difficult, given <strong>the</strong> currentneed to make f<strong>in</strong>ancial sav<strong>in</strong>gs and achieve efficiencies.Although <strong>IT</strong> <strong>modernisation</strong> should facilitate <strong>the</strong>se goals <strong>in</strong> <strong>the</strong> longer-term, at <strong>the</strong>time <strong>of</strong> <strong>the</strong> second <strong>in</strong>terviews senior managers still did not know:(a) what <strong>the</strong> local costs <strong>of</strong> implementation will be;(b) when a replacement patient adm<strong>in</strong>istration system compliant with <strong>the</strong>programme will be available;(c) <strong>the</strong> timetable for delivery <strong>of</strong> <strong>in</strong>terim applications;(d) <strong>the</strong> features <strong>of</strong> <strong>the</strong>se applications;(e) <strong>the</strong> likely benefits and efficiencies from new systems.In <strong>the</strong> face <strong>of</strong> <strong>the</strong>se uncerta<strong>in</strong>ties, managers found it difficult to prioritiseimplementation <strong>of</strong> <strong>the</strong> programme.Concern was expressed about threats topatient safety from a ‘patch and mend’ approach to ma<strong>in</strong>ta<strong>in</strong> exist<strong>in</strong>g systems.Trust managers need to be given concrete <strong>in</strong>formation, about implementationtimetables, system compatibility with <strong>the</strong> long term goals <strong>of</strong> <strong>the</strong> programme, andvalue-for-money. Communication generally between CfH and Trusts needs toimprove. F<strong>in</strong>ally, Trusts need assistance to prioritise <strong>IT</strong> <strong>modernisation</strong> aga<strong>in</strong>sto<strong>the</strong>r compet<strong>in</strong>g f<strong>in</strong>ancial pressures, for example by <strong>in</strong>clusion <strong>in</strong> performancemanagement frameworks.76
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 26. Qualitative f<strong>in</strong>d<strong>in</strong>gs from Level 2: implementation <strong>of</strong> specific e-functions6.1. IntroductionAs set out <strong>in</strong> chapter 1, we planned to study <strong>the</strong> implementation <strong>of</strong> three specificfunctions: PACS; CPOE; e-book<strong>in</strong>g. We report here on f<strong>in</strong>d<strong>in</strong>gs from our studies<strong>of</strong> PACS (implemented wholly or partially <strong>in</strong> three Trusts) and CPOE(implemented <strong>in</strong> two Trusts, although can be classed only as attemptedimplementation <strong>in</strong> one), as e-book<strong>in</strong>g had not been implemented widely enough(implemented only partially <strong>in</strong> one Trust).As described <strong>in</strong> chapter 4, <strong>the</strong>se functions were studied us<strong>in</strong>g <strong>the</strong> analyticalframework <strong>of</strong> diffusion <strong>of</strong> <strong>in</strong>novations <strong>the</strong>ory 78 and fur<strong>the</strong>r work by Greenhalgh etal 79 , develop<strong>in</strong>g a conceptual framework for <strong>the</strong> factors <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> diffusionand implementation <strong>of</strong> <strong>in</strong>novations. In this framework, Greenhalgh et al 79 identifyn<strong>in</strong>e <strong>in</strong>teract<strong>in</strong>g elements relat<strong>in</strong>g to, for example, attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation;characteristics <strong>of</strong> <strong>the</strong> adopter; system read<strong>in</strong>ess for <strong>in</strong>novation; implementationprocess, and so on.In this chapter, we outl<strong>in</strong>e <strong>the</strong> background to <strong>the</strong> <strong>IT</strong> applications (<strong>in</strong>novations) and<strong>the</strong>n report on our f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> terms <strong>of</strong> key factors <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong>ir adoption:attributes <strong>of</strong> <strong>the</strong> application; characteristics <strong>of</strong> <strong>the</strong> adopters; implementationprocesses; and organisational factors. We also report on <strong>the</strong> impact <strong>of</strong> <strong>the</strong>implementation <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications. As Greenhalgh et al 79and o<strong>the</strong>rs havenoted, <strong>the</strong>se factors <strong>in</strong>teract with each o<strong>the</strong>r <strong>in</strong> complex ways, for example, <strong>the</strong>attributions <strong>of</strong> <strong>the</strong> <strong>in</strong>novations may affect <strong>the</strong> implementation process which <strong>in</strong>turn affects adoption.6.2. Background to <strong>IT</strong> applications6.2.1. Picture archiv<strong>in</strong>g and communication system (PACS)Broadly, <strong>the</strong>re are two types <strong>of</strong> PACS: computerised radiography whichchanges <strong>the</strong> film cassette <strong>in</strong>to a digital image, and digital radiography (‘true’PACS) which has no film, <strong>the</strong> image be<strong>in</strong>g digital from <strong>the</strong> outset. Digitalradiography is more expensive but more efficient than computerisedradiography. We <strong>in</strong>terviewed 17 end users <strong>in</strong> <strong>the</strong> three Trusts us<strong>in</strong>g PACS (<strong>the</strong>fourth Trust had not implemented it) dur<strong>in</strong>g <strong>the</strong> period January –October 2005.77
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2These end users were us<strong>in</strong>g digital radiography systems. Only one Trust(no.4) had a true PACS system, digital radiography throughout <strong>the</strong> Trust, withno hard film available to staff or used. Staff <strong>in</strong>terviewed from ano<strong>the</strong>r twoTrusts had partial systems <strong>in</strong> place. Trust 2 had PACS throughout one part <strong>of</strong>a new build<strong>in</strong>g on one part <strong>of</strong> spilt site, so digital films were moved aroundcl<strong>in</strong>ics, between staff that worked <strong>in</strong> this new build<strong>in</strong>g, and adjacent build<strong>in</strong>gs,but were not available for view<strong>in</strong>g across o<strong>the</strong>r parts <strong>of</strong> <strong>the</strong> Trust. Trust 3 hadtwo pockets <strong>of</strong> PACS, with just one mach<strong>in</strong>e for digital radiography situated <strong>in</strong>each. This meant staff us<strong>in</strong>g <strong>the</strong>se mach<strong>in</strong>es could take small numbers <strong>of</strong>digital films but <strong>the</strong>se made up a small proportion <strong>of</strong> <strong>the</strong> total x-rays taken.View<strong>in</strong>g could be done from most parts <strong>of</strong> <strong>the</strong> Trust but was limited to <strong>the</strong>small number <strong>of</strong> digital films. All <strong>the</strong>se PACS systems were implemented priorto NPf<strong>IT</strong>. The NPf<strong>IT</strong> is provid<strong>in</strong>g a computerised radiography version <strong>of</strong>PACS. 56,91,92We asked <strong>in</strong>terviewees about <strong>the</strong>ir experiences <strong>of</strong> us<strong>in</strong>g <strong>the</strong>PACS system <strong>the</strong>y had implemented and <strong>the</strong>ir views on implement<strong>in</strong>g <strong>the</strong>NPf<strong>IT</strong> version <strong>of</strong> PACS. PACS was widely used, and extremely popular with<strong>the</strong> end users we <strong>in</strong>terviewed.6.2.2. e-test order<strong>in</strong>g and brows<strong>in</strong>g (CPOE)The systems are different between <strong>the</strong> two Trusts us<strong>in</strong>g this application. InTrust 1, <strong>the</strong> system which went live <strong>in</strong> 2001 is both for order<strong>in</strong>g tests andbrows<strong>in</strong>g. It is very quick and easy to use – takes about 15 seconds to am<strong>in</strong>ute and has clearly laid out <strong>in</strong>structions. In Trust 2, on one hospital site,<strong>the</strong>re are separate systems for e-test order<strong>in</strong>g and brows<strong>in</strong>g, bothimplemented <strong>in</strong> 2002, which replaced a previous DOS-based e-testorder<strong>in</strong>g/brows<strong>in</strong>g system. While <strong>the</strong> DOS-based system had been used by<strong>the</strong> majority <strong>of</strong> staff, <strong>the</strong> current e-test order<strong>in</strong>g system is used only by am<strong>in</strong>ority <strong>of</strong> staff. Most staff use <strong>the</strong> brows<strong>in</strong>g system.We <strong>in</strong>terviewed 21 staff <strong>in</strong> <strong>the</strong>se two Trusts dur<strong>in</strong>g <strong>the</strong> period January toOctober 2005.78
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 26.3. F<strong>in</strong>d<strong>in</strong>gsWe present our f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> terms <strong>of</strong> four ma<strong>in</strong> factors which <strong>in</strong>fluence <strong>the</strong> adoption<strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications: attributes <strong>of</strong> <strong>the</strong> application; characteristics <strong>of</strong> <strong>the</strong>adopter; implementation processes; organisational factors. F<strong>in</strong>ally, we present <strong>the</strong>impact <strong>of</strong> <strong>the</strong> different <strong>IT</strong> applications, although <strong>the</strong>se also, <strong>in</strong> turn, affect howwidely <strong>the</strong> application is adopted.6.3.1. Attributes <strong>of</strong> <strong>the</strong> <strong>IT</strong> applicationAs o<strong>the</strong>rs have found, <strong>the</strong> attributes <strong>of</strong> <strong>the</strong> <strong>IT</strong> application are very important <strong>in</strong><strong>in</strong>fluenc<strong>in</strong>g its rate <strong>of</strong> adoption. These <strong>in</strong>clude ease and speed <strong>of</strong> use,reliability, ability to customise, and compatibility with exist<strong>in</strong>g practices.i) Speed/ease <strong>of</strong> use/reliabilityPACS was perceived by many users as fast, easy to use, and reliable – as <strong>the</strong>follow<strong>in</strong>g quotes from Trust 4, which had ‘full’ PACS, illustrate:“<strong>the</strong> systems were so user-friendly, so easy to work, people enjoyed us<strong>in</strong>g it,so we didn’t have any major problems” [PACS tra<strong>in</strong>er, Trust 4].“It was remarkably quick (to learn) and people felt pleased with <strong>the</strong>mselveshav<strong>in</strong>g been able to, to master it” [Radiologist and PACS lead, Trust 4].“If <strong>the</strong>re’s a doctor who hasn’t worked here before I can show <strong>the</strong>m how to useit very quickly” [Adm<strong>in</strong>istrator, Trust 4].This experience at Trust 4 contrasted with that <strong>of</strong> Trust 2 where users foundPACS more time-consum<strong>in</strong>g than analogue film. This was because only apartial PACS system had been implemented so that view<strong>in</strong>g could only takeplace across part <strong>of</strong> <strong>the</strong> site and staff mov<strong>in</strong>g around <strong>the</strong> site had to use morethan one system.The experience between <strong>the</strong> two Trusts us<strong>in</strong>g different systems <strong>of</strong> e-testorder<strong>in</strong>g and brows<strong>in</strong>g illustrates <strong>the</strong> importance <strong>of</strong> <strong>the</strong> usability <strong>of</strong> <strong>the</strong> <strong>IT</strong>application. In Trust 1 where <strong>the</strong> systems were perceived as easy to use andtime-sav<strong>in</strong>g, <strong>the</strong>re has been much greater adoption than at Trust 2 whereorder<strong>in</strong>g <strong>in</strong> particular has had a slow rate <strong>of</strong> adoption because it is very hard touse:79
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2“for new members <strong>of</strong> staff, um, even with <strong>the</strong> best will <strong>in</strong> <strong>the</strong> world, for <strong>the</strong> firstcouple <strong>of</strong> weeks <strong>the</strong>y are function<strong>in</strong>g at about fifty percent <strong>of</strong> what somebodyelse is” [Senior cl<strong>in</strong>ician, Trust 2].ii) Ability to customize/compatibility with exist<strong>in</strong>g practicesOne important attribute for e-test order<strong>in</strong>g was <strong>the</strong> ability to customize. InTrust 1, <strong>the</strong>y have been able to customise <strong>the</strong>ir orders:“we <strong>in</strong>troduced rules…. <strong>the</strong>se tests would be ordered and with a bit <strong>of</strong> jiggerypokery it works and it cont<strong>in</strong>ues to work and that makes a real difference sothat I know that all <strong>the</strong> tests will be done on our patients when <strong>the</strong>y come to<strong>in</strong>tensive care. There were one or two funny glitches, but essentially itworked” [Cl<strong>in</strong>ician, Trust 1].In Trust 2, however, <strong>the</strong> system <strong>of</strong> e-test order<strong>in</strong>g was not perceived ascompatible with exist<strong>in</strong>g practices and <strong>the</strong>refore rate <strong>of</strong> adoption has beenslow:“it’s not <strong>in</strong>tuitive as to who does <strong>the</strong> test, so you may have to go <strong>in</strong>to extensivelaboratory menus to try and identify what <strong>the</strong> test is… and I could spend agestry<strong>in</strong>g to look through to f<strong>in</strong>d out where…more <strong>of</strong>ten what I may end up do<strong>in</strong>gis I’ll ei<strong>the</strong>r have to phone somebody to f<strong>in</strong>d out… Or else I just default us<strong>in</strong>g apiece <strong>of</strong> paper. So for unusual tests or for even th<strong>in</strong>gs that are slightlyunusual, <strong>the</strong> th<strong>in</strong>gs that I don’t know where <strong>the</strong>y are it can take too long to go.There’s a second problem, um, <strong>in</strong> nam<strong>in</strong>g <strong>of</strong> tests <strong>the</strong>re’s no standardisedmechanism <strong>of</strong> nam<strong>in</strong>g <strong>of</strong> tests. …could be that <strong>the</strong>y’re listed alphabetically,um, if I wanted to do fast<strong>in</strong>g lipids, um, I don’t, it may be <strong>in</strong> under ‘f’ for fast<strong>in</strong>glipid or it could be <strong>in</strong> for lipid, bracket, fast<strong>in</strong>g or it could be <strong>in</strong> under cholec ‘c’for cholesterol, plus ……brackets, fast<strong>in</strong>g” [Senior Cl<strong>in</strong>ician, Trust 2].6.3.2. Characteristics <strong>of</strong> <strong>the</strong> AdoptersWhe<strong>the</strong>r or not <strong>the</strong>re were positive attributes <strong>of</strong> <strong>the</strong> <strong>IT</strong> application, <strong>the</strong>re weredifficulties <strong>in</strong> <strong>the</strong> <strong>in</strong>itial implementation stage. These <strong>in</strong>cluded potentialadopters’ concerns prior to implementation <strong>of</strong> each <strong>of</strong> <strong>the</strong> applications,particularly from those not used to us<strong>in</strong>g computers. One <strong>in</strong>tervieweesummarised o<strong>the</strong>rs’ views on resistance from, for example,“consultants who are liv<strong>in</strong>g <strong>in</strong> <strong>the</strong> dark ages.. I call <strong>the</strong> quill and <strong>in</strong>kwellbrigade, who don’t know what a PC looks like and <strong>the</strong>y’re frightened” [PACSmanager, Trust 3].80
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2There was <strong>in</strong>itially a lack <strong>of</strong> belief <strong>in</strong> <strong>the</strong> <strong>IT</strong> application from some preimplementation,and subsequently difficulties <strong>in</strong> mak<strong>in</strong>g <strong>the</strong> transition from onesystem to ano<strong>the</strong>r:“orthopaedic consultants have <strong>in</strong>dicated already that <strong>the</strong>y don’t believe thatimages will be as good…you need that really high resolution <strong>of</strong> pla<strong>in</strong> film forbone….so traditionally orthopaedics departments can be awkward…<strong>the</strong>y liketo draw pictures on pre and post…”[PACS project manager, Trust 2].“<strong>the</strong> clerical staff were a different issue, it took <strong>the</strong>m longer to accept, accept<strong>the</strong>y had to use it and <strong>the</strong>y were a bit wary <strong>of</strong> it and <strong>the</strong>y didn’t really like itbecause it was a lot different to what <strong>the</strong>y used to been do<strong>in</strong>g” [PACS tra<strong>in</strong>er,Trust 2].“Transition period was a bit difficult…we still wanted to look at <strong>the</strong> old x-raysas <strong>the</strong> well as <strong>the</strong> ones that were on <strong>the</strong> computer” [Adm<strong>in</strong>istrator, Trust 4].“We’re had our problems with PACS…we had loads and loads <strong>of</strong> problemswith <strong>the</strong> archive, with <strong>the</strong> workflow and everyth<strong>in</strong>g, um, until we got it right…Ith<strong>in</strong>k for about a year it was difficult” [PACS tra<strong>in</strong>er, Trust 4]The characteristics <strong>of</strong> <strong>the</strong> adopters did not rema<strong>in</strong> fixed, however, and <strong>the</strong>rewere changes over time as <strong>IT</strong> applications <strong>in</strong>novations were implemented. Theattributes <strong>of</strong> <strong>the</strong> application <strong>in</strong>fluenced how <strong>the</strong> adopters viewed it, andsimilarly <strong>the</strong> processes <strong>of</strong> implementation affected how potential usersadopted <strong>the</strong> application, or not.6.3.3. Implementation processesImportant factors here were <strong>the</strong> levels <strong>of</strong> user consultation and <strong>in</strong>volvement,quality <strong>of</strong> tra<strong>in</strong><strong>in</strong>g and <strong>IT</strong> support, and a ‘critical mass’ <strong>of</strong> implementation.The level <strong>of</strong> user consultation and <strong>in</strong>volvement varied between <strong>IT</strong> applicationsand Trusts. There were criticisms <strong>of</strong> <strong>the</strong> lack <strong>of</strong> <strong>in</strong>volvement <strong>in</strong> CPOE systems<strong>in</strong> Trust 2 with key staff groups:“it comes back to <strong>the</strong> importance <strong>of</strong> br<strong>in</strong>g<strong>in</strong>g on cl<strong>in</strong>icians right at <strong>the</strong> beg<strong>in</strong>n<strong>in</strong>g<strong>of</strong> design<strong>in</strong>g <strong>the</strong> system <strong>in</strong> that <strong>the</strong>y’re <strong>the</strong> people that have to use it and<strong>the</strong>y’re <strong>the</strong> more, <strong>the</strong> most important people. You know, <strong>the</strong>ir ideas are notgo<strong>in</strong>g to be <strong>the</strong> same as some <strong>IT</strong> bod sat <strong>in</strong> a room design<strong>in</strong>g it” [<strong>IT</strong> tra<strong>in</strong>er,Trust 2].Whereas <strong>in</strong> Trust 1, <strong>the</strong>y had carried out some user consultation on adapt<strong>in</strong>g<strong>the</strong> e-test order<strong>in</strong>g system to <strong>the</strong>ir needs:81
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2“<strong>the</strong>y wanted our f<strong>in</strong>al <strong>in</strong>put as to were we happy with everyth<strong>in</strong>g, all <strong>the</strong> teststhat were on <strong>the</strong>re, um, aspects <strong>of</strong> how <strong>the</strong>y order? Did we want any rules <strong>in</strong>?For example, so <strong>the</strong>re’s some tests that have got certa<strong>in</strong> rules attached to<strong>the</strong>m that prevent you from order<strong>in</strong>g <strong>the</strong>m or if it’s <strong>in</strong>appropriate or that comeup with warn<strong>in</strong>gs say<strong>in</strong>g that, you know ’This needs to be discussed with, youknow, a haematology consultant before it actually can be analysed‘ orsometh<strong>in</strong>g like that. So we were, we were <strong>in</strong>volved <strong>in</strong> that side <strong>of</strong> th<strong>in</strong>gs”[Senior Cl<strong>in</strong>ician, Trust 1].The quality and amount <strong>of</strong> tra<strong>in</strong><strong>in</strong>g, as well as <strong>IT</strong> support, also differedbetween Trusts. The PACS systems seem to require less <strong>in</strong>tensive tra<strong>in</strong><strong>in</strong>g, as<strong>the</strong>y are easier to use, however, on-go<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g with new staff, particularlyjunior doctors is important. Tra<strong>in</strong><strong>in</strong>g, both <strong>in</strong>itial and on-go<strong>in</strong>g, is criticised <strong>in</strong>both Trusts with e-test order<strong>in</strong>g and brows<strong>in</strong>g:“we have a reasonable turnover <strong>of</strong> staff and a new staff member may appear,um, <strong>the</strong>y have to go for tra<strong>in</strong><strong>in</strong>g, um, <strong>the</strong> nearest next date for <strong>the</strong>ir tra<strong>in</strong><strong>in</strong>gmay be ten days away… and for ten days <strong>the</strong>y’re work<strong>in</strong>g at a majordisadvantage <strong>in</strong> that <strong>the</strong>y have to use paper, um, so <strong>the</strong>y get to sort <strong>of</strong> learnhow <strong>the</strong> cl<strong>in</strong>ic runs, but us<strong>in</strong>g what, us<strong>in</strong>g a strategy that <strong>the</strong>y <strong>the</strong>n have tounlearn” [Senior cl<strong>in</strong>ician, Trust 2].“one <strong>of</strong> our significant issues is that we, new medical staff, for <strong>in</strong>stance, <strong>the</strong>re’sonly a two hour slot for tra<strong>in</strong><strong>in</strong>g <strong>the</strong>m on EPR…I mean we have certa<strong>in</strong>ly gotsome ……tra<strong>in</strong><strong>in</strong>g and <strong>the</strong> sort <strong>of</strong> local support, but I mean it isn’t, it isn’t asgreat as it might, as it might be” [Project manager, test order<strong>in</strong>g, Trust 1].<strong>IT</strong> support <strong>in</strong> <strong>the</strong> form <strong>of</strong> responsive helpdesks accessible 24 hours a day is animportant element <strong>of</strong> <strong>the</strong> implementation process:“You r<strong>in</strong>g <strong>the</strong> helpdesk, you’re on hold for ten m<strong>in</strong>utes, um, <strong>the</strong>y will say “Don’tknow, I’ll have a look at it, call you back later” which <strong>the</strong>y never do” [Cl<strong>in</strong>ician,Trust 2].“I said ’Well look, we have locums who turn up at five o’clock <strong>in</strong> <strong>the</strong> even<strong>in</strong>g towork on <strong>in</strong>tensive care, to work on <strong>the</strong> wards, <strong>the</strong>y’ve got to be able to access<strong>the</strong> system.’ Then <strong>the</strong>y said ’Oh, well we’ll have somebody on site to tra<strong>in</strong><strong>the</strong>m.’ Well <strong>the</strong>y don’t have people on site to tra<strong>in</strong> <strong>the</strong>m. And <strong>the</strong>n <strong>the</strong>y said’Well, we’ll give <strong>the</strong>m a temporary password.’ And so what actually happensis that people give <strong>the</strong>m out, somebody, <strong>the</strong> person <strong>the</strong>y’re tak<strong>in</strong>g over fromgives <strong>the</strong>m <strong>the</strong>ir password. Well, you know, that <strong>the</strong> <strong>IT</strong> people say ’Well thatmust never ever happen.’ But <strong>the</strong>re is, <strong>the</strong>re is a lack <strong>of</strong> understand<strong>in</strong>g by <strong>the</strong><strong>IT</strong> people <strong>of</strong> how hospitals work” [Cl<strong>in</strong>ician, Trust 1].F<strong>in</strong>ally, achiev<strong>in</strong>g a critical mass <strong>of</strong> implementation i.e. implement<strong>in</strong>g <strong>the</strong> <strong>IT</strong>application widely enough so that it is worthwhile for staff to use it is important.For example, <strong>in</strong> Trust 4, <strong>the</strong> PACS lead, a radiologist, stated:82
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2“<strong>in</strong> order to complete that functional loop we have to also put <strong>the</strong>, um, PACS<strong>in</strong>to <strong>the</strong> orthopaedic cl<strong>in</strong>ics and <strong>in</strong>to <strong>the</strong>atre” [Radiologist and PACS lead,Trust 4].Related to this issue <strong>of</strong> critical mass is also reduc<strong>in</strong>g access to alternatives sothat users have to switch to <strong>the</strong> <strong>IT</strong> application:“hardest part also is to make sure that you’re not pr<strong>in</strong>t<strong>in</strong>g films… have to bevery, very strong to say ’I’m not pr<strong>in</strong>t<strong>in</strong>g films, you’ve got to look at th<strong>in</strong>gs onPACS.’” [PACS tra<strong>in</strong>er, Trust 4]6.3.4. Organisational factorsIn addition to <strong>the</strong> implementation processes outl<strong>in</strong>ed above, <strong>the</strong>re are anumber <strong>of</strong> organisational factors which had ei<strong>the</strong>r a positive or negativeimpact on <strong>the</strong> adoption <strong>of</strong> <strong>the</strong>se particular <strong>IT</strong> applications. These <strong>in</strong>cludedawareness <strong>of</strong> <strong>the</strong> ‘bus<strong>in</strong>ess process’ <strong>in</strong> <strong>the</strong> design <strong>of</strong> <strong>the</strong> application; <strong>the</strong>presence <strong>of</strong> a strong project management team; and <strong>the</strong> level <strong>of</strong> <strong>the</strong> ability <strong>of</strong><strong>the</strong> organization to work as a whole and <strong>in</strong> teams, ra<strong>the</strong>r than disparate units.i) Awareness <strong>of</strong> <strong>the</strong> bus<strong>in</strong>ess processesAn important factor <strong>in</strong> <strong>the</strong> adoption <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications was how far thosedesign<strong>in</strong>g and implement<strong>in</strong>g <strong>the</strong>m understood <strong>the</strong> nature <strong>of</strong> ‘<strong>the</strong> bus<strong>in</strong>ess’ <strong>the</strong>ywere design<strong>in</strong>g for. There were contrast<strong>in</strong>g experiences <strong>of</strong> this <strong>in</strong> terms <strong>of</strong> e-test order<strong>in</strong>g <strong>in</strong> Trust 1 and 2.“I th<strong>in</strong>k this company was totally unaware <strong>of</strong> how, what <strong>the</strong> cl<strong>in</strong>icians wanted,ei<strong>the</strong>r that or <strong>the</strong>y couldn’t produce what we wanted. We got quite a lot <strong>of</strong>noise around here <strong>in</strong> <strong>the</strong> sense that <strong>the</strong>y couldn’t produce what we wanted… Idon’t th<strong>in</strong>k <strong>the</strong>y had <strong>the</strong> technical know-how... was <strong>the</strong> impression we had,<strong>the</strong>y couldn’t actually do what was required to produce a user-friendly order<strong>in</strong>gsystem” [Senior cl<strong>in</strong>ician, Trust 2].“The test order<strong>in</strong>g is one <strong>of</strong> <strong>the</strong> systems that works well here, it’s been aroundor quite a while. Um, <strong>the</strong> guy that runs it is <strong>in</strong>tegrated <strong>in</strong>to <strong>the</strong> bus<strong>in</strong>ess aswell, he’s, he’s not just a technologist, he follows <strong>the</strong> bus<strong>in</strong>ess process as well.So that works well for us” [Junior doctor, Trust 1].However, not everyone at Trust 1 shared this view:“one <strong>of</strong> <strong>the</strong> o<strong>the</strong>r th<strong>in</strong>gs which I th<strong>in</strong>k could be done slicker by a Trustorganisation because you have people work<strong>in</strong>g to a test script that <strong>the</strong>y don’tnecessarily understand <strong>the</strong> bus<strong>in</strong>ess logic beh<strong>in</strong>d. …to give you, give you an83
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2example, um, I had one <strong>of</strong> <strong>the</strong>ir bus<strong>in</strong>ess analysts say “We’ve been runn<strong>in</strong>gthis test script on a particular test and we’re gett<strong>in</strong>g a funny answer.” When Ilooked through <strong>the</strong> test script and I said “Well <strong>the</strong> reason why you’re hav<strong>in</strong>g anissue is that we would never report that particular value <strong>in</strong> that way” [Projectmanager, test order<strong>in</strong>g, Trust 1].“what happens a lot <strong>of</strong> <strong>the</strong> time too is you get a technology solution and all<strong>the</strong>se technology people say ’This is <strong>the</strong> way you’ve got to do it.’ What <strong>the</strong>ydon’t do is consult <strong>the</strong> bus<strong>in</strong>ess and say “This is <strong>the</strong> way <strong>the</strong> bus<strong>in</strong>ess has towork now for <strong>NHS</strong> cl<strong>in</strong>ical practice.” This is <strong>the</strong> way <strong>the</strong>y have to work now t<strong>of</strong>it <strong>in</strong> with <strong>the</strong> system” [House <strong>of</strong>ficer, Trust 1].ii) Strong project management team with high level management supportIt was widely recognized that implementation <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications requiresvery strong project management which is supported at a high level <strong>of</strong>management with<strong>in</strong> <strong>the</strong> organisation.“my experience has been <strong>the</strong> top down directives, if it’s not supported bysomeone from <strong>the</strong> top <strong>the</strong>re’s no po<strong>in</strong>t <strong>in</strong> do<strong>in</strong>g it. If it’s handed to, if it’s a taskhanded to a junior project manager or somebody like that it’s got no authorityto make people use <strong>the</strong> system and it just becomes ano<strong>the</strong>r system thatmakes <strong>the</strong> <strong>IT</strong> environment more complex and wastes everybody’s time andeffort” [EPR implementation manager, Trust 1]“A lot <strong>of</strong> credit should go to [name <strong>of</strong> person] because he was at cl<strong>in</strong>icaldirectorship level and he’s a very forward th<strong>in</strong>k<strong>in</strong>g guy, which made him, orforced him or gave him <strong>the</strong> possibilities to work very closely with o<strong>the</strong>r high uppeople…he already had that work<strong>in</strong>g relationship with <strong>the</strong> directorate and Ith<strong>in</strong>k that helped a lot….whole team was beh<strong>in</strong>d him and trusted him”[Radiographer, Trust 4].“<strong>the</strong> management cha<strong>in</strong> is very short and very close…with<strong>in</strong> this directorate it,it’s excellent…extremely close work<strong>in</strong>g relationships” [Radiologist, Trust 3].“I don’t th<strong>in</strong>k <strong>the</strong>re’s anybody <strong>in</strong> [<strong>the</strong> <strong>IT</strong> company] now here who was, who washere at <strong>the</strong> beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> <strong>the</strong> project…<strong>the</strong>re is nobody left who had anyth<strong>in</strong>g todo with this implementation” [PACS project manager, Trust 2].“<strong>the</strong>y had people that were go<strong>in</strong>g to put <strong>in</strong> this NPf<strong>IT</strong> stuff that had absolutelyno experience <strong>in</strong> project management whatsoever and no changemanagement experience …… <strong>the</strong>y really couldn’t grasp <strong>the</strong> impact that <strong>the</strong>seth<strong>in</strong>gs were go<strong>in</strong>g to have on <strong>the</strong>, on <strong>the</strong> organisation and that seems to befairly ……<strong>the</strong> <strong>NHS</strong>. …Um, a lot <strong>of</strong> <strong>the</strong> Trusts need to reth<strong>in</strong>k have <strong>the</strong>y <strong>the</strong>resource for <strong>the</strong>se sort <strong>of</strong> projects. I th<strong>in</strong>k hav<strong>in</strong>g <strong>in</strong>experienced people is justdest<strong>in</strong>ed to failure” [EPR implementation manager, Trust 1].84
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2iii) Level <strong>of</strong> organisational unity and teamworkThis po<strong>in</strong>t relates to <strong>the</strong> importance <strong>of</strong> team work<strong>in</strong>g both with<strong>in</strong> and betweendepartments, and <strong>the</strong> ability <strong>of</strong> <strong>the</strong> organisation to work as a whole toimplement <strong>the</strong>se <strong>IT</strong> applications. There seemed to be more examples <strong>of</strong> this <strong>in</strong>Trust 4 than <strong>the</strong> o<strong>the</strong>r three Trusts, which may be at least <strong>in</strong> part because as as<strong>in</strong>gle-site hospital this process is easier.“This whole journey is what needs to be looked at and it’s a mistake to justlook purely from a ra<strong>the</strong>r selfish viewpo<strong>in</strong>t”[Radiologist and PACS lead, Trust4]“<strong>the</strong>y [staff] were not an audience, <strong>the</strong>y were actually part <strong>of</strong> <strong>the</strong> decisionmak<strong>in</strong>gprocess” [Radiographer, Trust 4]“everybody we worked as a team toge<strong>the</strong>r, attend<strong>in</strong>g meet<strong>in</strong>g toge<strong>the</strong>r and<strong>the</strong>y were m<strong>in</strong>uted…..if we are not part <strong>of</strong> <strong>the</strong> team all <strong>the</strong> work that you do isnot go<strong>in</strong>g to be, you don’t achieve anyth<strong>in</strong>g…You have to work, um, as agroup and communicate” [PACS Tra<strong>in</strong>er, Trust 4]“It’s important to have a multi-team approach, holistic approach whenconsult<strong>in</strong>g staff” [Radiologist, Trust 3].“<strong>the</strong>re’s quiet a lot <strong>of</strong> examples <strong>of</strong> where one party’s <strong>in</strong>terest actually conflictedwith ano<strong>the</strong>r’s and it depends on who’s got more political weight as to whogets what, who moves forward and who doesn’t and quite <strong>of</strong>ten <strong>the</strong> ones thatdon’t have, um, a big voice so to speak, end up with <strong>the</strong> burden… <strong>the</strong>re’sprobably no-one <strong>in</strong> this Trust at <strong>the</strong> moment that has a good holistic view <strong>of</strong><strong>the</strong> requirements and th<strong>in</strong>gs <strong>of</strong> all <strong>the</strong> different departments and that’ssometh<strong>in</strong>g that’s been addressed at <strong>the</strong> moment as well” [EPR implementationmanager, Trust 1]“Well, it’s not been an easy situation all told because obviously as well <strong>the</strong>re’sbeen a certa<strong>in</strong> element <strong>of</strong> feel<strong>in</strong>g between <strong>the</strong> sites <strong>in</strong> so much as one site hasgot a brand new hospital, <strong>the</strong> o<strong>the</strong>r one has got one that needs completelyredevelop<strong>in</strong>g….<strong>the</strong> sort <strong>of</strong> <strong>the</strong> staff <strong>of</strong> <strong>the</strong> Trust generally haven’t reallyparticularly knitted toge<strong>the</strong>r as one organization” [EPR tra<strong>in</strong>er, Trust 1].6.3.5. Impact <strong>of</strong> implement<strong>in</strong>g <strong>IT</strong> applicationsAs shown <strong>in</strong> <strong>the</strong> quantitative analysis (see chapter 7), <strong>the</strong> impact <strong>of</strong> <strong>the</strong>se <strong>IT</strong>applications was relatively limited because <strong>the</strong> implementation was limited.The impact <strong>of</strong> implement<strong>in</strong>g <strong>the</strong>se applications related to <strong>the</strong> follow<strong>in</strong>g areas:patient experience; work<strong>in</strong>g practices; and safety/governance. In all cases,<strong>the</strong>re were positive and negative examples <strong>of</strong> <strong>the</strong>se reported, but overall, forPACS <strong>in</strong> all three Trusts and e-test order<strong>in</strong>g <strong>in</strong> Trust 1, <strong>the</strong> positives appear tooutweigh <strong>the</strong> negatives. Hav<strong>in</strong>g said that, very little formal measurement <strong>of</strong>85
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2<strong>the</strong>se consequences was carried out by <strong>the</strong> Trusts, for example, <strong>the</strong> reported<strong>in</strong>crease <strong>in</strong> <strong>the</strong> numbers <strong>of</strong> tests follow<strong>in</strong>g implementation <strong>of</strong> e-test order<strong>in</strong>gwas not quantified by Trust 1.These consequences are important, not least because <strong>the</strong> perceived positiveand negative impact <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> <strong>IT</strong> application <strong>in</strong>fluenced cont<strong>in</strong>ueduse <strong>of</strong> <strong>the</strong> application and wider adoption.i) Impact on patient experienceIn terms <strong>of</strong> patient experience, improvements from PACS cited <strong>in</strong>cluded lowerradiation doses result<strong>in</strong>g from fewer repeat x-rays because fewer lost images,reduced wait<strong>in</strong>g times dur<strong>in</strong>g <strong>the</strong> period <strong>of</strong> <strong>the</strong> patient’s appo<strong>in</strong>tment,<strong>in</strong>creased <strong>in</strong>formation for patients as <strong>the</strong>y can see <strong>the</strong>ir x-ray image on <strong>the</strong>computer screen, and <strong>in</strong>novation now perceived as ‘essential’ to <strong>the</strong>diagnostic part <strong>of</strong> <strong>the</strong> patient pathway by respondents at all three Trusts.“PACS is someth<strong>in</strong>g that has moved from be<strong>in</strong>g an <strong>in</strong>novation toy to critical to<strong>the</strong> pathway <strong>of</strong> evaluation <strong>of</strong> a patient” [Radiologist and PACS lead, Trust 4].“<strong>in</strong> <strong>the</strong> past <strong>the</strong>re was that k<strong>in</strong>d <strong>of</strong> wait<strong>in</strong>g, ei<strong>the</strong>r for <strong>the</strong> films or <strong>the</strong> filmpackets…<strong>the</strong> patient just goes straight back now, get registered, has <strong>the</strong> x-rayand <strong>the</strong>n <strong>of</strong>f <strong>the</strong>y go back to <strong>the</strong> cl<strong>in</strong>ic” [PACS tra<strong>in</strong>er, Trust 4].“many patients actually like <strong>the</strong> concept <strong>of</strong> see<strong>in</strong>g what’s wrong with <strong>the</strong>m and<strong>the</strong>y can understand” [Radiologist and PACS lead, Trust 4].“it’s much less remote… [patients can] sit <strong>the</strong>re side by side with <strong>the</strong>ir cl<strong>in</strong>icianand discuss various th<strong>in</strong>gs” [Radiologist and PACS lead, Trust 4]Positive impacts on patient experience were reported where e-test order<strong>in</strong>g iswork<strong>in</strong>g well at Trust 1, but where <strong>the</strong> e-test order<strong>in</strong>g system is not work<strong>in</strong>gwell at Trust 2, negative effects on patient experience were reported. Forexample, doctors reported that because <strong>of</strong> <strong>the</strong> complexity <strong>of</strong> <strong>the</strong> system, <strong>the</strong>yhave to <strong>in</strong>teract with a computer screen for long periods <strong>of</strong> time dur<strong>in</strong>g aconsultation, result<strong>in</strong>g <strong>in</strong> less eye-contact with <strong>the</strong> patient.ii) Impact on work<strong>in</strong>g practicesWe had anticipated that we would have more significant f<strong>in</strong>d<strong>in</strong>gs relat<strong>in</strong>g tochanges <strong>in</strong> work<strong>in</strong>g practices had <strong>the</strong>re been more widespread86
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2implementation <strong>of</strong> <strong>IT</strong> applications. However, <strong>the</strong>re were reportedimprovements to work<strong>in</strong>g practices for both PACS and where e-test order<strong>in</strong>gand brows<strong>in</strong>g has worked well, <strong>the</strong>se <strong>in</strong>cluded improved workflow andimproved communication between pr<strong>of</strong>essionals:“you can have multiple teams look<strong>in</strong>g at <strong>the</strong>ir images at <strong>the</strong> same time” [PACSproject manager, Trust 2]CPOE significantly reduced report<strong>in</strong>g time as reported by Trust 1:“th<strong>in</strong>gs that used to have a three day turnaround time are now com<strong>in</strong>g out <strong>in</strong>,<strong>the</strong>y’re gett<strong>in</strong>g back <strong>in</strong> forty m<strong>in</strong>utes” [Project manager, test order<strong>in</strong>g, Trust 1].And it“will save cl<strong>in</strong>icians’ time as well as nurses’ time because <strong>the</strong> nurses aren’twait<strong>in</strong>g for <strong>the</strong> doctors to come, <strong>the</strong> doctors aren’t wait<strong>in</strong>g, <strong>the</strong>y’re not hav<strong>in</strong>gto juggle <strong>the</strong>ir work and prioritise, you know, and hav<strong>in</strong>g to do, come and take,take <strong>the</strong> blood and order it immediately” [Tra<strong>in</strong>er, e test order<strong>in</strong>g, Trust 1].“but ano<strong>the</strong>r advantage it has now got is, um, specialist nurses have now gotsome order<strong>in</strong>g privileges, which means that it does make it more convenientfor <strong>the</strong> patient because it’s <strong>of</strong>ten <strong>the</strong> nurse that’s draw<strong>in</strong>g <strong>the</strong> blood, um, sopatients can actually have tests when <strong>the</strong>y’re needed. Ra<strong>the</strong>r than hav<strong>in</strong>g towait for a doctor to come and take it <strong>the</strong> nurse can actually <strong>in</strong>itiate patient carequicker” [Ward sister, Trust 1].Trust 1 also reported that this <strong>IT</strong> application reduced <strong>the</strong> number <strong>of</strong> duplicatetests ordered, although <strong>the</strong>y were not able to quantify this.Many PACS users reported that decision-mak<strong>in</strong>g had improved, for example,“we can now screen those letters, pull up <strong>the</strong> x-ray at <strong>the</strong> same time…make adecision as to how urgent we need to see <strong>the</strong> patient based on thatpicture…now we have old films on <strong>the</strong> system …you can pull up two films andcompare” [Senior cl<strong>in</strong>ician, Trust 4].And fewer lost films resulted <strong>in</strong> fewer repeat x-rays as noted above which hasbenefits for both patients and <strong>the</strong> hospital.In Trust 1 some improvements to <strong>the</strong> work<strong>in</strong>g environment were reported:“it makes <strong>the</strong> job more enjoyable from that po<strong>in</strong>t <strong>of</strong> view because it takesnurs<strong>in</strong>g on that bit fur<strong>the</strong>r ra<strong>the</strong>r than just, just <strong>the</strong> actual nurs<strong>in</strong>g side <strong>of</strong> it. It’s,it’s all part <strong>of</strong> be<strong>in</strong>g a team, a team approach to look<strong>in</strong>g after, after <strong>the</strong> patient”[Ward sister, Trust 1].However, some disadvantages to <strong>the</strong> <strong>IT</strong> applications were reported. Trust 1reported that CPOE had resulted <strong>in</strong> an <strong>in</strong>crease <strong>in</strong> <strong>the</strong> number <strong>of</strong> orders:87
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2“we are f<strong>in</strong>d<strong>in</strong>g that because it’s so easy to place orders for some, to becollected when you’re not <strong>the</strong>re, that we’re see<strong>in</strong>g quite a high <strong>in</strong>crease, well,we’ve seen a high <strong>in</strong>crease which we’ve not really been able to control”[Project manager, test order<strong>in</strong>g, Trust 1].In Trust 2, however, <strong>the</strong> CPOE system was reported as be<strong>in</strong>g slower than <strong>the</strong>previous system result<strong>in</strong>g <strong>in</strong> <strong>in</strong>creas<strong>in</strong>g <strong>in</strong>efficiencies and a decl<strong>in</strong>e <strong>in</strong>relationships between cl<strong>in</strong>ical staff and laboratory staff.iii) Safety/cl<strong>in</strong>ical governanceBoth <strong>IT</strong> applications were perceived to improve safety <strong>in</strong> various ways,however some examples <strong>of</strong> decreases <strong>in</strong> safety were also cited.In Trust 1, <strong>the</strong>re was widespread report<strong>in</strong>g <strong>of</strong> e-test order<strong>in</strong>g and brows<strong>in</strong>gresult<strong>in</strong>g <strong>in</strong> a reduction <strong>in</strong> errors. These <strong>in</strong>cluded fewer patient identificationerrors and staff hav<strong>in</strong>g to take more responsibility for <strong>the</strong>ir work because it isrecorded electronically:“people are more responsible for <strong>the</strong>ir own work. You know, that <strong>the</strong>y knowthat if it’s done electronically <strong>the</strong>re is a record, you know, and that can’t bedenied” [EPR tra<strong>in</strong>er, Trust 1].“<strong>the</strong>y can’t cover up <strong>the</strong>ir mistakes, <strong>the</strong>y can’t cover <strong>the</strong>m up, is <strong>the</strong> answer tothat, <strong>the</strong>y can’t cover up a mistake, but <strong>the</strong>y are, <strong>the</strong>y have to be moreresponsible” [EPR tra<strong>in</strong>er, Trust 1].Most <strong>in</strong>terviewees viewed PACS as contribut<strong>in</strong>g to improved patient safety, forexample, <strong>in</strong> terms <strong>of</strong> improv<strong>in</strong>g quality control and provid<strong>in</strong>g better security:“you have better evidence, so you are polic<strong>in</strong>g <strong>the</strong> quality control better thanyou could” [Radiographer, Trust 4].“Now <strong>the</strong>y have a situation where <strong>the</strong>y cannot get rid <strong>of</strong> an image so <strong>the</strong>y haveto decide whe<strong>the</strong>r <strong>the</strong>y send it to PACS so it will be see by a cl<strong>in</strong>ician dur<strong>in</strong>greport<strong>in</strong>g so he will know that <strong>the</strong>y passed through a bad image…<strong>the</strong>y haveevidence, you have evidence that a particular person is send<strong>in</strong>g more to <strong>the</strong>b<strong>in</strong> than anybody else” [Radiographer, Trust 4]“data-wise it’s been fantastic for security…<strong>the</strong>re was always <strong>the</strong> ability <strong>of</strong>people to walk <strong>in</strong> and maybe pick up a film and look at it, but with PACS yousimply can’t do that” [EPR tra<strong>in</strong>er, Trust 2].There were concerns, expressed, however, about potential threats to patientsafety which <strong>the</strong>se <strong>IT</strong> applications may engender. Some <strong>of</strong> <strong>the</strong>se could be<strong>in</strong>terpreted as pr<strong>of</strong>essional anxieties about <strong>the</strong>ir roles. For example, concerns88
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2were expressed about <strong>the</strong> openness <strong>of</strong> PACS and a range <strong>of</strong> cl<strong>in</strong>icians be<strong>in</strong>gable to view images. We have already mentioned <strong>the</strong> reduction <strong>in</strong> exposure toradiation because <strong>of</strong> fewer x-rays required us<strong>in</strong>g PACS. However, o<strong>the</strong>rsmentioned that <strong>the</strong>re might be less diligence <strong>in</strong> monitor<strong>in</strong>g exposure toradiation.“radiation <strong>in</strong>cidents can go up because you’ve got a lot <strong>of</strong> patients, a wholeload <strong>of</strong> John Smiths and <strong>the</strong> cl<strong>in</strong>ician wants John Smith number one to select,but <strong>in</strong>advertently selected number two” [Radiographer, Trust 3].There were also concerns that <strong>the</strong>se <strong>IT</strong> applications might lead to less securityfor patients <strong>in</strong> terms <strong>of</strong> access to <strong>the</strong>ir records or an <strong>in</strong>crease <strong>in</strong> errors.“one <strong>of</strong> <strong>the</strong> big nightmares is, um patients be<strong>in</strong>g double-recorded…<strong>the</strong>computer is not as savvy as a human <strong>in</strong> <strong>the</strong> sense <strong>of</strong>, you know, if <strong>the</strong>re’s aspace <strong>the</strong>re but <strong>the</strong> rest <strong>of</strong> it is <strong>the</strong> same that’s go to be a new person” [Seniorcl<strong>in</strong>ician, Trust 4].“just <strong>the</strong> fact <strong>of</strong> many automated processes…it will automatically go on and dothat for you, which sounds great, but if you get a bit carried away it might sort<strong>of</strong> do that to a patient that you didn’t <strong>in</strong>tend to do” [Radiographer, Trust 3].“There was I mean a real, what was a real, you know, SUI, serious untoward<strong>in</strong>cident, whereby it was discovered after about a year <strong>of</strong> we weredo<strong>in</strong>g….somebody was fiddl<strong>in</strong>g around and <strong>the</strong>y, <strong>the</strong>y realised that <strong>the</strong>y couldchange this two weeks to show me all <strong>the</strong> unsigned letters and <strong>the</strong>y suddenlyfound that <strong>the</strong>y had five hundred unsigned letters because <strong>the</strong>y justdisappeared <strong>of</strong>f <strong>the</strong> end…a thousand letters never got sent” [Senior cl<strong>in</strong>ician,Trust 1].In Trust 2 where an <strong>in</strong>adequate e-test order<strong>in</strong>g system was implemented,<strong>the</strong>re was a widely held perception that <strong>the</strong> system led to <strong>in</strong>creases <strong>in</strong> errorsand <strong>in</strong>creased cl<strong>in</strong>ical risk, as this example illustrates:“<strong>the</strong> biggest impact it’s had on patient care that was that for quite a significantperiod <strong>of</strong> time our cl<strong>in</strong>ic had to cont<strong>in</strong>ually audit whe<strong>the</strong>r we were receiv<strong>in</strong>gresults because we, it po<strong>in</strong>ted out, identified and po<strong>in</strong>ted out for <strong>the</strong> hospitalthat large numbers <strong>of</strong> results, whe<strong>the</strong>r positive or negative, were disappear<strong>in</strong>g<strong>in</strong>to <strong>the</strong> computer and no-one was be<strong>in</strong>g made aware <strong>of</strong> positive results, whichhad, which clearly had with it <strong>the</strong>re are def<strong>in</strong>ite <strong>in</strong>stances where it had cl<strong>in</strong>icalconsequences…. we became aware that patients were hav<strong>in</strong>g, um, hadchlamydia but no results had ever been received by anyone” [Senior cl<strong>in</strong>ician,Trust 2].89
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 26.4. Summary <strong>of</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gsThree out <strong>of</strong> four Trusts had implemented some sort <strong>of</strong> PACS system, but onlyTrust 4 had implemented a ‘true’ PACS. Two Trusts had implemented e testorder<strong>in</strong>g and brows<strong>in</strong>g, but <strong>in</strong> one <strong>of</strong> <strong>the</strong>se (Trust 2) <strong>the</strong> system was so poor itwas hardly used so, <strong>in</strong> effect, had not been implemented.Draw<strong>in</strong>g on <strong>the</strong> literature on diffusion <strong>of</strong> <strong>in</strong>novations, we found that <strong>the</strong>re werefour, <strong>in</strong>ter-related factors which <strong>in</strong>fluenced <strong>the</strong> adoption <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications:<strong>the</strong> attributes <strong>of</strong> <strong>the</strong> application; <strong>the</strong> characteristics <strong>of</strong> <strong>the</strong> adopter; implementationprocesses; and organisational factors. In terms <strong>of</strong> <strong>the</strong> attributes <strong>of</strong> <strong>the</strong> application,<strong>the</strong> speed, ease <strong>of</strong> use, reliability and <strong>the</strong> ability to customise were key issues.Thus PACS <strong>in</strong> Trust 4 was adopted much more widely than <strong>in</strong> Trust 2; and e testorder<strong>in</strong>g and brows<strong>in</strong>g was adopted much more quickly and effectively <strong>in</strong> Trust 1than <strong>in</strong> Trust 2. Characteristics <strong>of</strong> adopters seemed to be most important <strong>in</strong> <strong>the</strong>early stages <strong>of</strong> implementation and so <strong>in</strong> all Trusts, <strong>the</strong> challenge <strong>of</strong> persuad<strong>in</strong>gpotential users who were not familiar with us<strong>in</strong>g <strong>IT</strong> was raised. The way <strong>the</strong>se <strong>IT</strong>applications were implemented was crucial to <strong>the</strong>ir use, <strong>in</strong> particular, <strong>the</strong> level <strong>of</strong>user consultation <strong>in</strong> <strong>the</strong> implementation; <strong>the</strong> quality <strong>of</strong> tra<strong>in</strong><strong>in</strong>g and <strong>IT</strong> support; andwhe<strong>the</strong>r <strong>the</strong> applications were implemented <strong>in</strong> terms <strong>of</strong> creat<strong>in</strong>g a ‘critical mass’ <strong>of</strong>benefit. F<strong>in</strong>ally, <strong>the</strong>re were some key organisational factors which <strong>in</strong>fluenced <strong>the</strong>adoption <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications, <strong>the</strong> most important <strong>of</strong> which were: that <strong>the</strong>designers and implementers <strong>of</strong> <strong>the</strong> application understood <strong>the</strong> bus<strong>in</strong>ess process<strong>the</strong> <strong>IT</strong> application was go<strong>in</strong>g to be used <strong>in</strong>; a strong project management team toimplement with high level management support; and <strong>the</strong> level <strong>of</strong> team work<strong>in</strong>gwith<strong>in</strong> and between departments and <strong>the</strong> ability <strong>of</strong> <strong>the</strong> organisation to work as awhole (for example, to implement a ‘critical mass’ <strong>of</strong> <strong>the</strong> application).The perceived impact <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications varied accord<strong>in</strong>g to <strong>the</strong> application,how <strong>the</strong>y had been implemented, and relate to <strong>the</strong> follow<strong>in</strong>g areas: patientexperience; work<strong>in</strong>g practices; and safety/governance. In all cases, <strong>the</strong>re werepositive and negative examples <strong>of</strong> <strong>the</strong>se reported, but overall, for PACS <strong>in</strong> allthree Trusts and e-test order<strong>in</strong>g <strong>in</strong> Trust 1, <strong>the</strong> positives appear to outweigh <strong>the</strong>negatives. Although, very little formal measurement <strong>of</strong> <strong>the</strong>se consequences wascarried out by <strong>the</strong> Trusts, for example, <strong>the</strong> reported <strong>in</strong>crease <strong>in</strong> <strong>the</strong> numbers <strong>of</strong>tests follow<strong>in</strong>g implementation <strong>of</strong> e-test order<strong>in</strong>g was not quantified by Trust 1.90
Report to SDO for NCRS ProjectQualitative F<strong>in</strong>d<strong>in</strong>gs level 2These consequences are important, not least because <strong>the</strong> perceived positive andnegative impact <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> <strong>IT</strong> application <strong>in</strong>fluenced cont<strong>in</strong>ued use <strong>of</strong><strong>the</strong> application and wider adoption.91
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g Trusts7. Quantitative results7.1. Information about participat<strong>in</strong>g TrustsTable 18 gives background quantitative <strong>in</strong>formation about each Trust <strong>in</strong> <strong>the</strong> study,and shows which <strong>of</strong> <strong>the</strong> Trusts implemented <strong>the</strong> <strong>IT</strong> systems on which <strong>the</strong> study isbased, and when. As with any comparison, <strong>the</strong> characteristics <strong>of</strong> <strong>the</strong> control areas important as <strong>the</strong> characteristics <strong>of</strong> <strong>the</strong> <strong>in</strong>tervention, when <strong>in</strong>terpret<strong>in</strong>gdifferences between <strong>the</strong> two. In <strong>the</strong> three Trusts without CPOE, some form <strong>of</strong>computer-based access to pathology test results tended to be available, but thisfell far short <strong>of</strong> <strong>the</strong> rapid and easy access which should be provided by a fullCPOE system, and computer-based access to results was not widely orconsistently used by cl<strong>in</strong>icians.Trust 3 had limited PACS functionality <strong>in</strong> itschildren’s hospital (X-ray only, ma<strong>in</strong>ly with<strong>in</strong> <strong>IT</strong>U). Trust 2 was unable to providepathology data for <strong>the</strong> period before October 2002, and no Urea & Electrolyte(UE) test data were available for this Trust. Data for <strong>the</strong> first three months <strong>of</strong> year2000 were miss<strong>in</strong>g for Trust 2 <strong>in</strong>patient and outpatient, Trust 3 pathology, andTrust 4 pathology and radiology.7.2. CPOE association with primary outcomesThe results <strong>of</strong> <strong>the</strong> between-Trust and with<strong>in</strong>-Trust comparisons for implementation<strong>of</strong> CPOE are summarized <strong>in</strong> Tables 19a and 19b respectively. These tablesshow <strong>the</strong> coefficient or odds ratio for <strong>the</strong> regression model <strong>in</strong>teraction term whichestimates <strong>the</strong> effect <strong>of</strong> <strong>the</strong> CPOE implemented <strong>in</strong> Trust 1 system on <strong>the</strong> primaryoutcomes (see Table 15). The between- and with<strong>in</strong>-Trust data on which <strong>the</strong>seanalyses were based are summarized <strong>in</strong> Appendices 11.1 and 11.2 respectively.The between-Trust results show trends <strong>in</strong> several outcomes, compar<strong>in</strong>g <strong>the</strong> postandpre-<strong>in</strong>tervention periods; <strong>the</strong>se can be seen <strong>in</strong> <strong>the</strong> data (Appendix 11.1). Inparticular, use <strong>of</strong> full blood count (FBC) and ur<strong>in</strong>e culture (UC) tests <strong>in</strong>creased for<strong>in</strong>patients, and use <strong>of</strong> all test types <strong>in</strong>creased for outpatients. ‘Repeat’ tests atoutpatient appo<strong>in</strong>tments also <strong>in</strong>creased for each type <strong>of</strong> test. Trends revealed by<strong>the</strong> between-Trust analyses were generally consistent with <strong>the</strong> results <strong>of</strong> <strong>the</strong>with<strong>in</strong>-Trust analyses, with <strong>the</strong> exception <strong>of</strong> UC test<strong>in</strong>g among <strong>in</strong>patients(Appendix 11.2). Evidence for a possible beneficial impact <strong>of</strong> an CPOE system92
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g Trustsis seen most strik<strong>in</strong>gly <strong>in</strong> <strong>the</strong> reduction <strong>in</strong> outpatient tests. This effect is seen <strong>in</strong><strong>the</strong> between- and with<strong>in</strong>-Trust comparisons for FBC and UE tests; for UC tests<strong>the</strong> effect is seen only <strong>in</strong> <strong>the</strong> between-Trust comparison. The effect <strong>of</strong> CPOE <strong>in</strong>reduc<strong>in</strong>g ‘repeat’ FBC tests at outpatient appo<strong>in</strong>tments is also seen <strong>in</strong> <strong>the</strong>between- and with<strong>in</strong>-Trust comparisons.Conversely, CPOE appears to <strong>in</strong>crease <strong>the</strong> use <strong>of</strong> UE tests among day casepatients. The between-Trust comparison reveals an almost fourfold <strong>in</strong>creaseassociated with CPOE; <strong>the</strong> with<strong>in</strong>-Trust comparison shows that this <strong>in</strong>dicator wasmore than doubled.The o<strong>the</strong>r possibly beneficial effects attributable to CPOE, although seen only <strong>in</strong><strong>the</strong> with<strong>in</strong>-Trust comparison, are reduction <strong>in</strong> FBC and UE tests repeated with<strong>in</strong>48 hours dur<strong>in</strong>g an <strong>in</strong>patient stay, and a reduction <strong>in</strong> FBC test<strong>in</strong>g among<strong>in</strong>patients. Conversely, CPOE is associated with an <strong>in</strong>crease <strong>in</strong> UC test<strong>in</strong>g among<strong>in</strong>patients and day case patients.7.3. PACS association with primary outcomesThe results <strong>of</strong> <strong>the</strong> between-Trust comparison for implementation <strong>of</strong> PACS aresummarized <strong>in</strong> Table 20a; results <strong>of</strong> <strong>the</strong> first and second with<strong>in</strong>-Trustcomparisons are summarized <strong>in</strong> Tables 20b and 20c respectively. As for CPOE,each table shows <strong>the</strong> coefficient or odds ratio for <strong>the</strong> regression model <strong>in</strong>teractionterm which estimates <strong>the</strong> effect <strong>of</strong> PACS on <strong>the</strong> outcome. The correspond<strong>in</strong>gbetween-Trust and with<strong>in</strong>-Trust data on which <strong>the</strong>se analyses were based aresummarized <strong>in</strong> Appendices 12.1 and 12.2 respectively.There was a consistent upward trend <strong>in</strong> ‘repeat’ pla<strong>in</strong>-film X-ray exams atoutpatient appo<strong>in</strong>tments, seen <strong>in</strong> <strong>the</strong> between-Trust (Appendix 12.1) and bothwith<strong>in</strong>-Trust comparisons (Appendix 12.2). An upward trend <strong>in</strong> ComputedTomography (CT) scans per <strong>in</strong>patient day and a downward trend <strong>in</strong> pla<strong>in</strong>-film X-ray exams ‘repeated’ with<strong>in</strong> 48 hours dur<strong>in</strong>g an <strong>in</strong>patient stay were seen <strong>in</strong> <strong>the</strong>between-Trust comparisons and <strong>in</strong> one <strong>of</strong> <strong>the</strong> with<strong>in</strong>-Trust comparisons. Adownward trend <strong>in</strong> use <strong>of</strong> pla<strong>in</strong>-film X-ray exams among <strong>in</strong>patients was seen <strong>in</strong>both with<strong>in</strong>-Trust comparisons. O<strong>the</strong>r trends were apparent only <strong>in</strong> one type <strong>of</strong>comparison.93
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 18: Characteristics <strong>of</strong> <strong>the</strong> participat<strong>in</strong>g TrustsTrust 1 Trust 2 Trust 3 Trust 4Beds 954 (2 sites) 821 (2 sites) 1110 (1 site) 470 (1 site)Forecast cumulative deficit, 1997-2007(% <strong>of</strong> 2006/2007 turnover)Annual <strong>in</strong>patientadmissionsAnnual outpatientappo<strong>in</strong>tments£38M(14.5%)£67M(26.0%)£14M(3.7%)£1.5M(1.1%)2000 73,328 78,647 3 94,135 36,0442001 75,573 78,824 91,744 32,5482002 75,400 83,716 94,933 32,8242003 77,079 88,377 103,119 33,1862004 82,686 99,479 112,599 33,8892005 87,971 105,114 116,771 37,9022000 369,606 367,460 3 397,928 203,1792001 369,070 418,547 399,863 202,1712002 385,132 426,255 411,195 197,2692003 398,120 410,493 407,296 200,6342004 418,590 399,325 422,043 192,9422005 429,354 356,569 432,251 197,6162000 166,824 291,623 3 231,201 3Annual pathology testsdata2001 168,034 311,974 315,188(Full Blood Count, Ureaunavailableand Electrolytes, and 2002 183,658339,997 315,530Ur<strong>in</strong>e Culture) for2003 200,639 452,752 370,298 335,374<strong>in</strong>patients, outpatients andA&E. 1 2004 200,716 494,192 397,392 333,4642005 205,376 505,235 404,766 330,697Annual radiologicalexam<strong>in</strong>ations (Pla<strong>in</strong> Film,Computed Tomographyand Ultrasound) for<strong>in</strong>patients, outpatients andA&E.CPOE2000 69,956 187,365 191,652 71,3762001 70,560 186,219 161,285 71,5182002 77,221 188,012 162,319 72,7402003 80,346 193,820 167,449 75,1422004 83,645 197,991 173,973 73,1602005 85,877 203,731 179,865 72,899New systemimplemented None None None2001-2002 2PACS None None NoneNew systemimplemented2001-2002 41234Urea & Electrolytes test data unavailable for Trust 2.Except <strong>in</strong> maternity.Estimated from data for 9 months (April - December)First <strong>in</strong> A&E and trauma & orthopaedics, <strong>the</strong>n <strong>in</strong> all o<strong>the</strong>r specialties (see Table 2).94
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 19a: Implementation <strong>of</strong> CPOE, between-Trust comparison (Trust 1 vs. Trust 2, 3, and 4). Regression coefficient (Co)or odds ratio (OR) = <strong>in</strong>teraction between <strong>in</strong>tervention (Trust 1) and post-<strong>in</strong>tervention period (2003-2005).Pathology test type Full Blood Count Urea & electrolytes 1 Ur<strong>in</strong>e culturePrimary outcomesRegression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Tests per <strong>in</strong>patient (non-zero vs zero response) OR=0.74 (0.48, 1.16) OR=0.66 (0.43, 1.02) OR=1.14 (0.80, 1.63)InpatientTests per <strong>in</strong>patient day (cont<strong>in</strong>uous non-zero response) Co=1.00 (0.90, 1.10) Co=1.03 (0.89, 1.18) Co=0.93 (0.82, 1.06)Tests per day case (non-zero vs zero response) OR=1.76 (0.78, 3.99) OR=3.63 (1.66, 7.94) 2 OR=1.29 (0.54, 3.13)Test with<strong>in</strong> 48hrs <strong>of</strong> prior test <strong>of</strong> same type OR=0.93 (0.79, 1.10) OR=1.07 (0.89, 1.29) OR=0.89 (0.70, 1.12)OutpatientTests at outpatient appo<strong>in</strong>tment (non-zero vs zero response) OR=0.25 (0.16, 0.40) 2 OR=0.55 (0.39, 0.77) 2 OR=0.30 (0.17, 0.51) 2Same test at next outpatient appo<strong>in</strong>tment OR=0.73 (0.53, 1.00) 2 OR=0.84 (0.64, 1.11) OR=0.73 (0.52, 1.02)12No data were contributed by Trust 2.Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.95
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 19b: Implementation <strong>of</strong> CPOE, with<strong>in</strong>-Trust 1 comparison (Obstetrics vs. all o<strong>the</strong>r specialties), regression coefficient(Co) or odds ratio (OR) = <strong>in</strong>teraction between <strong>in</strong>tervention specialty (obstetrics) and post-<strong>in</strong>tervention period(2003-2005).Pathology test type Full Blood Count Urea & electrolytes Ur<strong>in</strong>e culturePrimary outcomesRegression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Tests per <strong>in</strong>patient (non-zero vs zero response) OR=0.68 (0.55, 0.84) 1 OR=1.24 (0.94, 1.64) OR=2.03 (1.68, 2.46) 1InpatientTests per <strong>in</strong>patient day (cont<strong>in</strong>uous non-zero response) Co=0.95 (0.88, 1.03) Co=0.98 (0.90, 1.06) Co=0.90 (0.81, 1.00)Tests per day case (non-zero vs zero response) OR=1.35 (0.81, 2.24) OR=2.41 (1.54, 3.78) 1 OR=3.49 (1.83, 6.67) 1Test with<strong>in</strong> 48hrs <strong>of</strong> prior test <strong>of</strong> same type OR=0.88 (0.79, 0.98) 1 OR=0.77 (0.69, 0.87) 1 OR=0.90 (0.64, 1.27)OutpatientTests at outpatient appo<strong>in</strong>tment (non-zero vs zero response) OR=0.70 (0.55, 0.88) 1 OR=0.51 (0.39, 0.65) 1 OR=0.86 (0.67, 1.10)Same test at next outpatient appo<strong>in</strong>tment OR=0.84 (0.71, 0.99) 1 OR=0.80 (0.63, 1.02) OR=0.81 (0.64, 1.04)1Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.96
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsEvidence for a possible beneficial impact <strong>of</strong> PACS is seen <strong>in</strong> <strong>the</strong> reduction <strong>in</strong>‘repeat’ pla<strong>in</strong>-film X-ray exams at outpatient appo<strong>in</strong>tments (as seen <strong>in</strong> <strong>the</strong>between-Trust comparison, Table 19b, and <strong>the</strong> second with<strong>in</strong>-Trust comparison,Table 19c), and <strong>in</strong> <strong>the</strong> reduction <strong>in</strong> <strong>in</strong>patient CT scans (between-Trustcomparison). O<strong>the</strong>r evidence for a possibly beneficial effect <strong>of</strong> PACS was <strong>the</strong>reduction <strong>in</strong> pla<strong>in</strong>-film X-ray exams requested at outpatient appo<strong>in</strong>tments (secondwith<strong>in</strong>-Trust comparison only). Conversely, <strong>in</strong> <strong>the</strong> between-Trust comparison,PACS was associated with <strong>in</strong>creases <strong>in</strong> CT scans requested at outpatientappo<strong>in</strong>tments, and with CT scans ‘repeated’ with<strong>in</strong> 48 hours dur<strong>in</strong>g an <strong>in</strong>patientstay; and <strong>in</strong> <strong>the</strong> second with<strong>in</strong>-Trust comparison, with an <strong>in</strong>crease <strong>in</strong> pla<strong>in</strong>-film X-ray exams per <strong>in</strong>patient.The reduction <strong>in</strong> ultrasound (US) scans ‘repeated’ with<strong>in</strong> 48hrs dur<strong>in</strong>g an <strong>in</strong>patientstay, which is seen <strong>in</strong> both with<strong>in</strong>-Trust comparisons, is very unlikely to beattributable to PACS because ultrasound was not part <strong>of</strong> <strong>the</strong> PACSimplementation. Also, <strong>the</strong> numbers <strong>of</strong> patients from which <strong>the</strong>se results werederived are relatively small (Appendix 12.2). The only way <strong>in</strong> which <strong>the</strong> reduction<strong>in</strong> repeat US scans might be attributed to PACS would be if, for example, generalreorganisation <strong>of</strong> work flows <strong>in</strong> radiology as a result <strong>of</strong> implement<strong>in</strong>g PACS foro<strong>the</strong>r imag<strong>in</strong>g modes also brought about similar changes. Interviews with staff <strong>in</strong>Trust 4 confirmed that work flows <strong>in</strong> radiology were <strong>in</strong>deed radically changedwhen PACS was implemented, but <strong>the</strong> <strong>in</strong>terviews did not address directly whe<strong>the</strong>r<strong>the</strong>se changes could have affected order<strong>in</strong>g and report<strong>in</strong>g <strong>of</strong> US scans because<strong>the</strong>y were conducted prior to this quantitative analysis be<strong>in</strong>g carried out..7.4. Secondary outcomesThe results <strong>of</strong> our analyses <strong>of</strong> <strong>the</strong> impact <strong>of</strong> CPOE and PACS on secondaryoutcomes, compar<strong>in</strong>g <strong>in</strong>tervention Trusts with control Trusts, are summarized <strong>in</strong>Table 21a. The results <strong>of</strong> with<strong>in</strong>-Trust comparisons are summarized <strong>in</strong> Table 21bfor CPOE and Table 21c for PACS. The data on which <strong>the</strong> between-Trustanalyses were based are summarized <strong>in</strong> Appendix 13.1; <strong>the</strong> data on which <strong>the</strong>with<strong>in</strong>-Trust analyses were based are summarized <strong>in</strong> Appendix 13.2 for CPOEand Appendix 13.3 for PACS.97
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 20a: Implementation <strong>of</strong> PACS, between-Trust comparison (Trust 4 vs Trusts 1, 2, and 3). Regression coefficient (Co)or odds ratio (OR) = <strong>in</strong>teraction between <strong>in</strong>tervention (Trust 4) and post-<strong>in</strong>tervention period (2003-2005).Radiology exam<strong>in</strong>ation typePla<strong>in</strong> filmComputedTomographyUltrasound (not part <strong>of</strong>PACS <strong>in</strong> Trust 4)Primary outcomesRegression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Tests per <strong>in</strong>patient (non-zero vs zero response) OR1=0.90 (0.71, 1.14) OR1=0.83 (0.70, 0.98) 1 OR1=0.89 (0.69, 1.14)InpatientTests per <strong>in</strong>patient day (cont<strong>in</strong>uous non-zero response) Co1=0.97 (0.90, 1.05) Co1=1.02 (0.91, 1.14) Co1=0.96 (0.85, 1.09)Tests per day case (non-zero vs zero response) OR1=1.01 (0.55, 1.86) OR1=0.73 (0.31, 1.73) OR1=1.55 (0.83, 2.89)Test with<strong>in</strong> 48hrs <strong>of</strong> prior test <strong>of</strong> same type OR1=1.02 (0.91, 1.14) OR1=2.18 (1.52, 3.14) 1 OR1=1.08 (0.81, 1.44)OutpatientTests at outpatient appo<strong>in</strong>tment (non-zero vs zero response) OR1=0.90 (0.76, 1.07) OR1=1.89 (1.26, 2.84) 1 OR1=1.48 (0.60, 3.66)Same test at next outpatient appo<strong>in</strong>tment OR1=0.62 (0.44, 0.88) 1 n/a 2 OR1=0.58 (0.19, 1.82)12Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.Not analysed due to small numbers.98
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 20b: Implementation <strong>of</strong> PACS, first with<strong>in</strong>-Trust 4 comparison, before and after implementation <strong>in</strong> A&E andorthopaedics. Regression coefficient (Co) or odds ratio (OR) = <strong>in</strong>teraction between <strong>in</strong>tervention and post<strong>in</strong>terventionperiod.Radiology exam<strong>in</strong>ation typePla<strong>in</strong> filmComputedTomographyUltrasound (not part <strong>of</strong>PACS <strong>in</strong> Trust 4)Primary outcomesRegression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Tests per <strong>in</strong>patient (non-zero vs zero response) OR=1.10 (0.97, 1.25) OR=1.05 (0.85, 1.31) OR=1.03 (0.74, 1.43)InpatientTests per <strong>in</strong>patient day (cont<strong>in</strong>uous non-zero response) Co=1.01 (0.88, 1.14) Co=0.95 (0.73, 1.23) Co=1.18 (0.88, 1.58)Tests per day case (non-zero vs zero response) OR=0.81 (0.65, 1.02) OR=0.98 (0.36, 2.65) OR=0.71 (0.16, 3.17)Test with<strong>in</strong> 48hrs <strong>of</strong> prior test <strong>of</strong> same type OR=0.96 (0.89, 1.02) OR=0.70 (0.26, 1.88) OR=0.24 (0.10, 0.55) 1OutpatientTests at outpatient appo<strong>in</strong>tment (non-zero vs zero response) OR=0.90 (0.81, 1.01) n/a 2 n/a 2Same test at next outpatient appo<strong>in</strong>tment OR=0.85 (0.62, 1.17) n/a 2 n/a 212Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.Not analysed due to small numbers.99
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 20c: Implementation <strong>of</strong> PACS, second with<strong>in</strong>-Trust 4 comparison, before and after implementation <strong>in</strong> all specialtiesexcept A&E and orthopaedics. Regression coefficient (Co) or odds ratio (OR) = <strong>in</strong>teraction between <strong>in</strong>terventionand post-<strong>in</strong>tervention period.Radiology exam<strong>in</strong>ation typePla<strong>in</strong> filmComputedTomographyUltrasound (not part <strong>of</strong>PACS <strong>in</strong> Trust 4)Primary outcomesRegression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Regression coefficientor odds ratio (95% CI)Tests per <strong>in</strong>patient (non-zero vs zero response) OR1=1.33 (1.09, 1.62) 1 OR1=1.05 (0.94, 1.17) OR1=0.81 (0.65, 1.01)InpatientTests per <strong>in</strong>patient day (cont<strong>in</strong>uous non-zero response) Co1=0.95 (0.81, 1.12) Co1=0.75 (0.54, 1.04) Co1=0.89 (0.53, 1.50)Tests per day case (non-zero vs zero response) OR1=1.05 (0.84, 1.30) OR1=0.99 (0.50, 1.98) OR1=0.45 (0.08, 2.63)Test with<strong>in</strong> 48hrs <strong>of</strong> prior test <strong>of</strong> same type OR1=1.05 (0.92, 1.21) OR1=0.51 (0.26, 1.03) OR1=0.35 (0.16, 0.75) 1,2OutpatientTests at outpatient appo<strong>in</strong>tment (non-zero vs zero response) OR1=0.75 (0.69, 0.82) 1 n/a 3 n/a 3Same test at next outpatient appo<strong>in</strong>tment OR1=0.75 (0.61, 0.92) 1 n/a 3 n/a 3123Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.This estimate is based on small numbers <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention group (see Appendix 12.2).Estimate could not be calculated because <strong>of</strong> <strong>the</strong> small number <strong>of</strong> patients who had a CT repeated at <strong>the</strong> next outpatient appo<strong>in</strong>tment.100
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsThere were clear trends over time <strong>in</strong> seven <strong>of</strong> <strong>the</strong> eight secondary outcomes <strong>in</strong><strong>the</strong> between-Trust analysis. Of <strong>the</strong>se seven trends, three were consistentbetween both types <strong>of</strong> analysis (between- and with<strong>in</strong>-Trust); greater likelihood <strong>of</strong>be<strong>in</strong>g discharged follow<strong>in</strong>g admission (i.e. shorter length <strong>of</strong> stay), <strong>the</strong> lowerlikelihood <strong>of</strong> <strong>in</strong>tended day case patients be<strong>in</strong>g admitted overnight, and <strong>the</strong><strong>in</strong>creased likelihood <strong>of</strong> be<strong>in</strong>g discharged from fur<strong>the</strong>r follow-up at an outpatientappo<strong>in</strong>tment. There were upward trends <strong>in</strong> day case admission and outpatientattendance <strong>in</strong> <strong>the</strong> between-Trust comparison, but a downward trend <strong>in</strong> <strong>the</strong>seoutcomes <strong>in</strong> <strong>the</strong> comparison with<strong>in</strong> Trust 1. One <strong>of</strong> <strong>the</strong> two comparisons with<strong>in</strong>Trust 4 showed an upward trend <strong>in</strong> outpatient attendance. Comparisons with<strong>in</strong>Trusts 1 and 4 showed opposite trends <strong>in</strong> outpatient attendance. None <strong>of</strong> <strong>the</strong>trends <strong>in</strong> secondary outcomes with<strong>in</strong> Trust 4 were seen <strong>in</strong> ei<strong>the</strong>r <strong>the</strong> first orsecond PACS comparison.The between-Trust and with<strong>in</strong>-Trust analyses showed potentially detrimentalassociations <strong>of</strong> CPOE and PACS with a reduced likelihood <strong>of</strong> outpatients be<strong>in</strong>gdischarged. This association <strong>in</strong> <strong>the</strong> between-Trust analysis was contradicted by<strong>the</strong> analysis with<strong>in</strong> <strong>the</strong> Trust that implemented CPOE, which showed <strong>the</strong> oppositeeffect. The between-Trust analysis showed a beneficial effect <strong>of</strong> CPOE <strong>in</strong>reduc<strong>in</strong>g <strong>in</strong>patient deaths; this result could not be <strong>in</strong>vestigated <strong>in</strong> <strong>the</strong> with<strong>in</strong>-Trustanalysis because <strong>the</strong>re were an <strong>in</strong>sufficient number <strong>of</strong> deaths <strong>in</strong> <strong>the</strong> controlspecialty (obstetrics). Conversely, analysis with<strong>in</strong> <strong>the</strong> Trust which implementedCPOE showed potentially detrimental associations <strong>of</strong> CPOE with longer length <strong>of</strong>stay, and an <strong>in</strong>creased likelihood <strong>of</strong> a day case patient be<strong>in</strong>g admitted overnight;<strong>the</strong>se associations were not seen <strong>in</strong> <strong>the</strong> between-Trust analysis. An association<strong>of</strong> PACS with longer length-<strong>of</strong>-stay was seen <strong>in</strong> <strong>the</strong> second, but not <strong>in</strong> <strong>the</strong> first,with<strong>in</strong>-Trust PACS comparison; as was an association <strong>of</strong> PACS with a reduction<strong>in</strong> <strong>the</strong> proportion <strong>of</strong> outpatients discharged. A shorter time-to-death was seen <strong>in</strong><strong>the</strong> first, but not <strong>in</strong> <strong>the</strong> second, with<strong>in</strong>-Trust PACS comparison.101
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 21a: Implementation <strong>of</strong> CPOE (Trust 1) and PACS (Trust 4), between-Trust comparison. Hazard (HR) or odds ratio(OR) = <strong>in</strong>teraction between <strong>in</strong>tervention Trust (Trust 1, CPOE; Trust 4, PACS) and post-<strong>in</strong>tervention period (2003-2005).Trust 1 (CPOE)Trust 4 (PACS)Secondary outcomes Hazard or odds ratio (95% CI) Hazard or odds ratio (95% CI)Length-<strong>of</strong>-stay (exclud<strong>in</strong>g day cases) HR=1.02 (0.96, 1.08) HR=0.95 (0.89, 1.02)Inpatient treated as a day case (i.e. zero length <strong>of</strong> stay) OR=0.97 (0.77, 1.22) OR=0.92 (0.74, 1.15)InpatientIntended day case patient admitted overnight no data available OR=0.85 (0.53, 1.39)Emergency re-admission (with<strong>in</strong> 28 days) OR=1.05 (0.84, 1.32) OR=0.95 (0.79, 1.14)Deaths OR=0.82 (0.71, 0.95) 1 OR=0.91 (0.75, 1.09)Time-to-death HR=0.98 (0.92, 1.04) HR=1.05 (0.99, 1.11)OutpatientAttendance (Attended vs Did Not Attend) OR=0.87 (0.78, 0.98) 1 OR=0.94 (0.86, 1.04)Outcome (discharged vs follow-up) OR=0.73 (0.55, 0.98) 1 OR=0.58 (0.43, 0.78) 11Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.102
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 21b: Implementation <strong>of</strong> CPOE (Trust 1), with<strong>in</strong>-Trust comparison. Hazard (HR) or odds ratio (OR) = <strong>in</strong>teractionbetween all specialties except obstetrics and post-<strong>in</strong>tervention period (2003-2005).Trust 1 (CPOE)Secondary outcomesHazard or odds ratio (95% CI)Length-<strong>of</strong>-stay (exclud<strong>in</strong>g day cases) HR=0.95 (0.92, 0.97) 1Inpatient treated as a day case (i.e. zero length <strong>of</strong> stay) OR=1.61 (1.36, 1.92) 1InpatientIntended day case patient admitted overnight n/a 2Emergency re-admission (with<strong>in</strong> 28 days) n/a 2Deaths n/a 2Time-to-death HR=0.96 (0.92, 1.00)OutpatientAttendance (Attended vs Did Not Attend) OR=1.42 (1.22, 1.66) 1Outcome (discharged vs follow-up) OR=0.74 (0.70, 0.77) 112Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.Not analysed due to small numbers.103
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTable 21c: Implementation <strong>of</strong> PACS (Trust 4), with<strong>in</strong>-Trust comparison. Hazard (HR) or odds ratio (OR) = <strong>in</strong>teractionbetween <strong>in</strong>tervention specialties and post-<strong>in</strong>tervention period (2003-2005). 1 st PACS comparison , beforeand after implementation <strong>in</strong> A&E and orthopaedics (post-<strong>in</strong>tervention period, 12/2001-10/2002; pre<strong>in</strong>terventionperiod, 01/2000-11/2001). 2 nd PACS comparison, before and after implementation <strong>in</strong> allspecialties except A&E and orthopaedics (post-<strong>in</strong>tervention period, 11/2002-12/2005; pre-<strong>in</strong>terventionperiod, 12/2001-10/2002).1st PACS comparison2 nd PACS comparisonSecondary outcomes Hazard or odds ratio (95% CI) Hazard or odds ratio (95% CI)Length-<strong>of</strong>-stay (exclud<strong>in</strong>g day cases) HR1=0.97 (0.90, 1.04) HR1=0.91 (0.83, 0.99) 1Inpatient treated as a day case (i.e. zero length <strong>of</strong> stay) OR1=0.94 (0.82, 1.09) OR1=0.81 (0.46, 1.04)InpatientIntended day case patient admitted overnight OR1=1.54 (0.85, 2.79) OR1=1.72 (0.89, 3.30)Emergency re-admission (with<strong>in</strong> 28 days) OR1=1.04 (0.89, 1.21) OR1=1.04 (0.89, 1.23)Deaths OR1=1.38 (0.91, 2.09) OR1=1.50 (0.87, 2.58)Time-to-death HR1=1.12 (1.01, 1.25) 1 HR1=1.00 (0.80, 1.25)OutpatientAttendance (Attended vs Did Not Attend) OR1=0.99 (0.93, 1.04) OR1=0.94 (0.84, 1.05)Outcome (discharged vs follow-up) OR1=0.95 (0.87, 1.04) OR1=0.82 (0.75, 0.90) 11Estimates with confidence <strong>in</strong>tervals exclud<strong>in</strong>g 1 are shown <strong>in</strong> underl<strong>in</strong>ed bold text.104
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g Trusts7.5. Summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gsOur study was <strong>the</strong> largest <strong>of</strong> its k<strong>in</strong>d with<strong>in</strong> <strong>the</strong> UK, if not <strong>in</strong>ternationally, and it wasmade possible by <strong>the</strong> uniformity <strong>of</strong> data report<strong>in</strong>g across <strong>NHS</strong> Trusts. We discussour results <strong>in</strong> detail below; <strong>the</strong>se were <strong>in</strong>terpreted <strong>in</strong> <strong>the</strong> context <strong>of</strong> temporaltrends <strong>in</strong> <strong>the</strong> outcomes (as <strong>in</strong>dicated by <strong>the</strong> regression model parameter for <strong>the</strong>post-<strong>in</strong>tervention period vs <strong>the</strong> pre-<strong>in</strong>tervention period), and by <strong>in</strong>spection <strong>of</strong> <strong>the</strong>data on from which <strong>the</strong> regression model estimates were obta<strong>in</strong>ed (assummarized <strong>in</strong> Appendices 11 to 13).Implementation <strong>of</strong> <strong>the</strong> CPOE system or PACS was <strong>in</strong>corporated <strong>in</strong> each <strong>of</strong> <strong>the</strong>regression models as an <strong>in</strong>teraction term; hence <strong>the</strong> quantifiable impact <strong>of</strong> <strong>the</strong> <strong>IT</strong>system manifests as a modification <strong>of</strong> <strong>the</strong> underly<strong>in</strong>g temporal effect (trend). Suchunderly<strong>in</strong>g trends were seen for two-thirds (25/39) <strong>of</strong> all outcomes <strong>in</strong> between-Trust comparisons, and <strong>in</strong> half (34/67) <strong>of</strong> all outcomes <strong>in</strong> with<strong>in</strong>-Trustcomparisons. In between-Trust analyses, we found evidence for an effect <strong>of</strong>CPOE on 5 out <strong>of</strong> 18 primary outcomes, and on 3 out <strong>of</strong> 7 secondary outcomes;and for PACS, on 4 <strong>of</strong> 17 primary outcomes, and 1 <strong>of</strong> 8 secondary outcomes.Only three <strong>of</strong> <strong>the</strong>se thirteen effects occurred <strong>in</strong> <strong>the</strong> absence <strong>of</strong> an underly<strong>in</strong>g trend<strong>in</strong> <strong>the</strong> outcome.7.5.1. Impact <strong>of</strong> CPOE on primary outcomesThe effect <strong>of</strong> CPOE <strong>in</strong> reduc<strong>in</strong>g <strong>the</strong> upward trend <strong>in</strong> outpatient pathology testsderives from <strong>the</strong> decrease <strong>in</strong> FBC, UE and UR tests ordered at outpatientappo<strong>in</strong>tments <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust, compared with <strong>in</strong>creases <strong>in</strong> this<strong>in</strong>dicator <strong>in</strong> <strong>the</strong> two control Trusts for which data were available (Appendix11.1). With<strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust, this same effect is seen for FBC and UEtests <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention specialties compared with <strong>the</strong> control specialty(Appendix 11.2). Attribution <strong>of</strong> this effect to implementation <strong>of</strong> CPOE isplausible if <strong>the</strong> CPOE system enables <strong>the</strong> cl<strong>in</strong>ician to access <strong>the</strong> patient'spathology test history dur<strong>in</strong>g <strong>the</strong> outpatient appo<strong>in</strong>tment, thus reduc<strong>in</strong>g <strong>the</strong>number <strong>of</strong> unnecessary repeat tests. This argument is streng<strong>the</strong>ned by <strong>the</strong>105
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g Trustsreduction <strong>in</strong> ‘repeat’ FBC tests ordered at consecutive outpatientappo<strong>in</strong>tments, as seen <strong>in</strong> both between- and with<strong>in</strong>-Trust results.Thesef<strong>in</strong>d<strong>in</strong>gs are consistent with <strong>the</strong> views <strong>of</strong> users expressed <strong>in</strong> <strong>in</strong>terviews (seechapter 6).The effect <strong>of</strong> CPOE <strong>in</strong> fur<strong>the</strong>r <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> upward trend <strong>in</strong> UE tests orderedfor day case patients, as seen <strong>in</strong> both between- and with<strong>in</strong>-Trust results,derives from a large <strong>in</strong>crease <strong>in</strong> this <strong>in</strong>dicator <strong>in</strong> Trust 1 (from 2.2% to 10.2%)compared with <strong>the</strong> two control Trusts, one <strong>of</strong> which also saw a large <strong>in</strong>crease(from 9.9% to 18.7%), and from a relatively small <strong>in</strong>crease <strong>in</strong> this <strong>in</strong>dicator <strong>in</strong><strong>the</strong> control specialty (from 4.8% to 7.1%) compared with all o<strong>the</strong>r specialtieswith<strong>in</strong> Trust 1 (from 2.3% to 10.7%). There has been a large <strong>in</strong>crease <strong>in</strong> UEtest order<strong>in</strong>g across all Trusts, but <strong>the</strong> reason for <strong>the</strong> greater relative <strong>in</strong>crease<strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust is unclear, hence attribution <strong>of</strong> causality to <strong>the</strong>implementation <strong>of</strong> CPOE is not possible. It should also be noted that <strong>the</strong>proportion <strong>of</strong> day case patients for whom a UE test was ordered <strong>in</strong> Trust 1rema<strong>in</strong>ed much lower than <strong>in</strong> Trust 4, suggest<strong>in</strong>g that our measure <strong>of</strong> effectmay be susceptible to residual confound<strong>in</strong>g due to differences <strong>in</strong> case mixbetween <strong>the</strong> Trusts.Five o<strong>the</strong>r possible effects <strong>of</strong> CPOE were suggested by <strong>the</strong> with<strong>in</strong>-Trustanalysis: no change <strong>in</strong> FBC <strong>in</strong>patient tests (compared with an <strong>in</strong>crease <strong>in</strong>obstetrics), a relatively smaller <strong>in</strong>crease <strong>in</strong> FBC and UE <strong>in</strong>patient testsrepeated with<strong>in</strong> 48hrs (compared with larger <strong>in</strong>creases <strong>in</strong> obstetrics), a big<strong>in</strong>crease <strong>in</strong> UC tests per day case (compared with a reduction <strong>in</strong> obstetrics),and a relatively small decrease <strong>in</strong> UC tests per <strong>in</strong>patient (compared with alarger decrease <strong>in</strong> obstetrics). Aga<strong>in</strong>, <strong>in</strong>terpretation <strong>of</strong> <strong>the</strong>se results, andattribution <strong>of</strong> causality to implementation <strong>of</strong> CPOE, is not possible without an<strong>in</strong>-depth understand<strong>in</strong>g <strong>of</strong> cl<strong>in</strong>ical practice with<strong>in</strong> specialties. However, giventhat all <strong>of</strong> <strong>the</strong>se effects derived ma<strong>in</strong>ly from trends with<strong>in</strong> <strong>the</strong> control specialty,<strong>the</strong> role <strong>of</strong> CPOE can probably be discounted.106
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g Trusts7.5.2. Impact <strong>of</strong> PACS on primary outcomesImplementation <strong>of</strong> PACS attenuated an upward trend <strong>in</strong> CT scans requestedfor <strong>in</strong>patients, but amplified an upward trend <strong>in</strong> CT scans requested atoutpatient appo<strong>in</strong>tments. PACS was also associated with an <strong>in</strong>crease <strong>in</strong> CTscans repeated with<strong>in</strong> 48hrs dur<strong>in</strong>g <strong>in</strong>patient stay. These effects were seenonly <strong>in</strong> <strong>the</strong> between-Trust analyses. The first <strong>of</strong> <strong>the</strong>se effects derives from arelatively small <strong>in</strong>crease <strong>in</strong> <strong>in</strong>patient CT scans <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust (from8.1% to 10.2%) compared with <strong>the</strong> control Trusts. The second effect derivesfrom a big <strong>in</strong>crease <strong>in</strong> outpatient CT scans <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust (from0.02% to 0.21%), compared with no change <strong>in</strong> Trusts 2 and 3, although <strong>the</strong>reis a similarly big <strong>in</strong>crease <strong>in</strong> Trust 1 (from 0.03% to 0.25%). The third effectderives from a doubl<strong>in</strong>g <strong>of</strong> repeat <strong>in</strong>patient CT scans <strong>in</strong> Trust 4 (from 1.2% to2.5%) compared with small reductions <strong>in</strong> Trusts 2 and 3, and a slight <strong>in</strong>crease<strong>in</strong> Trust 1.Explanations for <strong>the</strong> relatively large <strong>in</strong>creases <strong>in</strong> outpatient CT scans andrepeat <strong>in</strong>patient CT scans <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust, and <strong>the</strong> large <strong>in</strong>crease <strong>in</strong>outpatient CT scans <strong>in</strong> Trust 1, were not forthcom<strong>in</strong>g from <strong>the</strong> Trusts. New CTmach<strong>in</strong>es were <strong>in</strong>stalled <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust <strong>in</strong> 2000 and 2006. A new CTmach<strong>in</strong>e was <strong>in</strong>stalled <strong>in</strong> Trust 1 <strong>in</strong> 2003, but this was to replace an exist<strong>in</strong>gmach<strong>in</strong>e. These results suggest that implementation <strong>of</strong> PACS <strong>in</strong> Trust 4 mayhave enabled an <strong>in</strong>creas<strong>in</strong>g demand for CT scans to be met throughoutpatient appo<strong>in</strong>tments, ra<strong>the</strong>r than through <strong>in</strong>patient admissions. It is <strong>the</strong>nplausible that those patients who still required hospital admission would bethose patients who needed repeat scans. However, a large <strong>in</strong>crease <strong>in</strong>outpatient CT scans was also seen <strong>in</strong> one <strong>of</strong> <strong>the</strong> control Trusts, henceattribution <strong>of</strong> <strong>the</strong>se effects to implementation <strong>of</strong> PACS is questionable.PACS also appeared to attenuate an upward trend <strong>in</strong> repeat PF exams atconsecutive outpatient appo<strong>in</strong>tments. As with repeat FBC tests at consecutiveoutpatient appo<strong>in</strong>tments, attribution <strong>of</strong> this effect to implementation <strong>of</strong> <strong>the</strong> newsystem is plausible if PACS enables <strong>the</strong> cl<strong>in</strong>ician to access <strong>the</strong> patient'sradiological exam<strong>in</strong>ation history dur<strong>in</strong>g <strong>the</strong> outpatient appo<strong>in</strong>tment. However,an <strong>in</strong>spection <strong>of</strong> <strong>the</strong> data (Appendix 12.1) reveals that this apparent effect isdue to <strong>in</strong>creases <strong>in</strong> repeat outpatient PF exams with<strong>in</strong> two <strong>of</strong> <strong>the</strong> control107
Report to SDO for NCRS ProjectParticipat<strong>in</strong>g TrustsTrusts; <strong>in</strong> <strong>the</strong> third control Trust and <strong>in</strong> <strong>the</strong> <strong>in</strong>tervention Trust <strong>the</strong>re is littlechange <strong>in</strong> this outcome. Also, while this effect was also seen with<strong>in</strong> Trust 4when all specialties except trauma and orthopaedics were compared withtrauma and orthopaedics <strong>in</strong> <strong>the</strong> second PACS comparison, this resultcontradicts <strong>the</strong> data beh<strong>in</strong>d <strong>the</strong> first comparison, which show an <strong>in</strong>crease <strong>in</strong>repeat PF exams after implementation <strong>of</strong> PACS (Appendix 12.2).7.5.3. Impact <strong>of</strong> CPOE and PACS on secondary outcomesAttribution <strong>of</strong> changes <strong>in</strong> secondary outcomes to implementation <strong>of</strong> ei<strong>the</strong>rCPOE or PACS is even more problematic than <strong>the</strong> attribution <strong>of</strong> changes <strong>in</strong>primary outcomes to implementation <strong>of</strong> <strong>the</strong>se systems. Secondary outcomesare likely to be strongly <strong>in</strong>fluenced by concurrent process changes and eventswith<strong>in</strong> <strong>the</strong> <strong>NHS</strong> <strong>in</strong> general (affect<strong>in</strong>g between-Trust comparisons), and with<strong>in</strong>participat<strong>in</strong>g Trusts <strong>in</strong> particular (affect<strong>in</strong>g between- and with<strong>in</strong>-Trustcomparisons). Our results did not demonstrate any consistent or plausibleeffects <strong>of</strong> CPOE or PACS on secondary outcomes.108
Report to SDO for NCRS ProjectDiscussion8. Discussion8.1. IntroductionIn chapter one, we described how <strong>the</strong> conception <strong>of</strong> this project changed with <strong>the</strong>chang<strong>in</strong>g policy context. We had orig<strong>in</strong>ally set out to evaluate <strong>the</strong> implementation<strong>of</strong> EPRs at local level. With <strong>the</strong> establishment <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>, we aimed to evaluate<strong>the</strong> impact <strong>of</strong> <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> applications through <strong>the</strong> nationalprogramme at local level. However, as <strong>the</strong> NPf<strong>IT</strong> failed to deliver accord<strong>in</strong>g to itsorig<strong>in</strong>al timetable, <strong>in</strong> Level 1 <strong>of</strong> our qualitative study, we tracked <strong>the</strong> impact <strong>of</strong> thisfailure at local level at two po<strong>in</strong>ts <strong>in</strong> time. We have been unable to evaluate <strong>IT</strong>applications implemented through <strong>the</strong> national programme because, <strong>in</strong> <strong>the</strong> course<strong>of</strong> this study, none were implemented <strong>in</strong> our four case study Trusts. We wereable to evaluate quantitatively and qualitatively, to a limited degree, <strong>the</strong> impact <strong>of</strong>two specific <strong>IT</strong> applications (PACS and CPOE) which had been implemented <strong>in</strong>some <strong>of</strong> our Trusts prior to <strong>the</strong> launch <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>.We also conducted asystematic review <strong>of</strong> economic evaluations <strong>of</strong> large-scale health care <strong>IT</strong>implementations to meet our fifth objective, to evaluate <strong>the</strong> economic evidence for<strong>the</strong> cost-effectiveness <strong>of</strong> <strong>IT</strong> systems <strong>in</strong> health care.In this chapter, we first summarise <strong>the</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gs from <strong>the</strong> empirical elements<strong>of</strong> our study; secondly, we identify <strong>the</strong> study’s strengths and weaknesses; thirdly,we place our f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> <strong>the</strong> context <strong>of</strong> <strong>the</strong> exist<strong>in</strong>g literature; fourthly, we identifyfuture areas for research; and f<strong>in</strong>ally, we set out <strong>the</strong> implications for managementand policy from our research.8.2. Summary <strong>of</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gs8.2.1. Qualitative <strong>in</strong>terviews, Level 1The first round <strong>of</strong> level 1 <strong>in</strong>terviews, with senior managers and cl<strong>in</strong>icians,highlighted four key issues:(a) Trusts vary <strong>in</strong> <strong>the</strong>ir circumstances, which affect <strong>the</strong>ir ability to implement<strong>the</strong> National Programme.(b) The process <strong>of</strong> implement<strong>in</strong>g <strong>the</strong> National Programme was suboptimal,lead<strong>in</strong>g to low morale among <strong>NHS</strong> staff responsible for implementation.109
Report to SDO for NCRS ProjectDiscussion(c) The overall timetable for implementation was unrealistic, with Trusts fac<strong>in</strong>gmajor uncerta<strong>in</strong>ties. The need to renew <strong>the</strong> PAS represented a bottleneckand <strong>the</strong> schedule for this activity could not be reconciled with targets forimplementation <strong>of</strong> substantive <strong>IT</strong> applications.(d) Short term benefits <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> are unlikely to be sufficient topersuade <strong>NHS</strong> staff to support <strong>the</strong> programme unreservedly, particularly ifnew applications deliver lower levels <strong>of</strong> functionality.It was far too early at <strong>the</strong> time <strong>of</strong> <strong>the</strong>se <strong>in</strong>terviews to assess <strong>the</strong> success <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong>, but <strong>the</strong> process <strong>of</strong> implementation was already clearly caus<strong>in</strong>g concern.In <strong>the</strong> second round (Level 1, stage b.) <strong>of</strong> <strong>in</strong>terviews with senior managers andcl<strong>in</strong>icians, it was clear that <strong>the</strong> NPf<strong>IT</strong> is a highly desirable objective.Interviewees were enthusiastic about, and supportive <strong>of</strong>, <strong>the</strong> goals <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong>. However, senior Trust staff still had serious concerns, several <strong>of</strong> whichwere <strong>the</strong> same as dur<strong>in</strong>g <strong>the</strong> first round <strong>of</strong> <strong>in</strong>terviews.Cont<strong>in</strong>u<strong>in</strong>g uncerta<strong>in</strong>ty about <strong>the</strong> programme was mak<strong>in</strong>g key managerialdecisions about <strong>IT</strong> implementation more difficult, given <strong>the</strong> current need tomake f<strong>in</strong>ancial sav<strong>in</strong>gs and achieve efficiencies. Although <strong>IT</strong> <strong>modernisation</strong>should facilitate <strong>the</strong>se goals <strong>in</strong> <strong>the</strong> longer-term, at <strong>the</strong> time <strong>of</strong> <strong>the</strong> second<strong>in</strong>terviews senior managers still did not know:(a) what <strong>the</strong> local costs <strong>of</strong> implementation will be;(b) when a replacement patient adm<strong>in</strong>istration system compliant with <strong>the</strong>programme will be available;(c) <strong>the</strong> timetable for delivery <strong>of</strong> <strong>in</strong>terim applications;(d) <strong>the</strong> features <strong>of</strong> <strong>the</strong>se applications;(e) <strong>the</strong> likely benefits and efficiencies from new systems.In <strong>the</strong> face <strong>of</strong> <strong>the</strong>se uncerta<strong>in</strong>ties, managers found it difficult to prioritise localimplementation <strong>of</strong> <strong>the</strong> NPf<strong>IT</strong>. Concern was expressed about threats to patientsafety from a ‘patch and mend’ approach to ma<strong>in</strong>ta<strong>in</strong> exist<strong>in</strong>g systems. Trustmanagers spoke clearly about <strong>the</strong>ir need for concrete <strong>in</strong>formation aboutimplementation timetables, system compatibility with <strong>the</strong> long term goals <strong>of</strong> <strong>the</strong>programme, and value-for-money.communication between CfH and Trusts to improve.More generally, <strong>the</strong>y also wanted110
Report to SDO for NCRS ProjectDiscussion8.2.2. Qualitative <strong>in</strong>terviews, Level 2Three out <strong>of</strong> four Trusts had implemented some sort <strong>of</strong> PACS system, but onlyTrust 4 had implemented ‘true’ PACS. Two Trusts had implemented e testorder<strong>in</strong>g and brows<strong>in</strong>g, but <strong>in</strong> one <strong>of</strong> <strong>the</strong>se (Trust 2) <strong>the</strong> system was so poor itwas hardly used so, <strong>in</strong> effect, had not been implemented.Draw<strong>in</strong>g on <strong>the</strong> literature on diffusion <strong>of</strong> <strong>in</strong>novations, we found that <strong>the</strong>re werefour, <strong>in</strong>ter-related factors which <strong>in</strong>fluenced <strong>the</strong> adoption <strong>of</strong> <strong>the</strong>se <strong>in</strong>novations:<strong>the</strong> attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation; <strong>the</strong> characteristics <strong>of</strong> <strong>the</strong> adopter;implementation processes; and organisational factors. In terms <strong>of</strong> <strong>the</strong>attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation, <strong>the</strong> speed, ease <strong>of</strong> use, reliability and <strong>the</strong> ability tocustomise were key issues. Thus PACS <strong>in</strong> Trust 4 was adopted much morewidely than <strong>in</strong> Trust 2; and e test order<strong>in</strong>g and brows<strong>in</strong>g was adopted muchmore quickly and effectively <strong>in</strong> Trust 1 than <strong>in</strong> Trust 2. Characteristics <strong>of</strong>adopters seemed to be most important <strong>in</strong> <strong>the</strong> early stages <strong>of</strong> implementationand so <strong>in</strong> all Trusts, <strong>the</strong> challenge <strong>of</strong> persuad<strong>in</strong>g potential users who were notfamiliar with us<strong>in</strong>g <strong>IT</strong> was raised. The way <strong>the</strong>se <strong>in</strong>novations wereimplemented was crucial to <strong>the</strong>ir use, <strong>in</strong> particular, <strong>the</strong> level <strong>of</strong> userconsultation <strong>in</strong> <strong>the</strong> implementation; <strong>the</strong> quality <strong>of</strong> tra<strong>in</strong><strong>in</strong>g and <strong>IT</strong> support; andwhe<strong>the</strong>r <strong>the</strong> <strong>in</strong>novations were implemented <strong>in</strong> terms <strong>of</strong> creat<strong>in</strong>g a ‘criticalmass’ <strong>of</strong> benefit. F<strong>in</strong>ally, <strong>the</strong>re were some key organisational factors which<strong>in</strong>fluenced <strong>the</strong> adoption <strong>of</strong> <strong>the</strong>se <strong>in</strong>novations, <strong>the</strong> most important <strong>of</strong> whichwere: that <strong>the</strong> designers and implementers <strong>of</strong> <strong>the</strong> <strong>in</strong>novation understood <strong>the</strong>bus<strong>in</strong>ess process <strong>the</strong> <strong>IT</strong> <strong>in</strong>novation was go<strong>in</strong>g to be used <strong>in</strong>; a strong projectmanagement team to implement with high level management support; and <strong>the</strong>level <strong>of</strong> team work<strong>in</strong>g with<strong>in</strong> and between departments and <strong>the</strong> ability <strong>of</strong> <strong>the</strong>organisation to work as a whole (for example, to implement a ‘critical mass’ <strong>of</strong><strong>the</strong> <strong>in</strong>novation).The perceived impact <strong>of</strong> <strong>the</strong>se <strong>in</strong>novations varied accord<strong>in</strong>g to <strong>the</strong> <strong>in</strong>novation,how <strong>the</strong>y had been implemented, and relate to <strong>the</strong> follow<strong>in</strong>g areas: patientexperience; work<strong>in</strong>g practices; and safety/governance. In all cases, <strong>the</strong>re werepositive and negative examples <strong>of</strong> <strong>the</strong>se reported, but overall, for PACS <strong>in</strong> allthree Trusts and e-test order<strong>in</strong>g <strong>in</strong> Trust 1, <strong>the</strong> positives appear to outweigh111
Report to SDO for NCRS ProjectDiscussion<strong>the</strong> negatives. Although, very little formal measurement <strong>of</strong> <strong>the</strong>seconsequences was carried out by <strong>the</strong> Trusts, for example, <strong>the</strong> reported<strong>in</strong>crease <strong>in</strong> <strong>the</strong> numbers <strong>of</strong> tests follow<strong>in</strong>g implementation <strong>of</strong> e-test order<strong>in</strong>gwas not quantified by Trust 1. These consequences are important, not leastbecause <strong>the</strong> perceived positive and negative impact <strong>of</strong> implement<strong>in</strong>g <strong>the</strong><strong>in</strong>novation <strong>in</strong>fluenced cont<strong>in</strong>ued use <strong>of</strong> <strong>the</strong> <strong>in</strong>novation and wider adoption.8.2.3. Quantitative effects <strong>of</strong> implementation <strong>of</strong> CPOE and PACSThe <strong>in</strong>vestigation <strong>of</strong> quantitative effects dist<strong>in</strong>guished primary outcomes,calculated from <strong>the</strong> number <strong>of</strong> diagnostic tests carried out, and secondaryoutcomes which were based on more general performance <strong>in</strong>dices. The size<strong>of</strong> <strong>the</strong> effects estimated was certa<strong>in</strong>ly potentially important, <strong>in</strong> <strong>the</strong> sense thatchanges <strong>in</strong> <strong>the</strong> volume <strong>of</strong> test order<strong>in</strong>g <strong>of</strong> 10 to 20% would have majorimplications if observed across <strong>the</strong> <strong>NHS</strong> dur<strong>in</strong>g roll out <strong>of</strong> <strong>the</strong> NationalProgramme. Our difficulties lay <strong>in</strong> dist<strong>in</strong>guish<strong>in</strong>g <strong>the</strong> effects from backgroundvariation <strong>in</strong> <strong>the</strong> performance <strong>in</strong>dices and <strong>in</strong> attribut<strong>in</strong>g those effects thatappeared to be ‘real’ to CPOE or PACS.The ma<strong>in</strong> effects <strong>of</strong> CPOE were <strong>in</strong> reduc<strong>in</strong>g <strong>the</strong> proportion <strong>of</strong> patients who hadany pathology test at outpatient appo<strong>in</strong>tments and <strong>the</strong> number <strong>of</strong> patients whohad <strong>the</strong> same test at <strong>the</strong>ir next outpatient appo<strong>in</strong>tments. These effects wereobserved to a greater or lesser extent for all tests that were <strong>in</strong>vestigated.These effects are plausible s<strong>in</strong>ce <strong>the</strong> CPOE system should allow a cl<strong>in</strong>ician toaccess a patient's pathology test history dur<strong>in</strong>g <strong>the</strong> outpatient appo<strong>in</strong>tment.There was some evidence that CPOE reduced <strong>the</strong> proportion <strong>of</strong> <strong>in</strong>patientshav<strong>in</strong>g pathology tests but this effect was not consistent across tests andbetween and with<strong>in</strong>-Trust comparisons.A similar effect with respect to repeat pla<strong>in</strong> X-ray films and US scans onsubsequent visits was observed when PACS was implemented. (Too fewpatients had a CT repeated to <strong>in</strong>vestigate <strong>the</strong> effect <strong>of</strong> PACS on this <strong>in</strong>dicatorfor this modality.) However, <strong>the</strong>re was no consistent effect on <strong>the</strong> overallproportion <strong>of</strong> patients who had a pla<strong>in</strong> X-ray film, CT or US scans at outpatientappo<strong>in</strong>tments. This may be because <strong>the</strong>se tests are less likely to be ordered112
Report to SDO for NCRS ProjectDiscussion<strong>in</strong> primary care, so patients would be unlikely to have previous test results. Inthis <strong>in</strong>terpretation, outpatient appo<strong>in</strong>tments at which imag<strong>in</strong>g tests werecarried out were effectively for <strong>the</strong> purpose <strong>of</strong> hav<strong>in</strong>g <strong>the</strong>se tests. As withCPOE, <strong>the</strong>re was possibly some evidence that PACS reduced <strong>the</strong> proportion<strong>of</strong> <strong>in</strong>patients hav<strong>in</strong>g imag<strong>in</strong>g tests but this was not consistent for between andwith<strong>in</strong>-Trust comparisons.A variety <strong>of</strong> changes <strong>in</strong> secondary outcomes were observed but attribution <strong>of</strong><strong>the</strong> changes to implementation <strong>of</strong> CPOE and PACS was more problematics<strong>in</strong>ce <strong>the</strong> hypo<strong>the</strong>sised cha<strong>in</strong> <strong>of</strong> causality l<strong>in</strong>k<strong>in</strong>g <strong>the</strong> application to <strong>the</strong>outcome was more tenuous. Secondary outcomes are likely to be strongly<strong>in</strong>fluenced by concurrent process changes and events <strong>in</strong> <strong>the</strong> participat<strong>in</strong>gTrusts.However, <strong>the</strong>re did appear to be a consistent reduction <strong>in</strong> <strong>the</strong>proportion <strong>of</strong> patients discharged at outpatient appo<strong>in</strong>tments after bothapplications were implemented.8.3. Strengths and weaknesses <strong>of</strong> <strong>the</strong> study8.3.1. Qualitative studyLevel 1 <strong>in</strong>terviewsThe <strong>the</strong>mes that emerged were communicated to us by <strong>in</strong>terviewees, withsupport<strong>in</strong>g <strong>in</strong>formation that showed <strong>the</strong>ir importance to <strong>the</strong> participat<strong>in</strong>gTrusts. In <strong>the</strong>se circumstances <strong>the</strong> validity <strong>of</strong> our f<strong>in</strong>d<strong>in</strong>gs is not <strong>in</strong> question,but <strong>the</strong> small number <strong>of</strong> cases makes us cautious about generalis<strong>in</strong>g morewidely. In support <strong>of</strong> <strong>the</strong> generalisability <strong>of</strong> <strong>the</strong> study, however, <strong>the</strong>circumstances <strong>of</strong> participat<strong>in</strong>g Trusts that were <strong>of</strong>ten <strong>the</strong> basis <strong>of</strong> managers’concerns are prevalent throughout <strong>the</strong> <strong>NHS</strong>: such as poor performance rat<strong>in</strong>gs(26% <strong>of</strong> acute Trusts have
Report to SDO for NCRS ProjectDiscussionwe cannot conclude that <strong>the</strong> issues highlighted <strong>in</strong> this report are <strong>the</strong> only ormost important ones.The small number <strong>of</strong> participat<strong>in</strong>g Trusts makes us cautious aboutgeneralis<strong>in</strong>g our f<strong>in</strong>d<strong>in</strong>gs. The Trusts studied are located <strong>in</strong> only two <strong>of</strong> <strong>the</strong>five geographic implementation clusters.However, uncerta<strong>in</strong>ty overtimetables and a lack <strong>of</strong> progress have been widely reported across all regions<strong>of</strong> England. 95Moreover, mergers <strong>of</strong> <strong>IT</strong> companies also mean that <strong>the</strong> Trustsstudied are be<strong>in</strong>g supplied by two <strong>of</strong> (now) four local service providers. 95Concerns raised by respondents, about performance and f<strong>in</strong>ance, areprevalent issues <strong>in</strong> <strong>the</strong> <strong>NHS</strong> but may be more salient <strong>in</strong> our participat<strong>in</strong>gTrusts than nationally.A fur<strong>the</strong>r limitation <strong>of</strong> this longitud<strong>in</strong>al study, was <strong>the</strong> degree <strong>of</strong> staff turnoverbetween <strong>the</strong> two stages. In <strong>the</strong> 18 months follow<strong>in</strong>g stage A, <strong>the</strong>re wereseveral changes <strong>in</strong> personnel; <strong>of</strong> <strong>the</strong> 23 staff orig<strong>in</strong>ally <strong>in</strong>terviewed <strong>in</strong> 2004,only 11 were still <strong>in</strong> post <strong>in</strong> 2006 (2 out <strong>of</strong> 4 chief executives, all 4 directors <strong>of</strong>nurs<strong>in</strong>g, 2 medical directors and 3 directors <strong>of</strong> <strong>in</strong>formation technology). This isan important context to <strong>the</strong> study itself, but means that <strong>the</strong>re are somediscont<strong>in</strong>uities <strong>in</strong> terms <strong>of</strong> <strong>in</strong>terview data.Set aga<strong>in</strong>st <strong>the</strong>se limitations, ours is <strong>the</strong> only <strong>in</strong>-depth, longitud<strong>in</strong>al study <strong>of</strong><strong>NHS</strong> <strong>IT</strong> <strong>modernisation</strong>. We <strong>in</strong>terviewed a cross section <strong>of</strong> senior Trust staffresponsible for implement<strong>in</strong>g <strong>the</strong> programme <strong>in</strong> <strong>NHS</strong> hospitals over a period <strong>of</strong>two years. These <strong>in</strong>terviews have provided us with a detailed account <strong>of</strong> <strong>the</strong>irviews about progress so far, <strong>the</strong> challenges <strong>the</strong>y perceive <strong>in</strong> implement<strong>in</strong>g <strong>the</strong>programme <strong>in</strong> <strong>NHS</strong> hospitals and <strong>the</strong>ir <strong>in</strong>formation needs, <strong>in</strong> address<strong>in</strong>g <strong>the</strong>sechallenges.Level 2 <strong>in</strong>terviewsWe were able to study <strong>the</strong> factors which affected adoption and <strong>the</strong> impact <strong>of</strong>two specific <strong>IT</strong> applications (PACS and CPOE) <strong>in</strong> some <strong>of</strong> our case studyTrusts. As implementation was limited (PACS was only fully implemented <strong>in</strong>one Trust, partially <strong>in</strong> two o<strong>the</strong>rs; CPOE was only fully implemented <strong>in</strong> oneTrust), this part <strong>of</strong> our study was not as large as we had hoped. As our focus114
Report to SDO for NCRS ProjectDiscussionwas on end-users’ experiences <strong>of</strong> <strong>the</strong>se <strong>IT</strong> applications, our use <strong>of</strong> <strong>the</strong><strong>in</strong>terview as method was appropriate, however we would have liked to havebeen able to <strong>in</strong>terview a wider range <strong>of</strong> end users had implementation beenmore widespread. We were able, however, to study <strong>the</strong> impact <strong>of</strong> partialimplementation <strong>of</strong> an <strong>IT</strong> application (PACS <strong>in</strong> two Trusts) compared to fullimplementation <strong>in</strong> ano<strong>the</strong>r, and compare unsuccessful implementation <strong>of</strong> an <strong>IT</strong>application (CPOE) <strong>in</strong> one Trust with relatively successful implementation <strong>in</strong>ano<strong>the</strong>r. This added to our understand<strong>in</strong>g <strong>of</strong> <strong>the</strong> factors which <strong>in</strong>fluenceadoption and diffusion.Our <strong>in</strong>tention had been to l<strong>in</strong>k <strong>the</strong> quantitative and qualitative data much morethan we have been able to achieve. This is partly because <strong>of</strong> <strong>the</strong> limitedamount <strong>of</strong> implementation and <strong>the</strong> focus <strong>of</strong> Level 1 <strong>of</strong> <strong>the</strong> qualitative study on<strong>the</strong> delayed implementation <strong>of</strong> NPf<strong>IT</strong>, and partly because <strong>of</strong> <strong>the</strong> length <strong>of</strong> timeit took us to access <strong>the</strong> quantitative data from <strong>the</strong> Trusts. We are able to l<strong>in</strong>ksome <strong>of</strong> <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs from <strong>the</strong> qualitative and quantitative studies on <strong>the</strong> impact<strong>of</strong> PACS and CPOE (see for example 7.5.1).8.3.2. Quantitative studyThe ma<strong>in</strong> limitations <strong>of</strong> <strong>the</strong> quantitative study relate to our ability to attributecausality to observed associations. We observed associations <strong>of</strong> substantialmagnitude, some beneficial and some adverse with respect to <strong>the</strong> efficiency <strong>of</strong>health care delivery, but few were ‘significant’ <strong>in</strong> a conventional statisticalsense. Moreover, even where we did f<strong>in</strong>d significant associations, we cannotnecessarily assume that <strong>the</strong>se arise from implementation <strong>of</strong> CPOE or PACS.In controlled before-and-after studies, one <strong>in</strong>vestigates how aggregatemeasures for a particular time period differ between ‘<strong>in</strong>tervention’ and ‘control’clusters, after adjust<strong>in</strong>g for ‘basel<strong>in</strong>e’ values <strong>of</strong> <strong>the</strong> aggregate measures forano<strong>the</strong>r time period when all clusters operated <strong>in</strong> a similar manner (ei<strong>the</strong>r allcontrol or all <strong>in</strong>tervention). With<strong>in</strong> each time period and cluster, outcomes areaggregated over many <strong>in</strong>dividuals. When analys<strong>in</strong>g such studies, it is vital totake <strong>in</strong>to account <strong>the</strong> cluster<strong>in</strong>g <strong>of</strong> <strong>in</strong>dividuals with<strong>in</strong> <strong>in</strong>stitutions (or o<strong>the</strong>rcluster unit); this can be done ei<strong>the</strong>r by analys<strong>in</strong>g <strong>the</strong> aggregate measures115
Report to SDO for NCRS ProjectDiscussion<strong>the</strong>mselves, or by analys<strong>in</strong>g <strong>the</strong> <strong>in</strong>dividual observations with appropriateadjustment to <strong>the</strong> standard errors calculated. (When we analysed <strong>the</strong> datawithout tak<strong>in</strong>g account <strong>of</strong> cluster<strong>in</strong>g, all effects were statistically significant.)The latter method has more statistical power; however, <strong>the</strong> former methodillustrates that our study was essentially a study with ‘n’=28 for between-Trustcomparisons (4 Trusts and 7 specialties, more for outpatients, although strictlyonly one <strong>in</strong>tervention Trust), and n=7 for with<strong>in</strong> Trust comparisons.Consideration <strong>of</strong> a controlled before and after study with only two <strong>in</strong>stitutions(which is <strong>of</strong>ten <strong>the</strong> case) also highlights <strong>the</strong> problem <strong>of</strong> <strong>in</strong>ferr<strong>in</strong>g causality;such a study may well f<strong>in</strong>d a highly significant effect but <strong>the</strong>re is no way <strong>of</strong>know<strong>in</strong>g whe<strong>the</strong>r <strong>the</strong> effect arises from implementation <strong>of</strong> <strong>the</strong> study<strong>in</strong>tervention or from some particular characteristic <strong>of</strong> <strong>the</strong> <strong>in</strong>stitution. Attribut<strong>in</strong>gcausality is streng<strong>the</strong>ned by us<strong>in</strong>g multiple clusters because <strong>the</strong> difference <strong>in</strong>aggregate outcome between <strong>in</strong>tervention and control clusters can be studiedaga<strong>in</strong>st <strong>the</strong> background context <strong>of</strong> variation <strong>in</strong> <strong>the</strong> outcome between allclusters.Statistical power is greatest when <strong>the</strong> numbers <strong>of</strong> <strong>in</strong>tervention and controlobservations are roughly equal.Obviously, we had no control overimplementation <strong>of</strong> CPOE and PACS and simply note that <strong>the</strong> unequalallocation <strong>of</strong> observations to <strong>in</strong>tervention and control groups meant that <strong>the</strong>study had less power than it might have had, if CPOE and PACS had beenimplemented more widely.We carried out both between- and with<strong>in</strong>-Trust comparisons as a check forconsistency.In effect, <strong>the</strong> latter represent analyses that control for <strong>the</strong>possibility that between-Trust f<strong>in</strong>d<strong>in</strong>gs arise from external factors affect<strong>in</strong>g only<strong>the</strong> <strong>in</strong>tervention (or control) Trusts. Remov<strong>in</strong>g one source <strong>of</strong> variation wouldnormally be expected to streng<strong>the</strong>n <strong>the</strong> analysis. However, <strong>in</strong> with<strong>in</strong>-Trustanalyses, <strong>the</strong> CPOE or PACS was only deployed (or withheld) <strong>in</strong> certa<strong>in</strong>specialties.Thus, <strong>the</strong>se analyses compared CPOE or PAC <strong>in</strong> somespecialties with no CPOE or PACS <strong>in</strong> o<strong>the</strong>r specialties and we cannot be surethat <strong>the</strong> opportunity for CPOE or PACS to <strong>in</strong>fluence <strong>the</strong> outcomes we studiedis <strong>the</strong> same for all specialties (a limitation which does not affect <strong>the</strong> betweenTrust comparisons).116
Report to SDO for NCRS ProjectDiscussionIf we had found many effects apparently associated with implementation <strong>of</strong>CPOE and PACS, we would have had to deal with <strong>the</strong> problem <strong>of</strong> attribut<strong>in</strong>gcausality many times. In <strong>the</strong> event, we only found a consistent effect <strong>of</strong> CPOEon outpatient test order<strong>in</strong>g, for which <strong>the</strong>re is a plausible explanation. Fur<strong>the</strong>r<strong>in</strong>vestigation <strong>of</strong> this effect, at a f<strong>in</strong>er level <strong>of</strong> detail or <strong>in</strong> a much larger sample<strong>of</strong> Trusts (with multiple Trusts implement<strong>in</strong>g CPOE), would be required to bemore confident that CPOE caused changes <strong>in</strong> test order<strong>in</strong>g. Conversely, thatwe did not f<strong>in</strong>d many effects associated with implementation <strong>of</strong> CPOE andPACS is both plausible and consistent with many o<strong>the</strong>r studies (see 8.4).We simply coded Trusts as implement<strong>in</strong>g CPOE and PACS or not, although<strong>the</strong> situation was more complex as has already been described. There is amore general issue <strong>of</strong> what, precisely, should be considered to represent an<strong>in</strong>novative <strong>IT</strong> application, especially when many applications are implemented<strong>in</strong> a stepped fashion. For example, changes <strong>in</strong> radiological imag<strong>in</strong>g <strong>of</strong>tenproceed from implementation <strong>of</strong> digital cameras, through digital storage, toeffective electronic communication <strong>of</strong> images over a more or less extendedperiod <strong>of</strong> time; similarly, electronic test order<strong>in</strong>g and brows<strong>in</strong>g functions arenot always implemented at <strong>the</strong> same time, and test order<strong>in</strong>g systems maydiffer substantially <strong>in</strong> <strong>the</strong>ir ability to implement restrictions on order<strong>in</strong>g on <strong>the</strong>basis <strong>of</strong> national or local guidel<strong>in</strong>es. Never<strong>the</strong>less, <strong>the</strong> key po<strong>in</strong>t here is that<strong>the</strong> slight lack <strong>of</strong> ‘purity’ <strong>in</strong> our classification <strong>of</strong> Trusts as <strong>in</strong>tervention andcontrol could only mean that any associations we observed wereunderestimates <strong>of</strong> <strong>the</strong> effects <strong>of</strong> CPOE and PACS.Although we restricted our between-Trust analyses to specialties common toall <strong>of</strong> <strong>the</strong> participat<strong>in</strong>g Trusts, our results rema<strong>in</strong> susceptible to residualconfound<strong>in</strong>g with<strong>in</strong> specialties due to differences <strong>in</strong> case-mix between Trusts.In with<strong>in</strong>-Trust comparisons, <strong>the</strong> analyses assumed constant case-mix overtime with<strong>in</strong> specialties.Our choice <strong>of</strong> outcomes was largely dictated by <strong>the</strong> data available from rout<strong>in</strong>esources. Therefore, we had to develop ‘proxy’ outcomes for <strong>the</strong> outcome wewanted to <strong>in</strong>vestigate, for example [redundant] ‘duplicate’ tests. We did nothave <strong>the</strong> level <strong>of</strong> detail necessary to determ<strong>in</strong>e whe<strong>the</strong>r tests repeated with<strong>in</strong>this <strong>in</strong>terval were actually redundant (e.g. redundant tests have typically been117
Report to SDO for NCRS ProjectDiscussionidentified by chart review). Our method <strong>of</strong> do<strong>in</strong>g this, e.g. retest with<strong>in</strong> 48hours, may not be equally applicable across specialties but we found noevidence to <strong>the</strong> contrary by compar<strong>in</strong>g <strong>the</strong> distributions <strong>of</strong> times to retest with<strong>in</strong>specialties. Our choice <strong>of</strong> <strong>in</strong>terval (48 hours) is also consistent with o<strong>the</strong>rstudies. 97-99 If some retests with<strong>in</strong> 48 hours are cl<strong>in</strong>ically necessary (as weexpect), and hence un<strong>in</strong>fluenced by CPOE, and some retests after 48 hoursare <strong>in</strong> truth duplicates, <strong>the</strong>se misclassifications could only mean that <strong>the</strong>association observed was an underestimate.It was not possible to verify data quality, although outpatient CDS data havebeen assessed as reliable. 96Pathology test and radiology exam<strong>in</strong>ation datawere unlikely to conta<strong>in</strong> significant omissions, s<strong>in</strong>ce <strong>the</strong>se were obta<strong>in</strong>eddirectly from pathology laboratory <strong>in</strong>formation systems (land radiology<strong>in</strong>formation systems (RIS) <strong>in</strong>to which all pathology tests and radiologicalexams were logged as standard operat<strong>in</strong>g procedure across all <strong>of</strong> <strong>the</strong> Trusts.More significant omissions may have arisen <strong>in</strong> us<strong>in</strong>g local patient identifiers tojo<strong>in</strong> <strong>the</strong>se data with <strong>the</strong> CDS data. We had no means to verify <strong>the</strong> reliability <strong>of</strong>this process, but <strong>the</strong> consistency <strong>of</strong> our outcome measures, both with<strong>in</strong> andbetween Trusts, gives us a reasonable degree <strong>of</strong> confidence.One <strong>of</strong> our biggest difficulties was obta<strong>in</strong><strong>in</strong>g background <strong>in</strong>formation on <strong>the</strong>implementation <strong>of</strong> applications, particularly <strong>in</strong> <strong>the</strong> control Trusts. Front-l<strong>in</strong>estaff <strong>in</strong> pathology and radiology departments were too heavily burdened withwork to respond to requests for <strong>in</strong>formation. Higher-level staff (managers andconsultants) expressed more <strong>in</strong>terested <strong>in</strong> <strong>the</strong> aims and ultimate success <strong>of</strong>our study, but lacked sufficiently detailed historical knowledge <strong>of</strong> systems <strong>in</strong><strong>the</strong>se departments.Hence we would be referred back to <strong>the</strong> samebeleaguered front-l<strong>in</strong>e staff who had been unable or unwill<strong>in</strong>g to respond toour orig<strong>in</strong>al requests. These shortcom<strong>in</strong>gs were compounded by <strong>in</strong>stitutionalamnesia as a result <strong>of</strong> high staff turnover, and by <strong>the</strong> demands <strong>of</strong> moreimmediate issues. (One consequence <strong>of</strong> <strong>the</strong> launch <strong>of</strong> NPf<strong>IT</strong> is that some <strong>of</strong><strong>the</strong> best <strong>IT</strong> staff with <strong>in</strong>side knowledge <strong>of</strong> <strong>the</strong> <strong>NHS</strong> were head-hunted by localservice providers, so <strong>the</strong>re was quite high turnover <strong>in</strong> local Trust <strong>IT</strong>Departments.)118
Report to SDO for NCRS ProjectDiscussionDespite <strong>the</strong>se limitations, we believe our study provides more valid andapplicable evidence <strong>of</strong> <strong>the</strong> effects <strong>of</strong> implement<strong>in</strong>g CPOE and PACSapplications than o<strong>the</strong>r studies have done. Our study was larger and broader<strong>in</strong> scope than previous ones and, despite small number <strong>of</strong> Trusts, broadlyrepresentative as we have argued above. The ‘controlled before-and-after’design is recognised as one <strong>of</strong> <strong>the</strong> best ways to take confound<strong>in</strong>g factors <strong>in</strong>toaccount (at <strong>the</strong> level <strong>of</strong> both <strong>the</strong> <strong>in</strong>stitution and <strong>in</strong>dividual observations). Ourlimited ability to <strong>in</strong>fer causality from <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs arose from <strong>the</strong> small number<strong>of</strong> Trusts we were able to <strong>in</strong>clude, not from <strong>the</strong> study design. In this firstattempt to carry out an evaluation on this scale, we were unable to recruitmore Trusts; it was difficult to obta<strong>in</strong> <strong>the</strong> data from Trusts and we onlyreceived <strong>the</strong> last batch <strong>of</strong> data required for <strong>the</strong> analyses <strong>in</strong> November 2006.What <strong>the</strong> study does demonstrate, however, are <strong>the</strong> opportunities for futureresearch us<strong>in</strong>g <strong>the</strong> same pr<strong>in</strong>ciples, as <strong>the</strong> roll-out <strong>of</strong> NPf<strong>IT</strong> picks up speed(see 8.5).8.3.3. Limitations affect<strong>in</strong>g <strong>the</strong> entire studyIn both <strong>of</strong> <strong>the</strong> preced<strong>in</strong>g sections, we acknowledge <strong>the</strong> limitations from hav<strong>in</strong>gonly four case study Trusts. Ano<strong>the</strong>r limitation <strong>of</strong> our study is <strong>the</strong> lack <strong>of</strong> aprimary care perspective. The NPf<strong>IT</strong> was conceived from <strong>the</strong> perspective <strong>of</strong><strong>the</strong> entire <strong>NHS</strong> <strong>in</strong> England, comb<strong>in</strong><strong>in</strong>g <strong>the</strong> goals <strong>of</strong> <strong>the</strong> orig<strong>in</strong>al episodefocusedelectronic patient record and <strong>the</strong> longitud<strong>in</strong>al, cradle-to-grave healthrecord.[ENlib#1] Realisation <strong>of</strong> this vision requires equal commitment from allsectors <strong>of</strong> <strong>the</strong> <strong>NHS</strong>. We tried to address <strong>the</strong> primary secondary <strong>in</strong>terface bystudy<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> Choose and Book but were unable to do so <strong>in</strong>detail because this application was not <strong>in</strong>troduced to a significant extent byany <strong>of</strong> <strong>the</strong> Trusts that we studied.8.4. F<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> <strong>the</strong> context <strong>of</strong> exist<strong>in</strong>g literature8.4.1. Qualitative studyExperiences <strong>of</strong> <strong>IT</strong> implementation <strong>in</strong> <strong>the</strong> UK 101 and o<strong>the</strong>r countries confirm <strong>the</strong>importance <strong>of</strong> sociocultural considerations. A case study from Australia119
Report to SDO for NCRS ProjectDiscussiondescribed a major failure <strong>of</strong> <strong>IT</strong> implementation, identify<strong>in</strong>g organisational andcultural factors that led to <strong>the</strong> failure as well as technical ones, with <strong>the</strong> systemfail<strong>in</strong>g to meet staff expectations. 12 In <strong>the</strong> United States <strong>in</strong>troduction <strong>of</strong> <strong>the</strong>“computer physician order entry” led users to feel that <strong>the</strong>ir work was disruptedand not facilitated and that <strong>the</strong> organisation ga<strong>in</strong>ed more than <strong>the</strong>y did, 33 withreports <strong>of</strong> an adverse impact on team relationships. 34This was mirrored <strong>in</strong> ourstudy <strong>of</strong> <strong>the</strong> experience <strong>of</strong> <strong>the</strong> failure <strong>of</strong> implementation <strong>of</strong> CPOE <strong>in</strong> Trust 2.There are also major technical and logistical challenges to implementation, butNPf<strong>IT</strong> project managers have shown commitment to deal<strong>in</strong>g with <strong>the</strong>se. 102However, <strong>the</strong> sociocultural challenges are daunt<strong>in</strong>g, 25,26,28 and we found thatsenior <strong>NHS</strong> staff felt <strong>the</strong>se to have been neglected. One concern is that staffwill not experience tangible benefits <strong>in</strong> <strong>the</strong> near future, 7,20but will have tocope with disruption, uncerta<strong>in</strong>ty, and change, and possibly a loss <strong>of</strong> <strong>IT</strong>functionality <strong>in</strong> <strong>the</strong> short term. In <strong>the</strong>se circumstances, a more sophisticatedapproach is needed to ga<strong>in</strong> <strong>the</strong> cooperation <strong>of</strong> front l<strong>in</strong>e staff, on whomsuccess will depend.The programme <strong>in</strong> wider contextGPs derive substantial benefits from us<strong>in</strong>g <strong>IT</strong> systems to support <strong>the</strong> day-todayrunn<strong>in</strong>g <strong>of</strong> <strong>the</strong>ir practices. These systems have been designed to meet<strong>the</strong> small-bus<strong>in</strong>ess needs <strong>of</strong> GPs and to underp<strong>in</strong> relatively simple cl<strong>in</strong>icalfunctions, 104 allow<strong>in</strong>g GPs to run <strong>the</strong>ir practices efficiently and autonomously.Therefore, GPs may perceive that <strong>the</strong>y will not benefit substantially from <strong>the</strong>programme and, more importantly, may not want applications <strong>of</strong> <strong>the</strong>programme imposed on <strong>the</strong>m. 105By contrast, acute hospital Trusts have to deal with more urgent and complexdemands, requir<strong>in</strong>g fast communication between hundreds <strong>of</strong> staff acrossmany specialties and pr<strong>of</strong>essional discipl<strong>in</strong>es and, <strong>in</strong> emergency situations,between hospitals and health sectors.Although <strong>the</strong>ir <strong>IT</strong> systems havehistorically been poorly <strong>in</strong>tegrated, <strong>the</strong>y stand to benefit hugely from<strong>modernisation</strong>, not least <strong>in</strong> achiev<strong>in</strong>g <strong>the</strong> efficiencies currently be<strong>in</strong>gdemanded <strong>of</strong> <strong>the</strong>m.For managers and cl<strong>in</strong>icians <strong>in</strong> acute Trusts, <strong>the</strong>programme has to work. There is no alternative, <strong>in</strong>dependent procurement <strong>of</strong>120
Report to SDO for NCRS ProjectDiscussion<strong>IT</strong> systems, <strong>in</strong> <strong>the</strong> absence <strong>of</strong> national standards, hav<strong>in</strong>g already been triedwith limited success. 106Implementation <strong>of</strong> Choose & Book illustrates <strong>the</strong>se differ<strong>in</strong>g perspectives.Senior Trust staff reported that achiev<strong>in</strong>g “seamless connectivity” betweenprimary and secondary care was a major obstacle, <strong>in</strong> addition to technicalproblems, and a lack <strong>of</strong> support for <strong>the</strong> concept <strong>of</strong> patient choice. There wasno <strong>in</strong>tegration <strong>of</strong> Trust and GP <strong>IT</strong> systems and acute Trust staff were unable toreconcile implementation timetables and goals for Choose & Book with <strong>the</strong>irprimary care colleagues. Many GPs did not accept <strong>the</strong> concept and couldchoose not to. 1078.4.2. Quantitative studyIt is clear from 8.2.3 that our strongest and most plausible f<strong>in</strong>d<strong>in</strong>g is thatimplementation <strong>of</strong> an CPOE system was associated with a much slowerupward trend <strong>in</strong> <strong>the</strong> proportion <strong>of</strong> outpatient appo<strong>in</strong>tments at which FBC, UEand UR pathology tests were ordered, and at which FBC tests were possiblyre-ordered.We conducted a literature search to identify comparable studies. For CPOE,this search was pre-empted by a fairly recent systematic review, to which weappended our own review <strong>of</strong> more recent publications. As might be expected,papers report<strong>in</strong>g issues around <strong>the</strong> implementation <strong>of</strong> health care <strong>IT</strong> systemsare be<strong>in</strong>g published at a rapidly <strong>in</strong>creas<strong>in</strong>g rate. As might also be expected,<strong>the</strong>re is little consistency <strong>in</strong> <strong>the</strong>ir f<strong>in</strong>d<strong>in</strong>gs, and studies vary widely <strong>in</strong>perspective, sett<strong>in</strong>g, size, and design.In <strong>the</strong> systematic review, CPOE was associated with reduced pathology testvolumes <strong>in</strong> 7 out <strong>of</strong> 11 studies, with no change <strong>in</strong> 3 studies, and with an<strong>in</strong>crease <strong>in</strong> one study. 18 Only one <strong>of</strong> <strong>the</strong> studies (show<strong>in</strong>g reduced volume),was performed <strong>in</strong> outpatients departments, and <strong>the</strong> <strong>in</strong>tervention evaluated <strong>in</strong>this study was a module added to an exist<strong>in</strong>g CPOE system to display testcharges. 85 We found one additional study (by <strong>the</strong> same author), <strong>in</strong> a USprimary care sett<strong>in</strong>g, which reported a reduction <strong>in</strong> order<strong>in</strong>g <strong>of</strong> six types <strong>of</strong>pathology tests (<strong>in</strong>clud<strong>in</strong>g FBC, UE and UC), and requests for two types <strong>of</strong>121
Report to SDO for NCRS ProjectDiscussionradiology exam<strong>in</strong>ations, if previous test or exam results were displayed. Thisresult was for <strong>the</strong> study overall; <strong>the</strong> slight decrease <strong>in</strong> FBC and UE test orderswas not analysed separately. UC test orders showed a slight <strong>in</strong>crease. 108A recent study, <strong>in</strong>volv<strong>in</strong>g <strong>the</strong> same CPOE system as was deployed <strong>in</strong> our<strong>in</strong>tervention Trust (but look<strong>in</strong>g at <strong>in</strong>patient tests for liver function and plasmagentamic<strong>in</strong> and vancomyc<strong>in</strong> levels), found no change <strong>in</strong> test order volumes 109 .Interest<strong>in</strong>gly, this study did f<strong>in</strong>d o<strong>the</strong>r changes (<strong>in</strong> turnaround time, <strong>in</strong><strong>in</strong>formation provided with specimens, and <strong>in</strong> order<strong>in</strong>g <strong>of</strong> tests removed from anorder set), which suggest that changes may occur at a level <strong>of</strong> detail beneathour outcomes. That this level <strong>of</strong> detail may be requisite <strong>in</strong> design<strong>in</strong>g studies toassess <strong>the</strong> impact <strong>of</strong> <strong>IT</strong> systems on health care provision, is best exemplifiedby a study <strong>of</strong> test utilization <strong>in</strong> a coronary care unit. 110The <strong>in</strong>tervention <strong>in</strong> thisstudy comprised new cl<strong>in</strong>ical guidel<strong>in</strong>es on test order<strong>in</strong>g, which were devisedfor <strong>the</strong> study and dissem<strong>in</strong>ated throughout, and modifications to an exist<strong>in</strong>gCPOE system. The study outcomes were specific to coronary <strong>in</strong>tensive care,and <strong>the</strong> <strong>in</strong>tervention and control care units were closely matched. The studydid f<strong>in</strong>d that <strong>the</strong> <strong>in</strong>tervention was associated with reduced test orders.Our study did not demonstrate effects on radiological exam<strong>in</strong>ation requestbehaviour which could be readily attributed to implementation <strong>of</strong> PACS. In <strong>the</strong>absence <strong>of</strong> a systematic review on this subject, we found one comparablestudy, which reported <strong>in</strong>creases <strong>in</strong> <strong>in</strong>patient and outpatient utilization <strong>of</strong>radiological services compar<strong>in</strong>g one North American hospital with ano<strong>the</strong>rhospital, and with <strong>the</strong> national average. 111However, none <strong>of</strong> <strong>the</strong>secomparisons were supported by statistical tests with which to measure <strong>the</strong>strength <strong>of</strong> evidence. We also found a study with<strong>in</strong> a UK hospital, whichreported some improvements <strong>in</strong> radiology department performance, <strong>in</strong>clud<strong>in</strong>ga slight reduction <strong>in</strong> <strong>the</strong> repeat imag<strong>in</strong>g rate. 56O<strong>the</strong>r studies were ei<strong>the</strong>rqualitative or exam<strong>in</strong>ed o<strong>the</strong>r outcomes; those which exam<strong>in</strong>ed length-<strong>of</strong>-stayfound no impact <strong>of</strong> PACS. 56,112,113We should not be discouraged that our study jo<strong>in</strong>ed almost all previousstudies <strong>in</strong> fail<strong>in</strong>g to detect any consistent or plausible beneficial impact <strong>of</strong>CPOE or PACS on outcomes such as <strong>in</strong>patient length-<strong>of</strong>-stay and mortality. Insome sense, <strong>the</strong>se outcomes served as negative controls, to ensure that our122
Report to SDO for NCRS ProjectDiscussion<strong>in</strong>tervention Trusts were not affected by major process changes which mightconfound any associations we found with our primary outcomes. For example,deployment <strong>of</strong> CPOE with<strong>in</strong> Trust A co<strong>in</strong>cided with construction <strong>of</strong> a newhospital under a government Private F<strong>in</strong>ance Initiative (PFI). A more cogentargument is that, while CPOE systems and PACS may br<strong>in</strong>g importantqualitative improvements to <strong>the</strong> process <strong>of</strong> cl<strong>in</strong>ical care (particularly <strong>in</strong> mak<strong>in</strong>glife easier for cl<strong>in</strong>icians), <strong>the</strong>se benefits are difficult to quantify and detect on amacroscopic (hospital-wide or Trust-wide) scale.8.5. Research agendaThis study has shown that it is possible to use rout<strong>in</strong>ely collected patient-leveldata from disparate sources with<strong>in</strong> very large health care <strong>in</strong>stitutions as a basisfor assess<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> technological changes on <strong>in</strong>dicators <strong>of</strong> cl<strong>in</strong>ical activityand operational efficiency. In <strong>the</strong> context <strong>of</strong> future research with<strong>in</strong> <strong>the</strong> UK <strong>NHS</strong>,<strong>the</strong> transmission <strong>of</strong> local (Trust-level) patient identifiers <strong>in</strong> CDS data to NWCS,and <strong>the</strong> improv<strong>in</strong>g availability <strong>of</strong> datasets from specialist departments with<strong>in</strong>Trusts, suggests that our technique <strong>of</strong> jo<strong>in</strong><strong>in</strong>g CDS data with <strong>the</strong>se specialistdatasets could form <strong>the</strong> basis for operational research on a nationwide scale. Forexample, <strong>the</strong> impact <strong>of</strong> new NPf<strong>IT</strong> functions could be assessed by compar<strong>in</strong>gTrusts randomly selected from <strong>the</strong> group <strong>of</strong> early-adopters with a randomselection <strong>of</strong> Trusts yet to implement <strong>the</strong> function. This method could be applied tochanges o<strong>the</strong>r than <strong>the</strong> implementation <strong>of</strong> new technologies, and to much largergroups <strong>of</strong> Trusts.This is an excit<strong>in</strong>g prospect s<strong>in</strong>ce <strong>the</strong> analyses are entirely feasible. The keyrequirement, <strong>in</strong> addition to a mandate to provide <strong>the</strong> necessary data, is extremelycareful documentation <strong>of</strong> <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> applications over time, bothwith respect to tim<strong>in</strong>g and details <strong>of</strong> exactly what is be<strong>in</strong>g implemented. Inpr<strong>in</strong>ciple, <strong>the</strong> <strong>NHS</strong> provides an appropriate sett<strong>in</strong>g to use an even stronger studydesign, e.g. a cluster randomised controlled trial or ‘stepped-wedge’ design (<strong>the</strong>same pr<strong>in</strong>ciples as <strong>the</strong> controlled before and after study but with randomisation <strong>of</strong>hospitals to implement earlier or later), but this would a require a level <strong>of</strong> nationalcontrol <strong>of</strong> <strong>the</strong> implementation schedule across Trusts that is probably notachievable on both logistical and political grounds.123
Report to SDO for NCRS ProjectDiscussionFor this method to succeed, it is very important to study a large number <strong>of</strong> Trusts.Aga<strong>in</strong>, this is entirely feasible provid<strong>in</strong>g that rout<strong>in</strong>e data for Trusts can l<strong>in</strong>ked <strong>in</strong>similar ways, without <strong>the</strong> need to customise data management tasks. A largenumber <strong>of</strong> participat<strong>in</strong>g Trusts will improve statistical precision <strong>in</strong> <strong>the</strong> conventionalmanner. More importantly, however, it will also allow variation betweenimplement<strong>in</strong>g and non-implement<strong>in</strong>g Trusts to be described <strong>in</strong> a morerepresentative manner. Variation between Trusts is critical because variation atthis level provides <strong>the</strong> basis for <strong>in</strong>ference about <strong>the</strong> statistical significance <strong>of</strong>differences between implement<strong>in</strong>g and non-implement<strong>in</strong>g Trusts; hav<strong>in</strong>g datafrom a large number <strong>of</strong> Trusts makes statistical <strong>in</strong>ferences more applicable.F<strong>in</strong>ally, hav<strong>in</strong>g a large number <strong>of</strong> participat<strong>in</strong>g Trusts gives greater confidence <strong>in</strong>attribution <strong>of</strong> effects to <strong>IT</strong> <strong>modernisation</strong> (or o<strong>the</strong>r organisation wide <strong>in</strong>novation ortechnology); artefacts would have to be widespread, associated with <strong>the</strong> chosen<strong>in</strong>dicators, and co<strong>in</strong>cide with implementation <strong>in</strong> <strong>the</strong> majority <strong>of</strong> Trusts (notnecessarily at <strong>the</strong> same po<strong>in</strong>t <strong>in</strong> calendar time), for <strong>the</strong>ir effects to be confusedwith those aris<strong>in</strong>g from implement<strong>in</strong>g <strong>IT</strong> <strong>modernisation</strong>.Large scale quantitative studies alone are, however, unlikely to provide all <strong>of</strong> <strong>the</strong><strong>in</strong>formation required. The difficulty that we experienced <strong>in</strong> attribut<strong>in</strong>g effects to <strong>IT</strong><strong>modernisation</strong> arose not simply because <strong>of</strong> <strong>the</strong> small number <strong>of</strong> participat<strong>in</strong>gTrusts but also because we had a poorly developed understand<strong>in</strong>g <strong>of</strong> <strong>the</strong> way <strong>in</strong>which <strong>IT</strong> applications impact on health care. Qualitative studies, such as level 2<strong>in</strong>terviews, provide this understand<strong>in</strong>g and can <strong>in</strong>form both <strong>the</strong> design and<strong>in</strong>terpretation <strong>of</strong> quantitative studies.Our study shows <strong>the</strong> usefulness <strong>of</strong> us<strong>in</strong>g qualitative methods to study processes<strong>of</strong> implementation at a local level. Multiple case studies, such as this one, provideuseful analyses both with<strong>in</strong> and across case studies, for example compar<strong>in</strong>gwhere implementation has gone well and less well. Longitud<strong>in</strong>al studies areimportant <strong>in</strong> study<strong>in</strong>g implementation processes, and <strong>in</strong> <strong>the</strong> case <strong>of</strong> implement<strong>in</strong>gcomplex <strong>in</strong>novations with<strong>in</strong> large systems, studies need to be conducted oversignificant time periods i.e. at least 5 years.Development <strong>of</strong> appropriate outcome measures provides one example <strong>of</strong> <strong>the</strong> way<strong>in</strong> which qualitative and quantitative methods should be comb<strong>in</strong>ed. One approachto <strong>the</strong> choice <strong>of</strong> outcomes (and, effectively, <strong>the</strong> one that we adopted) is simply to124
Report to SDO for NCRS ProjectDiscussionstudy <strong>in</strong>dices which are available, easily derived from rout<strong>in</strong>e sources or whichpolicy makers aspire to <strong>in</strong>fluence for reasons <strong>of</strong> face validity. 54A secondapproach is to base outcomes on feedback from users with experience <strong>of</strong> servicedelivery and <strong>IT</strong> applications, develop<strong>in</strong>g outcomes to reflect aspects <strong>of</strong> servicedelivery which <strong>the</strong> users <strong>the</strong>mselves consider important to <strong>the</strong>ir ways <strong>of</strong> work<strong>in</strong>gand which <strong>the</strong>y believe are <strong>in</strong>fluenced by <strong>IT</strong> <strong>modernisation</strong>.One major evidence gap, <strong>of</strong> particular importance to senior managers <strong>in</strong> <strong>NHS</strong>organisations faced with implement<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> and <strong>the</strong> levels <strong>of</strong> uncerta<strong>in</strong>tyalready described, is <strong>the</strong> absence <strong>of</strong> high quality evaluations <strong>of</strong> <strong>the</strong> economicimplications <strong>of</strong> implement<strong>in</strong>g organisation-wide <strong>IT</strong> applications. One reason for<strong>the</strong> lack <strong>of</strong> studies is <strong>the</strong> lack <strong>of</strong> high quality studies (us<strong>in</strong>g designs with goodvalidity and which are well executed) <strong>of</strong> <strong>the</strong> resource consequences <strong>of</strong>implementation. However, <strong>the</strong> economic evaluations that we reviewed were also<strong>of</strong> poor quality from <strong>the</strong> po<strong>in</strong>t <strong>of</strong> view <strong>of</strong> <strong>the</strong> economic methods used.We do not <strong>in</strong>tend to criticise <strong>the</strong>se studies unth<strong>in</strong>k<strong>in</strong>gly. We acknowledge that<strong>the</strong>re is a paradox.One <strong>the</strong> one hand, <strong>the</strong>re is an urgent need for betterevaluations <strong>of</strong> <strong>the</strong> economic and f<strong>in</strong>ancial consequences <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> tohelp plan implementation, yet it is not clear that <strong>the</strong> methods conventionally usedfor economic evaluation are applicable to such large scale and complex<strong>in</strong>terventions.research should:We recommend that, <strong>in</strong> plann<strong>in</strong>g future economic evaluations,• Be clear about <strong>the</strong> precise question that needs to be addressed.• Def<strong>in</strong>e precisely <strong>the</strong> nature <strong>of</strong> <strong>the</strong> <strong>in</strong>tervention, for example with respect to itsscale, <strong>the</strong> extent <strong>of</strong> <strong>in</strong>tegration between different components. It is importantto remember that <strong>IT</strong> applications are not necessarily equally effective, as weobserved.• Wherever possible, aim to study and value <strong>the</strong> health consequences as wellas resource consequences <strong>of</strong> <strong>IT</strong> implementation.• Study carefully <strong>the</strong> transition from <strong>the</strong> exist<strong>in</strong>g method <strong>of</strong> provid<strong>in</strong>g health to<strong>the</strong> new method based on <strong>the</strong> <strong>in</strong>tervention be<strong>in</strong>g studied, while at <strong>the</strong> sametime study<strong>in</strong>g <strong>the</strong> <strong>in</strong>tervention longitud<strong>in</strong>ally for a sufficient period <strong>of</strong> time toobserve <strong>the</strong> k<strong>in</strong>ds <strong>of</strong> effects that are hypo<strong>the</strong>sised.125
Report to SDO for NCRS ProjectDiscussionThis study has taken place at <strong>the</strong> very beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> <strong>the</strong> process <strong>of</strong> attempt<strong>in</strong>g toimplement a national <strong>IT</strong> system at local level, and provides useful lessons for <strong>the</strong>future. Given <strong>the</strong> delays <strong>in</strong> implementation which we have described, we have notbeen able to study processes, such as changes <strong>in</strong> work<strong>in</strong>g practices, to <strong>the</strong>degree we would have liked. Whichever way <strong>IT</strong> policy develops <strong>in</strong> <strong>the</strong> future, it willbe important to cont<strong>in</strong>ue to study <strong>the</strong> processes <strong>of</strong> implementation and <strong>the</strong> impact<strong>the</strong>y have on organisations, teams, and patient care.With respect to specific research questions (see below), we strongly recommendcont<strong>in</strong>uity <strong>of</strong> research similar to this project as NPf<strong>IT</strong> is rolled out. Quantify<strong>in</strong>g <strong>the</strong>effects <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> is very important <strong>in</strong> order to relieve <strong>the</strong> prevail<strong>in</strong>guncerta<strong>in</strong>ty, which <strong>in</strong> turn should promote uptake.Therefore, we <strong>of</strong>fer noapologies for recommend<strong>in</strong>g new research questions us<strong>in</strong>g <strong>the</strong> same methods,which we believe have been successful. It should be noted that we were unableto study implementation <strong>of</strong> NPf<strong>IT</strong> because <strong>of</strong> delays and this, ra<strong>the</strong>r than localimplementation <strong>of</strong> stand-alone applications, is <strong>the</strong> real <strong>in</strong>novation. Features <strong>of</strong> <strong>the</strong>NPf<strong>IT</strong>, such as <strong>the</strong> broad standardisation <strong>of</strong> applications and <strong>the</strong>ir <strong>in</strong>tegrateddesign, means that f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> our study cannot necessarily be generalised toNPf<strong>IT</strong>.A. Develop a framework for record<strong>in</strong>g <strong>the</strong> detailed implementation <strong>of</strong> NPf<strong>IT</strong> <strong>in</strong> all<strong>NHS</strong> Trusts, toge<strong>the</strong>r with a system for logg<strong>in</strong>g bus<strong>in</strong>ess cases for local <strong>IT</strong>expenditure relat<strong>in</strong>g to implementation <strong>of</strong> NPf<strong>IT</strong>. This framework is vital forany comparative study <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong> across <strong>the</strong> <strong>NHS</strong>.B. Develop <strong>in</strong>dicators which reflect important impacts <strong>of</strong> implement<strong>in</strong>g <strong>IT</strong>applications and potentially important health consequences for patients. Theresearch should use Delphi or consensus-like methods, br<strong>in</strong>g<strong>in</strong>g toge<strong>the</strong>rpeople with knowledge <strong>of</strong> rout<strong>in</strong>e <strong>NHS</strong> datasets, local directorate databases,<strong>IT</strong> implementation, workforce tra<strong>in</strong><strong>in</strong>g and plann<strong>in</strong>g, users (cl<strong>in</strong>icians ando<strong>the</strong>rs), patients, risk assessors, etc.C. Quantify <strong>the</strong> effects <strong>of</strong> implement<strong>in</strong>g new PAS systems which are compatiblewith NPf<strong>IT</strong>. The research should use quantitative methods as <strong>in</strong> this project,l<strong>in</strong>ked to PAS <strong>in</strong>stallation timetables from LSPs / cluster adm<strong>in</strong>istrators. Thetime period studied should be long enough to allow description <strong>of</strong>: (a) a stable126
Report to SDO for NCRS ProjectDiscussionbasel<strong>in</strong>e, (b) <strong>the</strong> period <strong>of</strong> implementation, (c) a short post-implementationperiod (1 year), (d) a long post-implementation period (2-3 years).duration required means that <strong>the</strong> study will need to be partly retrospective, andpartly prospective. We suggest that exist<strong>in</strong>g <strong>in</strong>dicators would be satisfactoryto address this research question.TheQualitative methods could be used <strong>in</strong>parallel to study implementation processes <strong>in</strong> detail, for example: <strong>in</strong>volvement<strong>of</strong> end users <strong>in</strong> <strong>the</strong> process, <strong>in</strong> formulat<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g requirements and <strong>in</strong>tra<strong>in</strong><strong>in</strong>g itself; impact on patient access, e.g. facilitation <strong>of</strong> improvements <strong>in</strong>wait<strong>in</strong>g times, <strong>in</strong> particular <strong>the</strong> 18 week target; impact on cl<strong>in</strong>ical work, e.g.benefits/disbenefits for patient safety; impact on pr<strong>of</strong>essional relationships,e.g. team work<strong>in</strong>g, <strong>in</strong> both <strong>the</strong> short and long term.D. Quantify <strong>the</strong> effects <strong>of</strong> implement<strong>in</strong>g <strong>of</strong> NPf<strong>IT</strong> approved ‘bolt on’applications. The study would aga<strong>in</strong> use similar quantitative methods but,potentially, us<strong>in</strong>g more relevant, appropriate or important <strong>in</strong>dicators (seeB). The same issue about <strong>the</strong> duration <strong>of</strong> study applies here as above(see C). We strongly recommend that <strong>the</strong> study should use qualitativemethods <strong>in</strong> parallel, as we did <strong>in</strong> this project, specifically to studyvariation/discrepancies between Trusts dur<strong>in</strong>g periods (b), (c) and (d). Thequalitative research could study implementation processes, as <strong>in</strong> C, butcould also explore [relative] successes and failures, to provide lessonsabout good practice. Selection <strong>of</strong> case studies for <strong>the</strong> qualitative research,would need to be <strong>in</strong>formed by <strong>the</strong> quantitative research (i.e. extremes <strong>of</strong>variation). Tim<strong>in</strong>g <strong>of</strong> <strong>the</strong> qualitative field work would also be critical, toensure memories <strong>of</strong> important issues were fresh and that f<strong>in</strong>d<strong>in</strong>gs could bereported sufficiently quickly for lessons to be applied.E. Investigate synergies between NPf<strong>IT</strong> approved applications. This projectwould build on A and B, us<strong>in</strong>g both quantitative and qualitative methods. Theaim would be to identify whe<strong>the</strong>r <strong>the</strong> co-implementation and use <strong>of</strong> multipleapplications is associated with different effects compared to when applicationsare implemented s<strong>in</strong>gly. This research question is key to understand<strong>in</strong>g <strong>the</strong>wider impact <strong>of</strong> <strong>IT</strong> <strong>modernisation</strong>. We do not have a def<strong>in</strong>ite prior hypo<strong>the</strong>sis.It is possible that co-implementation <strong>of</strong> applications produces an overall effectthat is smaller than <strong>the</strong> simple additive effect <strong>of</strong> <strong>the</strong> implementations127
Report to SDO for NCRS ProjectDiscussionseparately, because some shared effects can’t be realised twice.Alternatively, co-implementation <strong>of</strong> applications might produce effects overand-abovea simple additive effect, because <strong>of</strong> synergy between applications.F. Commission research <strong>in</strong>to methods for evaluat<strong>in</strong>g <strong>the</strong> economicconsequences <strong>of</strong> implement<strong>in</strong>g organisation-wide technologies/systems. Werecognise that this is a very broad question, which is likely to requireconsiderable ref<strong>in</strong>ement through discussion with economists.8.6. Implications for a National <strong>IT</strong> SystemMany health systems aim to realise <strong>the</strong> potential benefits <strong>of</strong> health care <strong>IT</strong>through <strong>the</strong> widespread implementation <strong>of</strong> electronic health care records. Thenational programme was conceived from <strong>the</strong> perspective <strong>of</strong> <strong>the</strong> entire <strong>NHS</strong> <strong>in</strong>England, comb<strong>in</strong><strong>in</strong>g <strong>the</strong> goals <strong>of</strong> <strong>the</strong> orig<strong>in</strong>al episode-focused electronic patientrecord and <strong>the</strong> longitud<strong>in</strong>al, cradle-to-grave health record. 1 The debate is howbest to achieve this. An important lesson to emerge from our study <strong>of</strong> NPf<strong>IT</strong>implementation is <strong>the</strong> difficulty <strong>in</strong> achiev<strong>in</strong>g an appropriate balance <strong>of</strong>responsibility between government and local health care systems. As <strong>the</strong>experience <strong>of</strong> <strong>IT</strong> implementation <strong>in</strong> this country illustrates, devolv<strong>in</strong>g control <strong>of</strong> <strong>IT</strong>to local managers results <strong>in</strong> a lack <strong>of</strong> standards, and disparate functionality.Central control is equally problematic, with <strong>the</strong> sheer size <strong>of</strong> <strong>the</strong> task mak<strong>in</strong>gcommunication and realistic goal sett<strong>in</strong>g difficult.NPf<strong>IT</strong> has not made <strong>the</strong> progress that was expected. 44 However, <strong>the</strong> views <strong>of</strong>senior <strong>NHS</strong> staff <strong>in</strong> our study represent a warn<strong>in</strong>g <strong>of</strong> <strong>the</strong> cont<strong>in</strong>u<strong>in</strong>g challengesahead. The process <strong>of</strong> implementation needs to change rapidly for <strong>NHS</strong> staff t<strong>of</strong>eel optimistic and to embrace <strong>IT</strong> changes with enthusiasm. Moreover, attribut<strong>in</strong>gbenefits unequivocally to <strong>the</strong> NPf<strong>IT</strong> is likely to be difficult and to take time. 24,100The latest strategy <strong>in</strong> this country <strong>in</strong>volves a third approach, sett<strong>in</strong>g centralstandards but with local implementation. As recommended by <strong>the</strong> BritishComputer Society, 114 CfH’s role is shift<strong>in</strong>g away from implementation towardsprovid<strong>in</strong>g a national <strong>in</strong>frastructure and standards-sett<strong>in</strong>g body. Implementation willnow be devolved more locally, as set out <strong>in</strong> <strong>the</strong> <strong>NHS</strong> national bus<strong>in</strong>ess plan for2007/08. 115 Even with <strong>the</strong>se changes, <strong>the</strong> issues raised <strong>in</strong> our study still need to128
Report to SDO for NCRS ProjectDiscussionbe addressed.CfH, <strong>in</strong> its new guise, needs to <strong>in</strong>volve local end users <strong>in</strong>discussions about what form <strong>the</strong> national <strong>in</strong>frastructure should take and <strong>in</strong>develop<strong>in</strong>g national standards – <strong>the</strong>se should not be imposed above, as thiswould only repeat mistakes that have already been made. Fur<strong>the</strong>r, devolv<strong>in</strong>gresponsibility for implementation locally raises question about <strong>the</strong> degree <strong>of</strong> localcustomisation permitted. As we found <strong>in</strong> our study <strong>of</strong> PACS and CPOE, localcustomisation is an important factor <strong>in</strong> successful adoption however, too muchcustomisation might weaken national standards and <strong>the</strong> ability to pass databetween providers. F<strong>in</strong>ally, a national <strong>in</strong>frastructure should <strong>in</strong>clude help<strong>in</strong>g Truststo prioritise <strong>IT</strong> <strong>modernisation</strong> aga<strong>in</strong>st compet<strong>in</strong>g f<strong>in</strong>ancial pressures, for example,by <strong>in</strong>clusion <strong>in</strong> performance management frameworks. Whatever changes areplanned, <strong>the</strong>y need to be communicated throughout <strong>the</strong> <strong>NHS</strong> with clear timetablesto end <strong>the</strong> uncerta<strong>in</strong>ty and ‘plann<strong>in</strong>g blight’ that currently exists at local level.8.7. Implications for local implementation <strong>of</strong> <strong>IT</strong> applicationsOur study <strong>of</strong> NPf<strong>IT</strong> implementation at local level and end users’ views <strong>of</strong> specific<strong>IT</strong> <strong>in</strong>novations has implications at <strong>the</strong> local level <strong>in</strong> <strong>the</strong> <strong>NHS</strong>.The CPOE system with<strong>in</strong> Trust A and PACS with<strong>in</strong> Trust D were considered bymanagers and end-users to have been successful implementations <strong>of</strong> <strong>the</strong>se types<strong>of</strong> health care <strong>IT</strong> system, preced<strong>in</strong>g by several years <strong>the</strong> roll-out <strong>of</strong> similarsystems under NPf<strong>IT</strong>. The UK <strong>NHS</strong> is lead<strong>in</strong>g <strong>the</strong> way <strong>in</strong> terms <strong>of</strong> <strong>the</strong> scale andhomogeneity <strong>of</strong> its health care <strong>IT</strong> programme, and although runn<strong>in</strong>g beh<strong>in</strong>dschedule and over budget, <strong>the</strong> programme cont<strong>in</strong>ues to receive <strong>the</strong> support <strong>of</strong>managers and cl<strong>in</strong>icians alike. 86,87,115It is possible that CPOE and PACS, when fully <strong>in</strong>tegrated with <strong>the</strong> o<strong>the</strong>r <strong>IT</strong>systems which comprise NPf<strong>IT</strong> (national electronic health records, patientadm<strong>in</strong>istration systems, electronic book<strong>in</strong>g, etc), will contribute to more dramaticquantitative changes, which raises <strong>the</strong> issue <strong>of</strong> where <strong>the</strong> responsibility for localimplementation lies – at national or local level. In <strong>the</strong> meantime, <strong>the</strong> evidencebase to support <strong>the</strong> procurement and implementation <strong>of</strong> <strong>IT</strong> systems by health careproviders falls far short <strong>of</strong> <strong>the</strong> evidence base required to <strong>in</strong>form changes <strong>in</strong> cl<strong>in</strong>icalpractice with<strong>in</strong> <strong>the</strong>se same providers. This is perhaps unsurpris<strong>in</strong>g, given <strong>the</strong>129
Report to SDO for NCRS ProjectDiscussiondifferent set <strong>of</strong> stakeholders <strong>in</strong>volved, <strong>the</strong> top-down political pressure, <strong>the</strong> fiercecompetition among <strong>the</strong> companies which provide <strong>the</strong>se systems, and <strong>the</strong>widespread assumption <strong>in</strong> <strong>the</strong> technological doma<strong>in</strong> that newer is necessarilybetter.At <strong>the</strong> local level, Trusts should be aware <strong>of</strong> <strong>the</strong> factors which enhance or impede<strong>IT</strong> implementation, and would be advised to undertake an analysis <strong>of</strong> <strong>the</strong>sefactors <strong>in</strong> relation to <strong>the</strong>ir own local context, before undertak<strong>in</strong>g implementation,as follows:1. Attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novationThese factors <strong>in</strong>clude <strong>the</strong> ease <strong>of</strong> use and reliability <strong>of</strong> <strong>the</strong> <strong>in</strong>novation, and itscompatibility with exist<strong>in</strong>g practices or <strong>the</strong> ability to customise it such that it iscompatible.2. Characteristics <strong>of</strong> <strong>the</strong> ‘adopter’Regardless <strong>of</strong> <strong>the</strong> attributes <strong>of</strong> <strong>the</strong> <strong>in</strong>novation, <strong>the</strong>re will be variations <strong>in</strong> how <strong>the</strong><strong>in</strong>novation is received depend<strong>in</strong>g on <strong>the</strong> characteristics <strong>of</strong> <strong>the</strong> adopter e.g. howfamiliar <strong>the</strong>y are with <strong>IT</strong> etc. These should be taken <strong>in</strong>to account when plann<strong>in</strong>gimplementation. However, <strong>the</strong>se characteristics are not static and <strong>the</strong>re will be an<strong>in</strong>teraction between how <strong>the</strong> <strong>in</strong>novation is received, its attributes, and <strong>the</strong>implementation processes.3. Implementation processesUser consultation and <strong>in</strong>volvement are crucial factors <strong>in</strong> <strong>the</strong> implementationprocess. Where Trusts had consulted and <strong>in</strong>volved staff <strong>in</strong> <strong>the</strong> implementation,<strong>the</strong>y were more successful. The quality <strong>of</strong> tra<strong>in</strong><strong>in</strong>g for staff to use <strong>the</strong> <strong>in</strong>novation(s)and on-go<strong>in</strong>g <strong>IT</strong> support are also very important. F<strong>in</strong>ally, achiev<strong>in</strong>g a critical mass<strong>of</strong> implementation i.e. implement<strong>in</strong>g <strong>the</strong> <strong>IT</strong> application widely enough so that it isworthwhile for staff to use is important.4. Organisational factorsTrusts vary <strong>in</strong> <strong>the</strong>ir circumstances, which affect <strong>the</strong>ir ability to implement <strong>IT</strong><strong>in</strong>novations. Issues such as recent structural changes, e.g. mergers, and <strong>the</strong>impact <strong>of</strong> f<strong>in</strong>ancial deficits mean that for some Trusts it is much harder to prioritise<strong>IT</strong> implementation. These Trusts may require additional external support <strong>in</strong> order130
Report to SDO for NCRS ProjectDiscussionto achieve this implementation. As we identified with<strong>in</strong> our study <strong>of</strong> specific<strong>in</strong>novations, <strong>IT</strong> implementation requires a strong project management team withhigh level management support.The design and implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong>novations needs to be based on athorough understand<strong>in</strong>g <strong>of</strong> ‘<strong>the</strong> bus<strong>in</strong>ess’ that <strong>the</strong>y are be<strong>in</strong>g designed for.F<strong>in</strong>ally, <strong>the</strong> level <strong>of</strong> <strong>the</strong> ability <strong>of</strong> <strong>the</strong> organization to work as a whole and <strong>in</strong> teamsis an important factor <strong>in</strong> <strong>the</strong> implementation <strong>of</strong> <strong>IT</strong> <strong>in</strong>novations.8.8. ConclusionsThis study is one <strong>of</strong> <strong>the</strong> few carried out on <strong>the</strong> early stages <strong>of</strong> implementation <strong>of</strong><strong>the</strong> national <strong>IT</strong> programme for <strong>the</strong> <strong>NHS</strong> <strong>in</strong> England. It provides useful <strong>in</strong>sights <strong>in</strong>to<strong>the</strong> challenges <strong>of</strong> attempt<strong>in</strong>g this very ambitious programme, from <strong>the</strong> perspective<strong>of</strong> <strong>the</strong> local level. It also provides data on <strong>the</strong> processes and impact <strong>of</strong>implement<strong>in</strong>g specific <strong>IT</strong> applications on a scale not achieved before. The studyhas significant implications for <strong>the</strong> future direction <strong>of</strong> <strong>NHS</strong> <strong>IT</strong> policy. We have alsoraised important methodological issues for future studies <strong>of</strong> large scale <strong>IT</strong>implementation <strong>in</strong> health care.131
Report to SDO for NCRS ProjectReferences9. References1. <strong>NHS</strong> Executive. Information for health. An <strong>in</strong>formation strategy for <strong>the</strong> modern<strong>NHS</strong> 1998-2005. Leeds: <strong>NHS</strong> Executive, 1998.2. Information Policy Unit. Deliver<strong>in</strong>g 21st Century <strong>IT</strong> Support for <strong>the</strong> <strong>NHS</strong>.Department <strong>of</strong> Health, London, 12 June 2002. http://www.doh.gov.uk/ipu/.3. Hoeksma J. <strong>IT</strong> strategy lies <strong>in</strong> ru<strong>in</strong>s as only five trusts hit April EPR targets.Health Serv J 2002;5797:4-5.4. Wanless D. Secur<strong>in</strong>g our future health: tak<strong>in</strong>g a long-term view. F<strong>in</strong>al report.London: HMTreasurywww.hmtreasury.gov.uk./Consultations_and_Legislation/wanless/consult_wanless_f<strong>in</strong>al.cfm (accessed 12 Jul 2005) 2002.5. Department <strong>of</strong> Health. Deliver<strong>in</strong>g 21st century <strong>IT</strong> support for <strong>the</strong> <strong>NHS</strong>. Nationalstrategic programme. London: DoH, 2002.6. Dyke P. Healthy Connections? Public F<strong>in</strong>ance 2003:24-6.7. Herbert M. Pr<strong>of</strong>essional and organizational impact <strong>of</strong> us<strong>in</strong>g patient care<strong>in</strong>formation systems. Med<strong>in</strong>fo 1998;9:849-53.8. Herbst K, Littlejohns P, Rawl<strong>in</strong>son J, Coll<strong>in</strong>son M, Wyatt JC. Evaluat<strong>in</strong>gcomputerized health <strong>in</strong>formation systems: hardware, s<strong>of</strong>tware and humanware: experiences from <strong>the</strong> Nor<strong>the</strong>rn Prov<strong>in</strong>ce, South Africa. J Public HealthMed 1999;21:305-10.9. Southon F, Sauer C, Dampney CNG. Information technology <strong>in</strong> complexhealth services: Organizational impediments to successful technology transferand diffusion. J Am Med Inform Assoc 1997;4:112-24.10. Booth N. Shar<strong>in</strong>g patient <strong>in</strong>formation electronically throughout <strong>the</strong> <strong>NHS</strong>. BMJ2003;327:114-5.11. Heathfield H, Pitty D, Hanka, R. Evaluat<strong>in</strong>g <strong>in</strong>formation technology <strong>in</strong> healthcare: barriers and challenges. BMJ 1998;316:1959-61.12. Southon G, Sauer C, Dampney K. Lessons from a failed <strong>in</strong>formation systems<strong>in</strong>itiative: Issues for complex organisations. Int J Med Inform 1999;55:33-46.13. Lorenzi NM, Riley RT, Blyth AJC, Southon G, Dixon BJ. Antecendents <strong>of</strong> <strong>the</strong>people and organizational aspects <strong>of</strong> medical <strong>in</strong>formatics: Review <strong>of</strong> <strong>the</strong>literature. J Am Med Inform Assoc 1997;4:79-93.132
Report to SDO for NCRS ProjectReferences14. The British Journal <strong>of</strong> Healthcare Comput<strong>in</strong>g and Management. Mckesson HISdelayed aga<strong>in</strong> at ERI. Editorial. The British Journal <strong>of</strong> Healthcare Comput<strong>in</strong>gand Management 2004;21:13.15. Lock C. What value do comoputers provide to <strong>NHS</strong> hospitals? BMJ1996;312:1407-10.16. Heathfield HA, Buchan IE. Current evaluations <strong>of</strong> <strong>in</strong>formation technology <strong>in</strong>health care are <strong>of</strong>ten <strong>in</strong>adequate. BMJ 1996;313:1008.17. Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC,Shekelle PG. Systematic review: impact <strong>of</strong> health <strong>in</strong>formation technology onquality, efficiency, and costs <strong>of</strong> medical care. Ann Intern Med 2006;144:742-52.18. Georgiou A, Williamson M, Westbrook JI, Ray S. The impact <strong>of</strong> computerisedphysician order entry systems on pathology services: A systematic review. IntJ Med Inform 2006.19. Wyatt JC, Wyatt SM. When and how to evaluate health <strong>in</strong>formation systems?International Journal <strong>of</strong> Medical Informatics 2003;69:251-259.20. Wyatt JC. Four barriers to realis<strong>in</strong>g <strong>the</strong> <strong>in</strong>formation revolution <strong>in</strong> health care.In: Lenaghan J, editor. Reth<strong>in</strong><strong>in</strong>g <strong>IT</strong> & Health. London: Institute for PublicPolicy Research, 1998:100-122.21. Laerum H, Ell<strong>in</strong>gsen G, Faxaag A. Doctors' use <strong>of</strong> electronic medical recordssystems <strong>in</strong> hospitals: cross sectional survey. BMJ 2001;323:1344-8.22. Benson T. Why general practitioners use computers and hospital doctors donot - Part 1: <strong>in</strong>centives. BMJ 2002;325:1086-9.23. Berg M. The search for synergy: Interrelat<strong>in</strong>g medical work and patient care<strong>in</strong>formation systems. Methods <strong>of</strong> Information <strong>in</strong> Medic<strong>in</strong>e 2003;42:337-44.24. Moorman PW, van der Lei J. An <strong>in</strong>ventory <strong>of</strong> publications on electronic patientrecords. Methods Inf Med 1999;38.25. Darbyshire P. The practice politics <strong>of</strong> computerised <strong>in</strong>formation systems: Afocus group study. Nurse Res 2001;8:4-17.26. Timmons S. Resistance to computerized care plann<strong>in</strong>g systems by qualifiednurses work<strong>in</strong>g <strong>in</strong> <strong>the</strong> UK <strong>NHS</strong>. Methods Inf Med 2003;42:471-6.27. Coiera E, Tombs V. Communication behaviours <strong>in</strong> a hospital sett<strong>in</strong>g: anobservational study. BMJ 1998;316:673-6.133
Report to SDO for NCRS ProjectReferences28. Harper RH, O'Hara KP, Sellen AJ, Duthie DJ. Toward <strong>the</strong> paperless hospital?Br J Anaesth 1997;78:762-7.29. Handy J, Hunter I, Whiddett R. User acceptance <strong>of</strong> <strong>in</strong>ter-organizationalelectronic medical records. Health Informatics J 2001;7:103-107.30. Backer TE. Manag<strong>in</strong>g <strong>the</strong> human side <strong>of</strong> change <strong>in</strong> VA's transformation. HospHealth Serv Adm 1997;42:433-59.31. Brown SH, L<strong>in</strong>coln MJ, Groen PJ, Kolodner RM. VistA - U. S. Department <strong>of</strong>Veterans Affairs national-scale HIS. Int J Med Inform 2003;69:135-56.32. Ash J, Gorman PN, Hersh WR, Lavelle M, Poulsen SB. Perceptions <strong>of</strong> house<strong>of</strong>ficers who use Physician Order Entry. American Medical InformationAssocation 1999:471-5.33. Ash JS, Lyman J, Carpenter J, Fournier L. A diffusion <strong>of</strong> <strong>in</strong>novations model <strong>of</strong>Physician Order Entry. American Medical Information Assocation 2001:22-6.34. Dykstra R. Computerized physician order entry and communication:Reciprocal impacts. American Medical Information Assocation - AnnualSymposium Proceed<strong>in</strong>g 2002:230-4.35. Ash JS, Gorman PN, Lavelle M, Payne TH, Massaro TA, Frantz GL. et al. Across-site qualitative study <strong>of</strong> Physician Order Entry. Journal <strong>of</strong> <strong>the</strong> AmericanMedical Informatics Association 2003;10:188-200.36. Mekhjian HS, Kumar RR, Kuehn L, Bentley TD, Teater P, Thomas A, et al.Immediate benefits realized follow<strong>in</strong>g implementation <strong>of</strong> physician order entryat an academic medical center. J Am Med Inform Assoc 2002;9:529-39.37. Herbst K, Littlejohns P, Rawl<strong>in</strong>son J, Coll<strong>in</strong>son M, Wyatt JC. Evaluat<strong>in</strong>gcomputerized health <strong>in</strong>formation systems: hardware, s<strong>of</strong>tware and humanware: experiences from <strong>the</strong> Nor<strong>the</strong>rn Prov<strong>in</strong>ce, South Africa. J Public HealthMed 1999;21:305-10.38. Bowns IR, Ro<strong>the</strong>rham G, Paisley S. Factors associated with success <strong>in</strong> <strong>the</strong>implementation <strong>of</strong> <strong>in</strong>formation management and technology <strong>in</strong> <strong>the</strong> <strong>NHS</strong>.Health Informatics J 1999;5:136 -45.39. <strong>NHS</strong> Information Authority. Core national evaluation <strong>of</strong> <strong>the</strong> electronic recordsdevelpment and implementation sites. 2003 January 31st F<strong>in</strong>al report (N2/P4).40. Kle<strong>in</strong> L. Realism, realism, realism. The British Journal <strong>of</strong> HealthcareComput<strong>in</strong>g and Management 1999;16:16-8.134
Report to SDO for NCRS ProjectReferences41. Kle<strong>in</strong> L. Research evaluation <strong>of</strong> <strong>NHS</strong> EPR/ICWS pilot sites. Produced byManchester Centre for Healthcare Management, University <strong>of</strong> Manchester;The Bayswater Institute, London: Medical Informatics Group, University <strong>of</strong>Manchester; School <strong>of</strong> Postgraduate Studies <strong>in</strong> Medical and Health Care,Swansea. 2001.42. Jones AJ, Hart A, Henwood F, Gerhardt C. The use <strong>of</strong> electronic patientrecords (EPRs) <strong>in</strong> <strong>the</strong> maternity services: Pr<strong>of</strong>essional and publicacceptability: University <strong>of</strong> Brighton, 2003:1-14.43. Bend J. Public Value and e-Health. London: Institute for Public PolicyResearch, 2004.44. National Audit Office. Department <strong>of</strong> Health: <strong>the</strong> National Programme for <strong>IT</strong> <strong>in</strong><strong>the</strong> <strong>NHS</strong>. London: Stationery Office, 2006.45. Berg M. Implement<strong>in</strong>g <strong>in</strong>formation systems <strong>in</strong> health care organizations: mythsand challenges. Int J Med Inform 2001;64:143-56.46. Drummond MF, Sculpher M, Torrance G, O'Brien B, Stoddart GL. Methods for<strong>the</strong> economic evaluation <strong>of</strong> health care programmes. Oxford: OxfordUniversity Press, England, 2005.47. Shiell A, Donaldson C, Mitton C, Currie G. Health economic evaluation. JEpidemiol. Community Health 2002;56:85-88.48. Clapm S, Keen J. The Value <strong>of</strong> Electronic Health Records: A Literature review:Yorkshire Centre for Health Informatics, University <strong>of</strong> Leeds, 2005.49. Alanen J, Keski Nisula L, Laurila J, Suramo I, Standertskjold Nordenstam CG,Brommels M. Costs <strong>of</strong> pla<strong>in</strong>-film radiography <strong>in</strong> a partially digitized radiologydepartment:an activity-based cost analysis. Acta Radiologica 1998;39:200-7.50. Chan L, Trambert M, Kywi A, Hartzman S. PACS <strong>in</strong> private practice--effect onpr<strong>of</strong>its and productivity. J Digit Imag<strong>in</strong>g 2002;15 Suppl 1:131-6.51. Kaushal R, Jha AK, Franz C, Glaser J, Shetty KD, Jaggi T, et al. Return on<strong>in</strong>vestment for a computerized physician order entry system. J Am Med InformAssoc 2006;13:261-6.52. Taylor R, Manzo J, S<strong>in</strong>nett M. Quantify<strong>in</strong>g value for physician order-entrysystems: a balance <strong>of</strong> cost and quality. Healthc F<strong>in</strong>anc Manage 2002;56:44-8.135
Report to SDO for NCRS ProjectReferences53. Arias-Vimarlund V, Ljunggren M, Timpka T,. Implementation <strong>of</strong> computerbasedpatient records <strong>in</strong> primary care: <strong>the</strong> societal health economic effects.Proc AMIA Annu Fall Symp 1996:503-7.54. The Efficiency Map. Department <strong>of</strong> Health 2005 Available from: URL:http://www.dh.gov.uk/assetRoot/04/11/75/50/04117550.pdf (cited 2007 March14).55. Fleiss J. Statistical methods for rates and proportions,. New York Wiley, 1981.56. Bryan S, Wea<strong>the</strong>rburn G, Buxton M, Watk<strong>in</strong>s J, Keen J, Muris N. <strong>Evaluation</strong> <strong>of</strong>a hospital picture archiv<strong>in</strong>g and communication system. J Health Serv ResPolicy 1999;4:204-9.57. Bryan S, Buxton M, Brenna E. Estimat<strong>in</strong>g <strong>the</strong> impact <strong>of</strong> a diffuse technologyon <strong>the</strong> runn<strong>in</strong>g costs <strong>of</strong> a hospital: a case study <strong>of</strong> a picture archiv<strong>in</strong>g andcommunication system. Int J Technol Assess Health Care 2000;16:787-98.58. Siegel EL. Economic and cl<strong>in</strong>ical impact <strong>of</strong> filmless operation <strong>in</strong> a multifacilityenvironment. J Digit Imag<strong>in</strong>g 1998;11:42-7.59. Siegel E, Re<strong>in</strong>er BI. The costs and benefits <strong>of</strong> pacs <strong>in</strong> <strong>the</strong> va: past experience,present reality, and future potential. Appl Radiol 1998;27:15-8.60. Siegel EL, Re<strong>in</strong>er BI. Filmless radiology at <strong>the</strong> Baltimore VA Medical Center: a9 year retrospective. Comput Med Imag<strong>in</strong>g Graph 2003;27:101-9.61. Barlow S, Johnson J, Steck J. The economic effect <strong>of</strong> implement<strong>in</strong>g an EMR<strong>in</strong> an outpatient cl<strong>in</strong>ical sett<strong>in</strong>g. J Healthc Inf Manag 2004;18:46-51.62. Miller RH, West C, Brown TM, Sim I, Ganch<strong>of</strong>f C. The value <strong>of</strong> electronichealth records <strong>in</strong> solo or small group practices. Physicians' EHR adoption isslowed by a reimbursement system that rewards <strong>the</strong> volume <strong>of</strong> services morethan it does <strong>the</strong>ir quality. Health Aff (Millwood) 2005;24:1127-37.63. Overhage JM, Dexter PR, Perk<strong>in</strong>s SM, Cordell WH, McG<strong>of</strong>f J, McGrath R, etal. A randomized, controlled trial <strong>of</strong> cl<strong>in</strong>ical <strong>in</strong>formation shared from ano<strong>the</strong>r<strong>in</strong>stitution. Ann Emerg Med 2002;39:14-23.64. Sachs R. The economic justification for electronic medical record systems. In:Davidson P, editor. Healthcare Information Systems. Boca Raton, FL:Auerbach publ, 2000:259-73.136
Report to SDO for NCRS ProjectReferences65. Wagner S, Morrison WB, Carr<strong>in</strong>o JA, Schweitzer ME, Nothnagel H. Picturearchiv<strong>in</strong>g and communication system: effect on report<strong>in</strong>g <strong>of</strong> <strong>in</strong>cidental f<strong>in</strong>d<strong>in</strong>gsRadiology 2002;225:500-5.66. Wang SJ, Middleton B, Prosser LA, Bardon CG, Spurr CD, Carchidi PJ, et al.A cost-benefit analysis <strong>of</strong> electronic medical records <strong>in</strong> primary care. Am JMed 2003;114:397-403.67. Maass M, Kosonen M, Kormano M. Cost analysis <strong>of</strong> Turku University CentralHospital PACS <strong>in</strong> 1998. Comput Methods Programs Biomed 2001;66:41-5.68. Fulop N, Protopsaltis G, Hutch<strong>in</strong>gs A, K<strong>in</strong>g A, Allen P, Normand C, et al.Process and impact <strong>of</strong> mergers <strong>of</strong> <strong>NHS</strong> trusts: multicentre case study andmanagement cost analysis. BMJ 2002;325:246-52.69. Hillestad R, Bigelow J, Bower A, Girosi F, Meili R, Scoville R, et al. Canelectronic medical record systems transform health care? Potential healthbenefits, sav<strong>in</strong>gs, and costs. The adoption <strong>of</strong> <strong>in</strong>teroperable EMR systemscould produce efficiency and safety sav<strong>in</strong>gs <strong>of</strong> $142-$371 billion. Health Aff(Millwood) 2005;24:1103-17.70. Pettigrew A. The Awaken<strong>in</strong>g Giant. Oxford: Basil Blackwell, 1985.71. Pettigrew A. The management <strong>of</strong> strategic change. Oxford: Blackwell, 1987.72. Ferlie E. Organisational studies. In: Fulop N, Allen P, Clarke A, Black N (eds).Study<strong>in</strong>g <strong>the</strong> organisation and delivery <strong>of</strong> health services London: Routledge,2001.73. Langley A. Strategies for <strong>the</strong>oriz<strong>in</strong>g from process data Acad Manage Rev1999;24:691-710.74. Berg MA, Aarts J, van der Lei J. ICT <strong>in</strong> Health Care: SociotechnicalApproaches. Methods Inf Med 2003;42:297-301.75. Fulop N, Allen P, Clarke A, Black N, editors. Study<strong>in</strong>g <strong>the</strong> organisation anddelivery <strong>of</strong> health services. London: Routledge, 2001.76. McKersie RB, Walton RE. Organizational change. In: Allen TJ, Scott MortonMS (Eds) Information Technology and <strong>the</strong> Corporation <strong>of</strong> <strong>the</strong> 1990s: ResearchStudies, New York: Oxford University Press, 1991.77. Pettigrew A, Ferlie E, McKee L Shap<strong>in</strong>g Strategic Change. London: Sagepublications, 1992.78. Rogers EM. Diffusion <strong>of</strong> Innovations. New York: Free Press, 2003.137
Report to SDO for NCRS ProjectReferences79. Greenhalgh T, Robert G, MacFarlane, F Bate, P Kyriakidou, O Diffusion <strong>of</strong><strong>in</strong>novations <strong>in</strong> service organisations: systematic review and recommendationsMilbank Quarterly 2004;82:581-629.80. Miles M. Qualitative data as an attractive nuisance—<strong>the</strong> problem <strong>of</strong> analysis.Adm Sci Q 1979;24:590-601.81. Henwood K, Pigeon N. Grounded <strong>the</strong>ory and research. The Psychologist1995;8:115-8.82. Glaser B, Strauss A. The discovery <strong>of</strong> grounded <strong>the</strong>ory: strategies forqualitative research. New York: Ald<strong>in</strong>e de Gruyter, 1967.83. Shadish W, Cook TD, Campbell DT. Experimental and Quasi-ExperimentalDesigns for Generalized Causal Inference. Boston: Houghton Miffl<strong>in</strong>, 2002.84. Chang B, Pocock, S. Analyz<strong>in</strong>g data with clump<strong>in</strong>g at zero. An exampledemonstration. J Cl<strong>in</strong> Epidemiol 2000;53:1036-43.85. Tierney W, Miller ME, McDonald CJ The effect on test order<strong>in</strong>g <strong>of</strong> <strong>in</strong>form<strong>in</strong>gphysicians <strong>of</strong> <strong>the</strong> charges for outpatient diagnostic tests. N Engl J Med1990;322:1499-504.86. Hendy J, Reeves BC, Fulop N, Hutch<strong>in</strong>gs A, Masseria C. Challenges to <strong>the</strong>national programme for <strong>in</strong>formation technology (NPf<strong>IT</strong>): a qualitative studyBMJ 2005;331:331-4.87. Hendy J, Fulop N, Reeves BC, Hutch<strong>in</strong>gs A, Coll<strong>in</strong> SM, . Implement<strong>in</strong>g <strong>the</strong><strong>NHS</strong> <strong>IT</strong> programme: a qualitative study <strong>of</strong> progress <strong>in</strong> acute trusts. In Press2007.88. Parliamentary Office <strong>of</strong> Science and Technology. New <strong>NHS</strong> <strong>IT</strong>. Post note No214. www.parliament.uk/post (accessed 2 Mar 2004) 2004.89. Cross M. Keep<strong>in</strong>g <strong>the</strong> <strong>NHS</strong> electronic sp<strong>in</strong>e on track. BMJ 2006;332:656-8.90. Connect<strong>in</strong>g for Heath: brakes placed on electronic care record as concernsgrow. Health Service Journal 2006 May 4th91. Redfern RO, Horii SC, Fe<strong>in</strong>gold E, Kundel HL. Radiology workflow and patientvolume: effect <strong>of</strong> picture archiv<strong>in</strong>g and communication systems ontechnologists and radiologists. J Digit Imag<strong>in</strong>g 2000;13:97-100.92. Redfern RO, Langlotz CP, Abbuhl SB, Polansky M, Horii SC, Kundel HL. Theeffect <strong>of</strong> PACS on <strong>the</strong> time required for technologists to produce radiographic138
Report to SDO for NCRS ProjectReferencesimages <strong>in</strong> <strong>the</strong> emergency department radiology suite. J Digit Imag<strong>in</strong>g2002;15:153-60.93. Commission for Health Improvement. Performance rat<strong>in</strong>gs: overall summary <strong>of</strong>results 2002-3. www.chi.nhs.uk/Rat<strong>in</strong>gs (accessed 27 Feb 2004).94. Comptroller and Auditor General. <strong>NHS</strong> (England) Summarised Accounts2002-2003 London: Stationery Office, 2004.95. e-health-<strong>in</strong>sider. Issue no. 232. . CfH aims to <strong>in</strong>stall at 22 acute trusts byOctober. http://www.e-health-<strong>in</strong>sider.com/news/newsletter.cfm (accessed 10July 2006) 2006 July.96. Outpatient Data Quality Report 2003-03 and 2004-05 The Information Centre2006 December 15 Available from: URL:http://www.ic.nhs.uk/pubs/outpatientdq/report/file.97. Bates DW, Boyle DL, Rittenberg E, Kuperman GJ, Ma'luf N, Menk<strong>in</strong> Vea.What proportion <strong>of</strong> common diagnostic tests appear redundant? Am J Med1998;104:361-8.98. Bates DW, Kuperman GJ, Rittenberg E, Teich JM, Fiskio J, Ma'luf Nea. Arandomized trial <strong>of</strong> a computer-based <strong>in</strong>tervention to reduce utilization <strong>of</strong>redundant laboratory tests. Am J Med 1999;106:144-50.99. Weydert J, Nobbs ND, Feld R, Kemp JD A simple, focused, computerizedquery to detect overutilization <strong>of</strong> laboratory tests Arch Pathol Lab Med2005;129:1141-3.100. Gosl<strong>in</strong>g P. Here comes <strong>the</strong> enforcer. Public F<strong>in</strong>ance 2004;22.101. Jones A, Hart A, Henwood F, Gerhardt C. The use <strong>of</strong> electronic patientrecords (EPRs) <strong>in</strong> <strong>the</strong> maternity services: pr<strong>of</strong>essional and public acceptability.Brighton: University <strong>of</strong> Brighton 2003:1-14.102. National Audit Office. Department <strong>of</strong> Health: patient choice at <strong>the</strong> po<strong>in</strong>t <strong>of</strong> GPreferral. London: Stationery Office, 2005.103. National Programme for Information Technology. <strong>NHS</strong> care record service:<strong>in</strong>dicative deployment plan—Jan 2005.www.connect<strong>in</strong>gforhealth.nhs.uk/all_images_and_docs/imp_plan_0105.pdf(accessed 12 Jul 2005) 2005.104. Benson T. Why general practitioners use computers and hospital doctors donot - Part 2: scalability. BMJ 2002;325:1090-3.139
Report to SDO for NCRS ProjectReferences105. Keen J. The <strong>NHS</strong> programme for <strong>in</strong>formation technology. This massive naturalexperiment needs evaluat<strong>in</strong>g and regulat<strong>in</strong>g. 333 2006:3-4.106. Jones M. Learn<strong>in</strong>g <strong>the</strong> lessons <strong>of</strong> history? Electronic records <strong>in</strong> <strong>the</strong> UnitedK<strong>in</strong>gdom acute hospitals, 1988-2002. Health Inform J 2004;10:253-63.107. BBC news. GPs dissatisfied with <strong>IT</strong> system.http://news.bbc.co.uk/1/hi/health/5028762.stm (accessed 21 June 2006).108. Tierney W, McDonald CJ, Mart<strong>in</strong> DK, Rogers MP. Computerized display <strong>of</strong>past test results. Effect on outpatient test<strong>in</strong>g. Ann Intern Med 1987;104:569-74.109. Westbrook J, Georgiou A, Dimos A, Germanos T. Computerised pathologytest order entry reduces laboratory turnaround times and <strong>in</strong>fluences testsordered by hospital cl<strong>in</strong>icians: a controlled before and after study. J Cl<strong>in</strong> Pathol2006;59:533-6.110. Wang T, Mort EA, Nordberg P, Chang Y, Cadigan ME, Mylott L, et al Autilization management <strong>in</strong>tervention to reduce unnecessary test<strong>in</strong>g <strong>in</strong> <strong>the</strong>coronary care unit. Arch Intern Med 2002;162:1885-90.111. Re<strong>in</strong>er B, Siegel E, Flagle C, Hooper F, Cox R, Scanlon M. Effect <strong>of</strong> filmlessimag<strong>in</strong>g on <strong>the</strong> utilization <strong>of</strong> radiologic services. Radiology 2000;215:163-7.112. Crowe B, Sim L. Implementation <strong>of</strong> a radiology <strong>in</strong>formation system/picturearchiv<strong>in</strong>g and communication system and an image transfer system at a largepublic teach<strong>in</strong>g hospital--assessment <strong>of</strong> success <strong>of</strong> adoption by cl<strong>in</strong>icians. JTelemed Telecare 2004;10 Suppl 1:25-7.113. Watk<strong>in</strong>s J, Bryan S, Muris NM, Buxton MJ. Exam<strong>in</strong><strong>in</strong>g <strong>the</strong> <strong>in</strong>fluence <strong>of</strong> picturearchiv<strong>in</strong>g communication systems and o<strong>the</strong>r factors upon <strong>the</strong> length <strong>of</strong> stay forpatients with total hip and total knee replacements Int J Technol AssessHealth Care 1999;15:497-505.114. British Computer Society. The Way Forward for <strong>NHS</strong> Health Informatics.Where should <strong>NHS</strong> Connect<strong>in</strong>g for Health (<strong>NHS</strong> CFH) go from here? London:British Computer Society 2006.115. Department <strong>of</strong> Health. The <strong>NHS</strong> <strong>in</strong> England: operat<strong>in</strong>g framework for 2007/08.London: Department <strong>of</strong> Health, 2006.116. Iglehart J. Pursu<strong>in</strong>g health <strong>IT</strong>: <strong>the</strong> delicate dance <strong>of</strong> government and <strong>the</strong>market. Health Aff 2005;24:1100-1.140
Report to SDO for NCRS ProjectReferences117. Coll<strong>in</strong>s T. British Computer Society report. .http://www.computerweekly.com/Articles/2006/08/29/218056/central-nhs-itmay-not-work-warns-bcs.htm(accessed 30 January 2007)118. Department <strong>of</strong> Health. The <strong>NHS</strong> <strong>in</strong> England: <strong>the</strong> operat<strong>in</strong>g framework for2007/08 http://www.dh.gov.uk/assetRoot/04/14/11/95/04141195.pdf (accessed30 January 2007).141
AppendicesAppendix 1EPR Implementation Project - Interview ScheduleLevel 1, stage a. - Organisational ContextDate and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Question -What contextual factors (historically and currently) act as facilitators or barriers to <strong>the</strong>implementation <strong>of</strong> EPRs at acute trusts – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong> impact <strong>of</strong> recent<strong>NHS</strong>CRS policy changes on EPR implementation.Preamble -Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to capture managers’ experiences <strong>of</strong> EPRs,particularly factors that facilitate or h<strong>in</strong>der successful implementation. The <strong>in</strong>terviewwill last no more than one hour and with your permission will be tape recorded – justto help me remember what was said later on. To reassure you, all <strong>in</strong>formationobta<strong>in</strong>ed will be anonymised. Nei<strong>the</strong>r <strong>the</strong> trust nor <strong>in</strong>dividual staff will be identified,when <strong>the</strong> research is written up, with all names and staff positions anonymised. Youwill have an opportunity to read <strong>the</strong> draft f<strong>in</strong>al report to make factual corrections. Youwill also receive an executive summary and be able to attend a sem<strong>in</strong>ardissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Before we beg<strong>in</strong>, do you have any questions, anyth<strong>in</strong>g I have not covered?2
AppendicesOK. Firstly, I’d like to ask you some general questions about <strong>the</strong> National Programmefor <strong>IT</strong>, <strong>the</strong>n I’d like to ask you about EPR implementation at (<strong>the</strong> trust).NPf<strong>IT</strong> <strong>in</strong> general -1. Previously, reach<strong>in</strong>g national targets regard<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> EPRs wasprimarily <strong>the</strong> responsibility <strong>of</strong> local trusts. The National Program for InformationTechnology (NPf<strong>IT</strong>) has now decided a more centrally controlled approach isneeded. What do you th<strong>in</strong>k about this decision?Prompts: explore wider organisational factors specific to <strong>the</strong> <strong>NHS</strong> that haveh<strong>in</strong>dered <strong>IT</strong> implementation?What would have helped?Will centrally controlled solutions be better or worse?EPR development at <strong>the</strong> trust -2. In 1998, Information for Health set out six levels <strong>of</strong> EPR development. By April2002 it was reported that only 3% <strong>of</strong> trusts (five <strong>in</strong> total) had complete EPRsystems <strong>in</strong> place – way under <strong>the</strong> hoped for target. In try<strong>in</strong>g to achieve some level<strong>of</strong> EPR implementation - can you give me any <strong>in</strong>sights <strong>in</strong>to how (<strong>the</strong> trust) got on?Prompts: explore <strong>the</strong> trust’s past experiences <strong>of</strong> implementation.Previous <strong>in</strong>-house <strong>IT</strong> successes and failuresAny specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. What do you th<strong>in</strong>k were some <strong>of</strong> <strong>the</strong> barriers to implementation, and what could<strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong> EPRdevelopment?Prompts: explore physical, <strong>in</strong>formational and organisational resources (costs)that have facilitated or h<strong>in</strong>dered <strong>IT</strong> implementation.3
AppendicesExplore <strong>the</strong> relationship between Trust Managers and <strong>the</strong> <strong>in</strong>formation system <strong>in</strong>use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.4. In terms <strong>of</strong> prepar<strong>in</strong>g for <strong>the</strong> new LSP solutions what do you th<strong>in</strong>k needs to bedone at (trust)?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong> LSPsolutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore any structuralchanges and strategy documents (obta<strong>in</strong> if available).5. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.6. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).7. Across <strong>the</strong> trust, how much agreement do you th<strong>in</strong>k <strong>the</strong>re is about <strong>the</strong> importance<strong>of</strong> achiev<strong>in</strong>g NCRS?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.8. In implement<strong>in</strong>g <strong>the</strong> LSP solutions – where do you see potential areas <strong>of</strong> difficulty?4
AppendicesPrompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities.Differ<strong>in</strong>g agendas – how <strong>the</strong> EPR implementation programme needs to address<strong>the</strong> priorities <strong>of</strong> ‘everyman’ - trust, SHA, and National Program.Explore <strong>the</strong> role <strong>of</strong> <strong>in</strong>-house <strong>IT</strong> <strong>in</strong>novations and <strong>the</strong>ir future.Explore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?9. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> goals – electronic patientrecords that support an <strong>in</strong>tegrated care records service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.10. For you what constitutes EPR implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?11. How can this success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time –12. Regard<strong>in</strong>g NPf<strong>IT</strong> - what do you th<strong>in</strong>k will be happen<strong>in</strong>g <strong>in</strong> <strong>the</strong> future?Prompts: explore whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k NPf<strong>IT</strong> will deliver long term – and <strong>the</strong>consequences <strong>of</strong> (non) delivery.5
Appendices13. How do you th<strong>in</strong>k (trust) will respond to <strong>the</strong>se changes?Prompts: explore both positive and negative responses.14. Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 2EPR Implementation Project - Interview ScheduleLevel 1, stage b. - Organisational ContextDate and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Question -What contextual factors (historically and currently) act as facilitators or barriers to <strong>the</strong>implementation <strong>of</strong> EPRs at acute trusts – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong> impact <strong>of</strong> recent<strong>NHS</strong>CRS policy changes on EPR implementation.Preamble -Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to follow up on <strong>in</strong>formation ga<strong>the</strong>red about <strong>the</strong>(NPf<strong>IT</strong>) <strong>in</strong> 2004. The aim to ga<strong>the</strong>r fur<strong>the</strong>r <strong>in</strong>formation about pr<strong>of</strong>essionals’ andmanagers’ experiences and <strong>the</strong>ir views on <strong>the</strong> NPf<strong>IT</strong>, particularly factors thatfacilitate or h<strong>in</strong>der successful implementation. The <strong>in</strong>terview will last no more thanone hour and with your permission will be tape recorded – just to help me rememberwhat was said later on. To reassure you, all <strong>in</strong>formation obta<strong>in</strong>ed will be anonymised.Nei<strong>the</strong>r <strong>the</strong> trust nor <strong>in</strong>dividual staff will be identified, when <strong>the</strong> research is written up,with all names and staff positions anonymised. You will have an opportunity to read<strong>the</strong> draft f<strong>in</strong>al report to make factual corrections. You will also receive an executivesummary and be able to attend a sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Before we beg<strong>in</strong>, do you have any questions, anyth<strong>in</strong>g I have not covered?2
AppendicesOK. Firstly, I’d like to ask you some general questions about <strong>the</strong> National Programmefor <strong>IT</strong>, <strong>the</strong>n I’d like to ask you about EPR implementation at (<strong>the</strong> trust).NPf<strong>IT</strong> <strong>in</strong> general -1. Previously, reach<strong>in</strong>g national targets regard<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> EPRs wasprimarily <strong>the</strong> responsibility <strong>of</strong> local trusts. The National Program for InformationTechnology (NPf<strong>IT</strong>) has now decided a more centrally controlled approach isneeded. What do you th<strong>in</strong>k about this decision?Prompts: explore wider organisational factors specific to <strong>the</strong> <strong>NHS</strong> that haveh<strong>in</strong>dered <strong>IT</strong> implementation?What would have helped?Will centrally controlled solutions be better or worse?EPR development at <strong>the</strong> trust -2. In try<strong>in</strong>g to achieve some level <strong>of</strong> EPR implementation - can you give me any<strong>in</strong>sights <strong>in</strong>to how (<strong>the</strong> trust) has been gett<strong>in</strong>g on?Prompts: explore <strong>the</strong> trust’s past experiences <strong>of</strong> implementation.Previous <strong>in</strong>-house <strong>IT</strong> successes and failuresMore recent deal<strong>in</strong>gs with NPf<strong>IT</strong>Any specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. What do you th<strong>in</strong>k were some <strong>of</strong> <strong>the</strong> barriers to implementation, and what could<strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong> EPRdevelopment? What could central NPf<strong>IT</strong> have done differently?Prompts: explore physical, <strong>in</strong>formational and organisational resources (costs)that have facilitated or h<strong>in</strong>dered <strong>IT</strong> implementation.3
AppendicesExplore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong> central and LSPcontractors.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.4. In terms <strong>of</strong> prepar<strong>in</strong>g for <strong>the</strong> new LSP solutions what do you th<strong>in</strong>k needs to bedone at (trust)?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong> LSPsolutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore any structuralchanges and strategy documents (obta<strong>in</strong> if available).5. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.Explore <strong>the</strong> role <strong>of</strong> LSPs <strong>in</strong> driv<strong>in</strong>g th<strong>in</strong>gs forward6. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).7. Across <strong>the</strong> trust, how much agreement do you th<strong>in</strong>k <strong>the</strong>re is about <strong>the</strong> importance<strong>of</strong> achiev<strong>in</strong>g NCRS?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.8. In implement<strong>in</strong>g <strong>the</strong> LSP solutions – where do you see potential areas <strong>of</strong> difficulty?4
AppendicesPrompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities.Differ<strong>in</strong>g agendas – how <strong>the</strong> EPR implementation programme needs to address<strong>the</strong> priorities <strong>of</strong> ‘everyman’ - trust, SHA, and National Program.Explore <strong>the</strong> role <strong>of</strong> <strong>in</strong>-house <strong>IT</strong> <strong>in</strong>novations and <strong>the</strong>ir future.Explore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?9. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g <strong>the</strong> NPf<strong>IT</strong> goals – electronic patientrecords that support an <strong>in</strong>tegrated care records service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.10. For you what constitutes EPR implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?11. How can this success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time –12. Regard<strong>in</strong>g NPf<strong>IT</strong> - what do you th<strong>in</strong>k will be happen<strong>in</strong>g <strong>in</strong> <strong>the</strong> future?Prompts: explore whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k NPf<strong>IT</strong> will deliver long term – and <strong>the</strong>consequences <strong>of</strong> (non) delivery.5
Appendices13. How do you th<strong>in</strong>k (trust) will respond to <strong>the</strong>se changes?Prompts: explore both positive and negative responses.14. Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 3EPR Implementation Project - Interview ScheduleLevel 2 – EPR useDate and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Department/ speciality:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Use <strong>of</strong> EPR <strong>in</strong> post:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Questions -How are specific areas <strong>of</strong> EPR functionality experienced by end-users?How is <strong>the</strong> process <strong>of</strong> implementation?Does EPR use impact on current work<strong>in</strong>g practices? And if so how?Preamble –Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to explore your experiences <strong>of</strong> us<strong>in</strong>g <strong>in</strong>formationtechnology (EPRs) <strong>in</strong> do<strong>in</strong>g your job. The <strong>in</strong>terview will last no more than one hourand with your permission will be tape recorded – just to help me remember what wassaid later on. To reassure you, all <strong>in</strong>formation obta<strong>in</strong>ed will be anonymised. Nei<strong>the</strong>r<strong>the</strong> trust nor <strong>in</strong>dividual staff will be identified, when <strong>the</strong> research is written up, with allnames and staff positions anonymised. You will have an opportunity to read <strong>the</strong> draftf<strong>in</strong>al report to make factual corrections. You will also receive an executive summaryand be able to attend a sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Before we beg<strong>in</strong>, do you have any questions, anyth<strong>in</strong>g I have not covered?OK. Firstly, I’d like to ask you some general questions about what’s its like to use <strong>the</strong>current system, <strong>the</strong>n I’d like to ask you about how us<strong>in</strong>g <strong>the</strong> system impacts on yourwork.2
AppendicesPart 1. Experience <strong>of</strong> EPR use -1. Can you talk me through how you use <strong>the</strong> current system to do (EPRfunction)?Prompts: explore -What is it that <strong>the</strong>y do? When, where, how and with whom?How does <strong>the</strong> EPR <strong>in</strong>fluence <strong>the</strong> way <strong>the</strong>y th<strong>in</strong>k, make decisions?How does <strong>the</strong> EPR impact on <strong>the</strong>ir <strong>in</strong>teraction with o<strong>the</strong>r staff/patients?Do <strong>the</strong>y th<strong>in</strong>k <strong>the</strong> EPR affects <strong>the</strong> care patients receive? If so how?2. Did you use <strong>the</strong> previous system? If so how does <strong>the</strong> current (EPRfunction) compare with previous ways <strong>of</strong> work<strong>in</strong>g?Prompts: explore negative/positive changes <strong>in</strong> <strong>the</strong>ir -Behaviour - How <strong>the</strong>y used to th<strong>in</strong>k, make decisionsTheir relationships with o<strong>the</strong>r staff/patients3. How easy or difficult is it to use <strong>the</strong> current system to do (EPRfunction)?Prompts: explore -Ease <strong>of</strong> access (physical and cognitive barriers and facilitators)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> <strong>the</strong>ir workWhat stops <strong>the</strong>m us<strong>in</strong>g it – what helps <strong>the</strong>m use it?Their knowledge <strong>of</strong> <strong>the</strong> EPR – how was <strong>the</strong> <strong>in</strong>formation given?Tra<strong>in</strong><strong>in</strong>g and support received & <strong>the</strong> process <strong>of</strong> <strong>in</strong>fo. giv<strong>in</strong>g and shar<strong>in</strong>g <strong>of</strong> ideasThe perception <strong>of</strong> <strong>the</strong>ir personal capabilities3
AppendicesPart 2. Process <strong>of</strong> implementation4. Were you <strong>in</strong>volved <strong>the</strong> process <strong>of</strong> implementation? If so how <strong>in</strong>volved?Prompts: explore – <strong>the</strong> relationship between <strong>the</strong>mselves and managementHow happy were <strong>the</strong>y about any consultation process?Do <strong>the</strong>y feel <strong>the</strong>ir views were heard/ valued?Do <strong>the</strong>y feel <strong>the</strong>ir <strong>in</strong>put was valued/ is valuable?5. How important do you th<strong>in</strong>k hav<strong>in</strong>g (EPR function) is?Prompts: explore -User acceptance and satisfactionHow motivated, efficacious, do <strong>the</strong>y feel about <strong>the</strong> us<strong>in</strong>g <strong>the</strong> EPR function?Areas <strong>of</strong> resistance - conflict - are <strong>the</strong>re o<strong>the</strong>r priorities/pressures?Part 3 Impact on work -6. What are <strong>the</strong> consequences (negative and positive) <strong>of</strong> us<strong>in</strong>g (not us<strong>in</strong>g)<strong>the</strong> EPR?Prompts: explore impact on -Staff relationships/rolesWork efficiency – cl<strong>in</strong>ical decision-mak<strong>in</strong>gPatient care – do patients receive better/worse care?7. Do you th<strong>in</strong>k (<strong>the</strong> EPR) could be improved? If so how?Prompts: explore -4
AppendicesUsers expectations <strong>of</strong> <strong>the</strong> EPR versus <strong>the</strong> current reality.How can <strong>the</strong> positive effects <strong>of</strong> EPRs be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use <strong>of</strong> <strong>the</strong> EPR?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use <strong>of</strong> <strong>the</strong> EPR?8. Do you th<strong>in</strong>k <strong>the</strong> EPR and NCRS will impact on your future work<strong>in</strong>gpractices? If so how?Prompts: explore -Future impact on work<strong>in</strong>g practices, cl<strong>in</strong>ical management and <strong>in</strong>dividual patient care.If time9. Do you th<strong>in</strong>k EPRs and NPf<strong>IT</strong> <strong>in</strong> general will impact on <strong>the</strong> future <strong>of</strong> <strong>the</strong><strong>NHS</strong>?Prompts:General impact on <strong>the</strong> organisation and patient care.What are <strong>the</strong>ir perceptions <strong>of</strong> <strong>the</strong> best way forward?10. How will <strong>the</strong> Trust respond to <strong>the</strong>se changes?5
AppendicesPrompts: explore both positive and negative responses.11. Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments beforeend<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 4NCRS Implementation Project - Interview ScheduleLevel 2a – EPR use (Project management)Date and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Questions -1. How is <strong>the</strong> process <strong>of</strong> implementation?2. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> (function) – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong>impact <strong>of</strong> <strong>NHS</strong>CRS policy.3. How is (function) experienced by end-users? Does (function) currentlyimpact on work<strong>in</strong>g practices? And if so how?Preamble -Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to capture your experiences <strong>of</strong> implement<strong>in</strong>g(function), particularly factors that have facilitated or h<strong>in</strong>dered implementation. Weare also <strong>in</strong>terested <strong>in</strong> users experiences <strong>of</strong> <strong>the</strong> system. The <strong>in</strong>terview will last nomore than one hour and with your permission will be tape recorded – just to help meremember what was said later on. To reassure you, all <strong>in</strong>formation obta<strong>in</strong>ed will beanonymised. Nei<strong>the</strong>r <strong>the</strong> trust nor <strong>in</strong>dividual staff will be identified, when <strong>the</strong> researchis written up, with all names and staff positions anonymised. You will have anopportunity to read <strong>the</strong> draft f<strong>in</strong>al report to make factual corrections. You will alsoreceive an executive summary and be able to attend a sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong>f<strong>in</strong>d<strong>in</strong>gs. Do you have any questions before we start?2
Appendices1. Previously, provid<strong>in</strong>g (function) was <strong>the</strong> responsibility <strong>of</strong> local trusts. TheNational Program for Information Technology (NPf<strong>IT</strong>) has now decided amore centrally controlled standardised approach is needed. What do youth<strong>in</strong>k about this decision?Prompts: explore wider [political/ organisational] factors that have <strong>in</strong>fluenced thisdecisionWill centrally controlled solutions be better or worse?2. In implement<strong>in</strong>g (function) - can you give me any <strong>in</strong>sights <strong>in</strong>to how th<strong>in</strong>gswent?Prompts: explore <strong>the</strong> trust’s past experiences <strong>of</strong> implementation.Previous <strong>in</strong>-house successes and failuresAny specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. How does <strong>the</strong> new system differ from <strong>the</strong> previous way <strong>of</strong> do<strong>in</strong>g th<strong>in</strong>gs?Prompts: explore negative/positive changes <strong>in</strong> –Output – speed, accuracy, detailAvailability <strong>of</strong> <strong>in</strong>formation - Integrity, completeness, compliance with best practice4. What do you th<strong>in</strong>k have been some <strong>of</strong> <strong>the</strong> barriers to implementation?Prompts: explore -Ease <strong>of</strong> use/access (physical and cognitive barriers)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> workChanges <strong>in</strong> culturePhysical, <strong>in</strong>formational and organisational resources (costs) that have facilitated orh<strong>in</strong>dered <strong>IT</strong> implementation.3
Appendices5. What could <strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong>(function) implementation?Prompts:Explore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong>.The <strong>in</strong>formation systems currently <strong>in</strong> use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.6. In terms <strong>of</strong> fur<strong>the</strong>r prepar<strong>in</strong>g for NCRS solutions what do you th<strong>in</strong>k needs tobe done at (trust)?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong>national solutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore anystructural changes and strategy documents (obta<strong>in</strong> if available).7. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.8. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).4
Appendices9. Across <strong>the</strong> trust, how much agreement do you th<strong>in</strong>k <strong>the</strong>re is about <strong>the</strong>importance <strong>of</strong> (function)?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.10. In implement<strong>in</strong>g (function) – where do you see future potential areas <strong>of</strong>difficulty?Prompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities.Differ<strong>in</strong>g agendasExplore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?11. Do you th<strong>in</strong>k (function) could be improved? If so how?Prompts: explore -How can <strong>the</strong> positive effects be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use?12. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g a fully electronic (function)service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.5
Appendices13. For you what constitutes implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?14. How can this success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement, improved communication and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time -15. How do you th<strong>in</strong>k (function) and NCRS will impact on <strong>the</strong> future <strong>of</strong> <strong>the</strong><strong>NHS</strong>?Prompts:General impact on <strong>the</strong> organisation and patient care.What are <strong>the</strong>ir perceptions <strong>of</strong> <strong>the</strong> best way forward?Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 5NCRS Implementation Project - Interview ScheduleLevel 2ai – EPR use (e-book<strong>in</strong>g project management)Date and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Questions -4. How is <strong>the</strong> process <strong>of</strong> implementation?5. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> e-book<strong>in</strong>g? – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong>impact <strong>of</strong> <strong>NHS</strong>CRS policy.6. How is e-book<strong>in</strong>g experienced by end-users? Does e-book<strong>in</strong>g currentlyimpact on work<strong>in</strong>g practices? And if so how?Preamble -Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to capture your experiences <strong>of</strong> implement<strong>in</strong>g e-book<strong>in</strong>g (also Choose & Book), particularly factors that have facilitated or h<strong>in</strong>deredimplementation. We are also <strong>in</strong>terested <strong>in</strong> users experiences <strong>of</strong> <strong>the</strong> system. The<strong>in</strong>terview will last no more than one hour and with your permission will be taperecorded – just to help me remember what was said later on. To reassure you, all<strong>in</strong>formation obta<strong>in</strong>ed will be anonymised. Nei<strong>the</strong>r <strong>the</strong> trust nor <strong>in</strong>dividual staff will beidentified, when <strong>the</strong> research is written up, with all names and staff positionsanonymised. You will have an opportunity to read <strong>the</strong> draft f<strong>in</strong>al report to makefactual corrections. You will also receive an executive summary and be able to attenda sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs. Do you have any questions before we start?2
Appendices1. Previously, book<strong>in</strong>g appo<strong>in</strong>tments was <strong>the</strong> responsibility <strong>of</strong> local trusts.The National Program for Information Technology (NPf<strong>IT</strong>) has now decideda more centrally controlled standardised approach is needed. What do youth<strong>in</strong>k about this decision?Prompts: explore wider [political/ organisational] factors that have <strong>in</strong>fluenced thisdecisionWill centrally controlled solutions be better or worse?2. Before becom<strong>in</strong>g an earlier adopter <strong>of</strong> Choose & Book <strong>the</strong> Trust had a pilote-book<strong>in</strong>g system <strong>in</strong> place - can you give me any <strong>in</strong>sights <strong>in</strong>to how th<strong>in</strong>gswent?Prompts: explore <strong>the</strong> trust’s past experiences <strong>of</strong> implementation.Previous <strong>in</strong>-house successes and failuresAny specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. How does <strong>the</strong> new system differ from <strong>the</strong> pilot?Prompts: explore negative/positive changes <strong>in</strong> –Output – speed, accuracy, detailAvailability <strong>of</strong> <strong>in</strong>formation - Integrity, completeness, compliance with best practice4. What do you th<strong>in</strong>k have been some <strong>of</strong> <strong>the</strong> barriers to implementation?Prompts: explore -Ease <strong>of</strong> use/access (physical and cognitive barriers)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> workChanges <strong>in</strong> culture3
AppendicesPhysical, <strong>in</strong>formational and organisational resources (costs) that have facilitated orh<strong>in</strong>dered <strong>IT</strong> implementation.5. What could <strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong>e-book<strong>in</strong>g implementation?Prompts:Explore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong>.The <strong>in</strong>formation systems currently <strong>in</strong> use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.6. In terms <strong>of</strong> fur<strong>the</strong>r prepar<strong>in</strong>g for e-book<strong>in</strong>g and NCRS what do you th<strong>in</strong>kneeds to be done at (trust)?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong>national solutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore anystructural changes and strategy documents (obta<strong>in</strong> if available).7. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.8. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).4
Appendices9. Across <strong>the</strong> trust, how much agreement do you th<strong>in</strong>k <strong>the</strong>re is about <strong>the</strong>importance <strong>of</strong> e-book<strong>in</strong>g/Choose & Book?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.10. In implement<strong>in</strong>g e-book<strong>in</strong>g – where do you see future potential areas <strong>of</strong>difficulty?Prompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities.Differ<strong>in</strong>g agendasExplore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?11. Do you th<strong>in</strong>k e-book<strong>in</strong>g could be improved? If so how?Prompts: explore -How can <strong>the</strong> positive effects be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use?12. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g a fully electronic book<strong>in</strong>g service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.5
Appendices13. For you what would constitute implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?14. How can this success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement, improved communication and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time -15. How do you th<strong>in</strong>k e-book<strong>in</strong>g/Choose & Book and NCRS will impact on <strong>the</strong>future <strong>of</strong> <strong>the</strong> <strong>NHS</strong>?Prompts:General impact on <strong>the</strong> organisation and patient care.What are <strong>the</strong>ir perceptions <strong>of</strong> <strong>the</strong> best way forward?Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 6EPR Implementation Project - Interview ScheduleLevel 2 - Organisational Context and e-book<strong>in</strong>g projectmanagement - Chief ExecutiveDate and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Questions -7. How is <strong>the</strong> process <strong>of</strong> implementation?8. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> e-book<strong>in</strong>g? – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong>impact <strong>of</strong> <strong>NHS</strong>CRS policy.Preamble -Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to capture managers’ experiences <strong>of</strong> EPRs,particularly e-book<strong>in</strong>g, look<strong>in</strong>g at factors that facilitate or h<strong>in</strong>der successfulimplementation. The <strong>in</strong>terview will last no more than one hour and with yourpermission will be tape recorded – just to help me remember what was said later on.To reassure you, all <strong>in</strong>formation obta<strong>in</strong>ed will be anonymised. Nei<strong>the</strong>r <strong>the</strong> trust nor<strong>in</strong>dividual staff will be identified, when <strong>the</strong> research is written up, with all names andstaff positions anonymised. You will have an opportunity to read <strong>the</strong> draft f<strong>in</strong>al reportto make factual corrections. You will also receive an executive summary and be ableto attend a sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Before we beg<strong>in</strong>, do you have any questions, anyth<strong>in</strong>g I have not covered?2
AppendicesOK. Firstly, I’d like to ask you some general questions about <strong>the</strong> National Programmefor <strong>IT</strong>, <strong>the</strong>n I’d like to ask you about EPR implementation at (<strong>the</strong> trust).NPf<strong>IT</strong> <strong>in</strong> general -1. Previously, reach<strong>in</strong>g national targets regard<strong>in</strong>g <strong>the</strong> implementation <strong>of</strong> EPRswas primarily <strong>the</strong> responsibility <strong>of</strong> local trusts. The National Program forInformation Technology (NPf<strong>IT</strong>) has now decided a more centrallycontrolled approach is needed. What do you th<strong>in</strong>k about this decision?Prompts: explore wider organisational factors specific to <strong>the</strong> <strong>NHS</strong> that haveh<strong>in</strong>dered <strong>IT</strong> implementation?What would have helped?Will centrally controlled solutions be better or worse?2. What do you th<strong>in</strong>k were some <strong>of</strong> <strong>the</strong> barriers to implementation, and whatcould <strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong> EPRdevelopment?Prompts: explore physical, <strong>in</strong>formational and organisational resources (costs)that have facilitated or h<strong>in</strong>dered <strong>IT</strong> implementation.Explore <strong>the</strong> relationship between Trust Managers and <strong>the</strong> <strong>in</strong>formation system <strong>in</strong>use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.3. In terms <strong>of</strong> prepar<strong>in</strong>g for <strong>the</strong> new LSP solutions what do you th<strong>in</strong>k needs tobe done at (trust)?3
AppendicesPrompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong> LSPsolutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore any structuralchanges and strategy documents (obta<strong>in</strong> if available).4. In terms <strong>of</strong> fur<strong>the</strong>r prepar<strong>in</strong>g for e-book<strong>in</strong>g/Choose& Book and NCRS whatdo you th<strong>in</strong>k needs to be done at (trust)?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong>national solutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore anystructural changes and strategy documents (obta<strong>in</strong> if available).5. What could <strong>the</strong> trust could have done differently to achieve a higher level <strong>of</strong>e-book<strong>in</strong>g implementation?Prompts:Explore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong>.The <strong>in</strong>formation systems currently <strong>in</strong> use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.6. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.7. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).8. Across <strong>the</strong> trust, how much agreement do you th<strong>in</strong>k <strong>the</strong>re is about <strong>the</strong>importance <strong>of</strong> e-book<strong>in</strong>g?4
AppendicesPrompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.9. In implement<strong>in</strong>g e-book<strong>in</strong>g – where do you see future potential areas <strong>of</strong>difficulty?Prompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities.Differ<strong>in</strong>g agendasExplore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?10. Do you th<strong>in</strong>k e-book<strong>in</strong>g could be improved? If so how?Prompts: explore -How can <strong>the</strong> positive effects be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use?11. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g a fully electronic book<strong>in</strong>g service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.12. For you what would constitute implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?13. How can this success be best achieved?5
AppendicesPrompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement, improved communication and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time -14. How do you th<strong>in</strong>k e-book<strong>in</strong>g/Choose & Book and NCRS will impact on <strong>the</strong>future <strong>of</strong> <strong>the</strong> <strong>NHS</strong>?Prompts:General impact on <strong>the</strong> organisation and patient care.What are <strong>the</strong>ir perceptions <strong>of</strong> <strong>the</strong> best way forward?15. Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments beforeend<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAppendix 7NCRS Implementation Project - Interview ScheduleLevel 2b – EPR use (e-book<strong>in</strong>g project management: second<strong>in</strong>terview)Date and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> focus -9. How is implementation progress<strong>in</strong>g?10. How is <strong>the</strong> process <strong>of</strong> implementation?11. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> e-book<strong>in</strong>g? – specifically exam<strong>in</strong><strong>in</strong>g <strong>the</strong>impact <strong>of</strong> <strong>NHS</strong>CRS policy.12. How is e-book<strong>in</strong>g experienced by end-users? Does e-book<strong>in</strong>g currentlyimpact on work<strong>in</strong>g practices? And if so how?1. What are your current thoughts about Choose & Book? Do you th<strong>in</strong>k it’sachievable? Do you th<strong>in</strong>k it’s someth<strong>in</strong>g that’s worth achiev<strong>in</strong>g?Prompts: explore wider [political/ organisational] factors that have <strong>in</strong>fluenced thisdecisionWill centrally controlled solutions be better or worse?Do people want choice? Is <strong>the</strong> choice real?2. As an earlier adopter <strong>of</strong> Choose & Book can you tell me how implementationhas been go<strong>in</strong>g?Prompts: explore <strong>the</strong> trust’s experiences <strong>of</strong> implementation.In-house successes and failuresAny specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. How does <strong>the</strong> new version differ from <strong>the</strong> previous versions? How will/hasthis make a difference?Prompts: explore negative/positive changes <strong>in</strong> –Output – speed, accuracy, detailAvailability <strong>of</strong> <strong>in</strong>formation - Integrity, completeness, compliance with best practice4. What do you th<strong>in</strong>k have been some <strong>of</strong> <strong>the</strong> barriers to implementation?Prompts: explore - GP’s <strong>in</strong>putEase <strong>of</strong> use/access (physical and cognitive barriers)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> work2
AppendicesChanges <strong>in</strong> culturePhysical, <strong>in</strong>formational and organisational resources (costs) that have facilitated orh<strong>in</strong>dered <strong>IT</strong> implementation.5. What could <strong>the</strong> 1. <strong>the</strong> national programme and 2. <strong>the</strong> trust could have donedifferently to achieve a higher level <strong>of</strong> e-book<strong>in</strong>g implementation?Prompts:Explore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong>.The <strong>in</strong>formation systems currently <strong>in</strong> use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.6. In terms <strong>of</strong> fur<strong>the</strong>r prepar<strong>in</strong>g for e-book<strong>in</strong>g and NCRS what do you th<strong>in</strong>kneeds to be done at 1. national level and 2. trust level ?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong>national solutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore anystructural changes and strategy documents (obta<strong>in</strong> if available).7. Across <strong>the</strong> trust and nationally, how much agreement do you th<strong>in</strong>k <strong>the</strong>re isabout <strong>the</strong> importance <strong>of</strong> e-book<strong>in</strong>g/Choose & Book?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.8. In implement<strong>in</strong>g e-book<strong>in</strong>g – where do you see future potential areas <strong>of</strong>difficulty?Prompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities. Differ<strong>in</strong>g agendasExplore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?3
Appendices9. Do you th<strong>in</strong>k e-book<strong>in</strong>g could still be improved? If so how?Prompts: explore -How can <strong>the</strong> positive effects be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use?10. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g a fully electronic book<strong>in</strong>g service?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.11. For you what would constitute implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?12. How can this future success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement, improved communication and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time -13. How do you th<strong>in</strong>k e-book<strong>in</strong>g/Choose & Book and NCRS will impact on <strong>the</strong>future <strong>of</strong> <strong>the</strong> <strong>NHS</strong>?Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.4
AppendicesAppendix 8NCRS Implementation Project - Interview ScheduleLevel 2b – EPR use (test-order<strong>in</strong>g: second <strong>in</strong>terview)Date and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Role <strong>in</strong> EPR implementation:Duration <strong>of</strong> <strong>in</strong>terview:YES NO DateInformation sheet GIVENAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> focus -13. How is implementation progress<strong>in</strong>g?14. How is <strong>the</strong> process <strong>of</strong> implementation?15. What contextual factors (historically and currently) act as facilitators orbarriers to <strong>the</strong> implementation <strong>of</strong> e-test order<strong>in</strong>g? – specifically exam<strong>in</strong><strong>in</strong>g<strong>the</strong> impact <strong>of</strong> <strong>NHS</strong>CRS policy.1. What are your current thoughts about national e-test order<strong>in</strong>g? Do youth<strong>in</strong>k it’s achievable? Do you th<strong>in</strong>k it’s someth<strong>in</strong>g that’s worth achiev<strong>in</strong>g?Prompts: explore wider [political/ organisational] factors that have <strong>in</strong>fluenced thisdecisionWill centrally controlled solutions be better or worse?Do people want choice? Is <strong>the</strong> choice real?2. As an earlier adopter <strong>of</strong> e-test order<strong>in</strong>g at Barnet - but not at chase - you tellme how future implementation has been go<strong>in</strong>g?Prompts: explore <strong>the</strong> trust’s experiences <strong>of</strong> implementation.In-house successes and failuresAny specific difficulties encountered - medical/ legal/ staff<strong>in</strong>g problems.3. What do you th<strong>in</strong>k have been some <strong>of</strong> <strong>the</strong> barriers to implementation?Prompts: explore – PFIEase <strong>of</strong> use/access (physical and cognitive barriers)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> workChanges <strong>in</strong> culturePhysical, <strong>in</strong>formational and organisational resources (costs) that have facilitated orh<strong>in</strong>dered <strong>IT</strong> implementation.4. What could <strong>the</strong> 1. <strong>the</strong> national programme and 2. <strong>the</strong> trust could have donedifferently to achieve a higher level <strong>of</strong> implementation?Prompts:2
AppendicesExplore <strong>the</strong> relationship between Trust Managers and NPf<strong>IT</strong>.The <strong>in</strong>formation systems currently <strong>in</strong> use.Explore <strong>the</strong> role <strong>of</strong> wider organisational pressures – such as achiev<strong>in</strong>goperational targets.5. In terms <strong>of</strong> fur<strong>the</strong>r prepar<strong>in</strong>g for e-test order<strong>in</strong>g and NCRS what do youth<strong>in</strong>k needs to be done at 1. national level and 2. trust level ?Prompts: explore <strong>the</strong> change management associated with plann<strong>in</strong>g for <strong>the</strong>national solutions - sett<strong>in</strong>g goals, staff consultation, tra<strong>in</strong><strong>in</strong>g etc. Explore anystructural changes and strategy documents (obta<strong>in</strong> if available).6. Across <strong>the</strong> trust and nationally, how much agreement do you th<strong>in</strong>k <strong>the</strong>re isabout <strong>the</strong> importance <strong>of</strong> e-test order<strong>in</strong>g?Prompts: explore organisational commitment to implementation – across <strong>the</strong>trust and with<strong>in</strong> different groups.The role <strong>of</strong> constant change <strong>in</strong> management teams and <strong>the</strong> <strong>NHS</strong> generally.Explore whe<strong>the</strong>r high levels <strong>of</strong> change has impacted on <strong>IT</strong> focus and staffcommitment? Explore <strong>the</strong> perceived commitment <strong>of</strong> different groups.7. Who is driv<strong>in</strong>g <strong>the</strong>se changes with<strong>in</strong> <strong>the</strong> trust?Prompts: explore <strong>the</strong> role <strong>of</strong> leaders and super-users - <strong>the</strong> organisational impact<strong>of</strong> key players.8. How do you see your role impact<strong>in</strong>g on <strong>the</strong> process <strong>of</strong> implementation?Prompts: explore how motivated, efficacious, and <strong>in</strong>volved <strong>the</strong>y are.Explore <strong>the</strong> organisational impact <strong>of</strong> <strong>the</strong>ir personal <strong>in</strong>vestment (or lack <strong>of</strong> it).9. In implement<strong>in</strong>g e-test order<strong>in</strong>g – where do you see future potential areas <strong>of</strong>difficulty?Prompts: explore issues <strong>of</strong> ‘organisational fit’ and goal conflict – o<strong>the</strong>r pressuresand priorities. Differ<strong>in</strong>g agendas3
AppendicesExplore perceptions <strong>of</strong> what NCRS should deliver aga<strong>in</strong>st what is perceived asbe<strong>in</strong>g rolled out -Any organisational divide between mangers/cl<strong>in</strong>icians/<strong>IT</strong> staff’s expectations and<strong>the</strong> deliverables?10. Do you th<strong>in</strong>k e-test order<strong>in</strong>g could still be improved? If so how?Prompts: explore -How can <strong>the</strong> positive effects be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use?11. What are <strong>the</strong> consequences <strong>of</strong> achiev<strong>in</strong>g a fully electronic order<strong>in</strong>g serviceacross both sites?Prompts: explore positive and negative outcomes - national and organisational.Explore impact on staff roles, relationships and patient care.12. For you what would constitute implementation success?Prompts: explore how <strong>the</strong> mean<strong>in</strong>g <strong>of</strong> success is def<strong>in</strong>ed, at what level, and forwhom – <strong>the</strong> trust, <strong>the</strong> LSP or <strong>the</strong> National Program?13. How can this future success be best achieved?Prompts: explore factors <strong>the</strong>y consider necessary for success – such as staffrelations, cl<strong>in</strong>ician engagement, improved communication and f<strong>in</strong>ance.How <strong>the</strong>se can be factors be achieved and whe<strong>the</strong>r <strong>the</strong>y th<strong>in</strong>k <strong>the</strong>se factors willbe forthcom<strong>in</strong>g?If time -14. How do you th<strong>in</strong>k NCRS will impact on <strong>the</strong> future <strong>of</strong> <strong>the</strong> <strong>NHS</strong>?Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments before end<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.4
AppendicesAppendix 9EPR Implementation Project - Interview ScheduleLevel 2c – EPR use – tra<strong>in</strong>erDate and time <strong>of</strong> <strong>in</strong>terview:Interview code no:Name <strong>of</strong> Trust:Name <strong>of</strong> respondent:Title <strong>of</strong> respondent:Department/ speciality:Length <strong>of</strong> time respondent has been <strong>in</strong> that post:Use <strong>of</strong> EPR <strong>in</strong> post:Duration <strong>of</strong> <strong>in</strong>terview:Information sheet GIVENYES NO DateAnonymity EXPLAINEDVerbal permission to be taped REQUESTEDVerbal permission to be taped RECEIVEDConsent form GIVENConsent form RECEIVEDThank you letter sent1
AppendicesMa<strong>in</strong> Questions -How is <strong>the</strong> process <strong>of</strong> implementation and specifically tra<strong>in</strong><strong>in</strong>g ?How are specific areas <strong>of</strong> EPR functionality experienced by end-users?Does EPR use impact on current work<strong>in</strong>g practices? And if so how?Preamble –Thank you for agree<strong>in</strong>g to take part <strong>in</strong> this research study.Just to reiterate, <strong>the</strong> study has been funded by <strong>the</strong> <strong>NHS</strong> Service Delivery andOrganisation R&D Programme. The aim is to evaluate <strong>the</strong> process <strong>of</strong> implement<strong>in</strong>gelectronic patient records, or <strong>NHS</strong> Care Record Systems, as <strong>the</strong>y are now called, <strong>in</strong>acute trusts.There are two ma<strong>in</strong> elements to <strong>the</strong> study, a quantitative analysis <strong>of</strong> <strong>the</strong> costs andsav<strong>in</strong>gs associated with <strong>the</strong> implementation <strong>of</strong> EPRs, and a qualitative analysis <strong>of</strong> <strong>the</strong>organisational impact <strong>of</strong> implementation.The focus <strong>of</strong> this set <strong>of</strong> <strong>in</strong>terviews is to explore your experiences <strong>of</strong> us<strong>in</strong>g <strong>in</strong>formationtechnology (EPRs) <strong>in</strong> do<strong>in</strong>g your job. The <strong>in</strong>terview will last no more than one hourand with your permission will be tape recorded – just to help me remember what wassaid later on. To reassure you, all <strong>in</strong>formation obta<strong>in</strong>ed will be anonymised. Nei<strong>the</strong>r<strong>the</strong> trust nor <strong>in</strong>dividual staff will be identified, when <strong>the</strong> research is written up, with allnames and staff positions anonymised. You will have an opportunity to read <strong>the</strong> draftf<strong>in</strong>al report to make factual corrections. You will also receive an executive summaryand be able to attend a sem<strong>in</strong>ar dissem<strong>in</strong>at<strong>in</strong>g <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs.Before we beg<strong>in</strong>, do you have any questions, anyth<strong>in</strong>g I have not covered?OK. Firstly, I’d like to ask you some general questions about what’s its like to use <strong>the</strong>current system, <strong>the</strong>n I’d like to ask you about how us<strong>in</strong>g <strong>the</strong> system impacts on yourwork.2
AppendicesPart 1. Experience <strong>of</strong> EPR use -12. Can you talk me through how staff use <strong>the</strong> current (EPRfunction) system?Prompts: explore -What is it that <strong>the</strong>y do? When, where, how and with whom?How does <strong>the</strong> EPR <strong>in</strong>fluence <strong>the</strong> way <strong>the</strong>y th<strong>in</strong>k, make decisions?How does <strong>the</strong> EPR impact on <strong>the</strong>ir <strong>in</strong>teraction with o<strong>the</strong>r staff/patients?Do <strong>the</strong>y th<strong>in</strong>k <strong>the</strong> EPR affects <strong>the</strong> care patients receive? If so how?13. Did you teach people to use <strong>the</strong> previous system? If so can you talk methrough what <strong>the</strong>y have to do differently?Prompts: explore negative/positive changes <strong>in</strong> <strong>the</strong>ir -Behaviour -How <strong>the</strong>y used to th<strong>in</strong>k, make decisionsTheir relationships with o<strong>the</strong>r staff/patients14. How does us<strong>in</strong>g <strong>the</strong> (EPR function) compare with previous ways <strong>of</strong>work<strong>in</strong>g?Prompts: explore negative/positive changes <strong>in</strong> changes <strong>in</strong> –Output – speed, accuracy, detail <strong>of</strong> resultsAvailability <strong>of</strong> <strong>in</strong>formation - Integrity, completeness, compliance with best practice3
Appendices15. How easy or difficult is it to teach staff to use <strong>the</strong> current (EPRfunction)?Prompts: explore -Ease <strong>of</strong> access (physical and cognitive barriers)Changes <strong>in</strong> <strong>the</strong> organisation (flow) <strong>of</strong> <strong>the</strong>ir workTheir knowledge <strong>of</strong> <strong>the</strong> EPR – how was <strong>the</strong> <strong>in</strong>formation given?Tra<strong>in</strong><strong>in</strong>g and support received & <strong>the</strong> process <strong>of</strong> <strong>in</strong>fo. giv<strong>in</strong>g and shar<strong>in</strong>g <strong>of</strong> ideasThe perception <strong>of</strong> <strong>the</strong>ir personal capabilitiesPart 2. Process <strong>of</strong> implementation16. Were you <strong>in</strong>volved <strong>the</strong> process <strong>of</strong> implementation? If so how <strong>in</strong>volved?Prompts: explore – <strong>the</strong> relationship between <strong>the</strong>mselves and managementHow happy were <strong>the</strong>y about any consultation process?Do <strong>the</strong>y feel <strong>the</strong>ir views were heard/ valued?Do <strong>the</strong>y feel <strong>the</strong>ir <strong>in</strong>put was valued/ is valuable?17. How important do you th<strong>in</strong>k hav<strong>in</strong>g (EPR function) is?Prompts: explore -User acceptance and satisfactionHow motivated, efficacious, do <strong>the</strong>y feel about <strong>the</strong> us<strong>in</strong>g <strong>the</strong> EPR function?Areas <strong>of</strong> resistance - conflict - are <strong>the</strong>re o<strong>the</strong>r priorities/pressures?4
AppendicesPart 3 Impact on work -18. What are <strong>the</strong> consequences (negative and positive) <strong>of</strong> us<strong>in</strong>g (not us<strong>in</strong>g)<strong>the</strong> EPR?Prompts: explore impact on -Staff relationships/rolesWork efficiency – cl<strong>in</strong>ical decision-mak<strong>in</strong>gPatient care – do patients receive better/worse care?19. Do you th<strong>in</strong>k (<strong>the</strong> EPR) could be improved? If so how?Prompts: explore -Users expectations <strong>of</strong> <strong>the</strong> EPR versus <strong>the</strong> current reality.How can <strong>the</strong> positive effects <strong>of</strong> EPRs be maximised?What physical or resource factors h<strong>in</strong>der or facilitate use <strong>of</strong> <strong>the</strong> EPR?What social/organisational <strong>in</strong>fluences h<strong>in</strong>der or facilitate use <strong>of</strong> <strong>the</strong> EPR?20. Do you th<strong>in</strong>k <strong>the</strong> EPR will impact on your future work<strong>in</strong>g practices? If sohow?Prompts: explore -Future impact on work<strong>in</strong>g practices, cl<strong>in</strong>ical management and <strong>in</strong>dividual patient care.5
AppendicesIf time21. Do you th<strong>in</strong>k EPRs and NPf<strong>IT</strong> <strong>in</strong> general will impact on <strong>the</strong> future <strong>of</strong> <strong>the</strong><strong>NHS</strong>?Prompts:General impact on <strong>the</strong> organisation and patient care.What are <strong>the</strong>ir perceptions <strong>of</strong> <strong>the</strong> best way forward?22. How will <strong>the</strong> Trust will respond to <strong>the</strong>se changes?Prompts: explore both positive and negative responses.23. Lastly – whe<strong>the</strong>r <strong>the</strong>y would like to make any o<strong>the</strong>r comments beforeend<strong>in</strong>gThank <strong>the</strong>m aga<strong>in</strong> – please call me if you have any future questions.6
AppendicesAPPENDIX 10 - Data sourcesCDS Inpatient variables*LOCAL PATIENT IDENTIFIERADMISSION METHODSTART DATE (HOSP<strong>IT</strong>AL PROVIDERSPELL)Related outcomesAll primary outcomesEmergency re-admission (with<strong>in</strong> 28 days)All outcomesEND DATE (HOSP<strong>IT</strong>AL PROVIDER SPELL) All outcomesDISCHARGE METHODTREATMENT FUNCTIONINTENDED MANAGEMENT* <strong>NHS</strong> Data Dictionary v3.0DeathsTime-to-deathAll outcomesRatio <strong>of</strong> actual to <strong>in</strong>tended day casesCDS Outpatient variables*LOCAL PATIENT IDENTIFIERTREATMENT FUNCTIONATTENDED OR DID NOT ATTENDOUTCOMEATTENDANCE DATE* <strong>NHS</strong> Data Dictionary v3.0Related outcomesAll primary outcomesAll outcomesAttendance (Attended vs Did Not Attend)Outcome (discharged vs follow-up)All outcomesPathology laboratory variablesLocal patient identifierTest typeDate test orderedRelated outcomesAll primary outcomesAll primary outcomesAll primary outcomesRadiology department variablesLocal patient identifierExam<strong>in</strong>ation typeDate exam requestedRelated outcomesAll primary outcomesAll primary outcomesAll primary outcomes1
AppendicesAPPENDIX 11.1 - CPOE, primary outcomes, between-Trust comparisonsShad<strong>in</strong>g represents <strong>the</strong> ‘<strong>in</strong>tervention’ Trust.Pathology test type=Full Blood Count Period Trust 1 Trust 2 Trust 3 Trust 4Tests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200564.4% - 43.9% 73.9%65.1% - 40.7% 75.4%66.3% 74.0% 48.8% 71.2%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous non-zeroresponse (tests/day)Tests per day case - proportion with non-zeroresponse20002001-20022003-200520002001-20022003-20050.59 - 0.60 0.620.61 - 0.62 0.610.64 0.69 0.66 0.614.4% - 6.6% 14.0%4.9% - 6.5% 15.0%10.9% 19.6% 11.6% 13.3%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-200545.3% - 43.0% 45.4%46.6% - 46.5% 45.1%46.9% 52.9% 49.0% 47.0%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with test(s)20002001-20022003-200520002001-20022003-200511.2% - 5.4% 9.7%9.8% - 7.2% 13.5%9.3% 10.4% 9.7% 14.5%17.9% - 12.3% 16.1%19.6% - 20.3% 20.4%18.5% 23.0% 18.3% 18.7%Pathology test type=Urea & Electrolytes Period Trust A Trust B Trust C Trust DTests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200549.6% - 35.4% 61.2%51.2% - 36.7% 63.1%57.4% - 42.3% 64.8%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (tests/day)Tests per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.56 - 0.50 0.640.58 - 0.52 0.620.64 - 0.59 0.652.2% - 4.7% 9.9%2.7% - 5.5% 10.7%10.2% - 7.7% 18.7%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-200550.1% - 49.0% 52.4%51.6% - 50.6% 50.6%49.9% - 52.6% 49.8%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with test(s)20002001-20022003-200520002001-20022003-20056.9% - 5.3% 5.9%6.2% - 7.5% 7.9%6.3% - 9.3% 9.0%10.0% - 6.9% 14.7%10.4% - 12.4% 16.4%14.3% - 14.5% 19.0%2
AppendicesPathology test type=Ur<strong>in</strong>e Culture Period Trust 1 Trust 2 Trust 3 Trust 4Tests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200525.8% - 12.0% 32.9%23.2% - 14.6% 34.0%21.5% 22.9% 17.4% 34.8%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (tests/day)Tests per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.37 - 0.33 0.400.35 - 0.40 0.390.36 0.35 0.41 0.411.4% - 1.5% 5.0%1.3% - 4.6% 5.0%3.3% 3.5% 3.9% 5.0%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-20058.6% - 6.7% 9.7%6.9% - 5.7% 9.7%7.2% 9.7% 6.0% 10.2%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatient20002001-20022003-200520004.0% - 1.2% 3.5%3.6% - 1.6% 4.7%3.5% 2.4% 1.5% 6.2%10.6% - 5.3% 11.2%appo<strong>in</strong>tment - proportion <strong>of</strong> outpatient2001-20029.8% - 6.4% 12.4%appo<strong>in</strong>tments with test(s)2003-200511.0% 9.6% 5.9% 15.1%3
AppendicesAPPENDIX 11.2 - CPOE, primary outcomes, with<strong>in</strong>-Trust comparisonShad<strong>in</strong>g represents <strong>the</strong> ‘<strong>in</strong>tervention’ specialties.Pathology test type=Full Blood Count Period ObstetricsAll o<strong>the</strong>rspecialtiesTests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200548.8% 73.1%51.3% 73.3%56.7% 74.1%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (tests/day)Tests per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.62 0.540.67 0.540.74 0.589.5% 4.6%11.4% 5.6%13.4% 11.6%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-200527.2% 48.0%29.8% 49.2%33.3% 51.0%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with test(s)20002001-20022003-200520002001-20022003-200516.5% 10.3%16.5% 8.6%17.8% 7.9%9.8% 19.7%9.7% 22.8%11.7% 20.7%Pathology test type= Urea & Electrolytes Period ObstetricsAll o<strong>the</strong>rspecialtiesTests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200515.2% 63.5%14.6% 65.5%18.4% 72.3%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (tests/day)Tests per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.54 0.520.56 0.530.65 0.604.8% 2.3%5.1% 3.4%7.1% 10.7%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-200530.6% 51.3%34.0% 52.8%38.9% 53.0%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with test(s)20002001-20022003-200520002001-20022003-20053.8% 7.3%4.4% 6.4%6.4% 6.2%10.7% 9.9%12.4% 10.1%16.1% 14.1%4
AppendicesPathology test type=Ur<strong>in</strong>e Culture Period ObstetricsAll o<strong>the</strong>rspecialtiesTests per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200533.5% 28.6%28.7% 26.4%18.6% 27.9%IPTests per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (tests/day)Tests per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.48 0.280.46 0.260.57 0.276.6% 1.0%4.8% 0.9%4.6% 3.0%Test with<strong>in</strong> 48hrs <strong>of</strong> previous test <strong>of</strong> sametype - proportion <strong>of</strong> all tests20002001-20022003-20058.4% 9.1%7.1% 7.1%8.0% 8.0%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more tests requestedTest <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with test(s)20002001-20022003-200520002001-20022003-200516.0% 2.3%12.9% 2.1%14.5% 1.9%14.6% 6.6%12.3% 7.2%15.9% 5.8%5
AppendicesAPPENDIX 12.1 - PACS, primary outcomes, between-Trust comparisonsShad<strong>in</strong>g represents <strong>the</strong> ‘<strong>in</strong>tervention’ Trust.Radiology exam<strong>in</strong>ation type = Pla<strong>in</strong> Film Period Trust 1 Trust 2 Trust 3 Trust 4Exams per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-200539.8% 36.6% 39.2% 42.4%39.3% 39.2% 36.2% 41.4%39.9% 45.5% 42.4% 43.4%IPExams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)Exams per day case - proportion with nonzeroresponse20002001-20022003-200520002001-20022003-20050.49 0.43 0.49 0.410.48 0.39 0.44 0.420.50 0.46 0.50 0.435.0% 5.2% 2.6% 3.8%4.6% 5.4% 2.2% 5.5%9.8% 11.8% 6.7% 10.8%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams20002001-20022003-200520.8% 26.5% 22.5% 18.8%21.1% 21.8% 19.9% 16.9%19.9% 21.4% 15.6% 15.6%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)20002001-20022003-200520002001-20022003-20053.3% 5.9% 8.6% 4.0%3.1% 6.2% 8.3% 5.1%3.0% 6.1% 8.7% 5.0%14.2% 21.1% 16.2% 22.5%16.5% 20.1% 24.1% 20.4%17.5% 22.1% 25.7% 21.3%Radiology exam<strong>in</strong>ation type = Computed Tomography Period Trust 1 Trust 2 Trust 3 Trust 4Exams per <strong>in</strong>patient day - non-zero vs zeroresponse20002001-20022003-20055.4% 5.3% 4.9% 8.1%7.1% 6.7% 5.1% 8.9%8.9% 8.9% 6.7% 10.2%Exams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)20002001-20022003-20050.22 0.19 0.25 0.190.24 0.18 0.24 0.200.28 0.21 0.31 0.21IPExams per day case - proportion with nonzeroresponse20002001-20022003-20050.3% 0.4% 0.2% 0.4%0.4% 0.5% 0.3% 0.6%1.1% 0.8% 1.0% 1.2%Exams per day case - proportion with nonzeroresponse20002001-20022003-20050.3% 0.4% 0.2% 0.5%0.4% 0.5% 0.3% 0.6%1.1% 0.8% 1.0% 1.2%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams20002001-20022003-20054.0% 2.2% 2.1% 1.2%4.5% 1.7% 1.6% 2.5%4.4% 1.8% 1.7% 2.4%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)20002001-20022003-200520002001-20022003-20050.03% 0.07% 0.18% 0.02%0.08% 0.08% 0.19% 0.09%0.25% 0.07% 0.23% 0.21%n/a n/a n/a n/a6
AppendicesRadiology exam<strong>in</strong>ation type = Ultrasound Period Trust 1 Trust 2 Trust 3 Trust 4Exams per <strong>in</strong>patient day - proportion withnon-zero response20002001-20022003-200511.0% 14.0% 13.7% 14.3%11.9% 13.6% 13.1% 13.0%14.2% 13.5% 12.5% 13.0%Exams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)20002001-20022003-20050.035 0.047 0.052 0.0460.038 0.045 0.052 0.0400.055 0.041 0.048 0.039IPExams per day case - proportion with nonzeroresponse20002001-20022003-20052.4% 2.2% 3.8% 1.3%2.7% 2.0% 3.7% 1.9%3.3% 1.8% 2.7% 1.8%Exams per day case - proportion with nonzeroresponse20002001-20022003-20052.4% 2.2% 3.8% 1.8%2.7% 2.0% 3.7% 1.9%3.3% 1.8% 2.7% 1.8%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams20002001-20022003-20055.3% 3.3% 3.6% 3.0%4.8% 3.1% 3.7% 2.7%6.3% 3.3% 3.3% 3.2%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)20002001-20022003-200520002001-20022003-20050.4% 2.8% 2.6% 1.9%0.7% 2.4% 2.4% 3.1%1.8% 1.6% 2.1% 3.8%4.8% 20.7% 18.3% 22.2%3.7% 19.2% 21.8% 10.7%7.1% 10.6% 19.6% 11.8%7
AppendicesAPPENDIX 12.2 - PACS, primary outcomes, with<strong>in</strong>-Trust comparisonNo shad<strong>in</strong>g, because <strong>the</strong> ‘<strong>in</strong>tervention’ specialties depended on <strong>the</strong> time period / comparisonconsidered (see Methods for quantitative elements <strong>of</strong> <strong>the</strong> study).Radiology exam<strong>in</strong>ation type = Pla<strong>in</strong> FilmPeriodTrauma &OrthopaedicsAll o<strong>the</strong>rspecialtiesExams per <strong>in</strong>patient day - non-zero vs zeroresponse01/2000-11/200112/2001-10/200211/2002-12/200572.2% 35.1%70.9% 33.3%66.0% 35.7%IPExams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)Exams per day case - proportion with nonzeroresponse01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/20050.495 0.3640.515 0.3820.574 0.37810.1% 3.1%7.6% 3.4%22.1% 4.6%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams01/2000-11/200112/2001-10/200211/2002-12/200523.1% 16.6%20.6% 15.1%19.1% 14.8%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/200530.4% 2.1%28.1% 2.1%30.1% 1.7%22.9% 5.3%26.8% 7.1%27.6% 6.2%Radiology exam<strong>in</strong>ation type = Computed TomographyPeriodTrauma &OrthopaedicsAll o<strong>the</strong>rspecialtiesExams per <strong>in</strong>patient day - non-zero vs zeroresponse01/2000-11/200112/2001-10/200211/2002-12/20055.6% 8.1%6.0% 8.5%7.1% 9.1%IPExams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)Exams per day case - proportion with nonzeroresponse01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/20050.201 0.1810.154 0.1890.281 0.1950.5% 0.4%0.6% 0.5%2.5% 0.6%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams01/2000-11/200112/2001-10/200211/2002-12/2005(6/220) 2.7% 2.2%(2/118) 1.7% 2.2%(17/540) 3.2% 2.4%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/2005n/an/an/an/a8
AppendicesRadiology exam<strong>in</strong>ation type = UltrasoundPeriodTrauma &OrthopaedicsAll o<strong>the</strong>rspecialtiesExams per <strong>in</strong>patient day - non-zero vs zeroresponse01/2000-11/200112/2001-10/200211/2002-12/20054.9% 13.0%4.9% 12.6%6.4% 12.1%IPExams per <strong>in</strong>patient day - cont<strong>in</strong>uous nonzeroresponse (exams/day)Exams per day case - proportion with nonzeroresponse01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/20050.127 0.3090.166 0.3050.211 0.2980.2% 1.2%0.1% 1.5%1.2% 1.2%Exam with<strong>in</strong> 48hrs <strong>of</strong> previous exam <strong>of</strong>same type - proportion <strong>of</strong> all exams01/2000-11/200112/2001-10/200211/2002-12/2005(8/207) 3.9% 2.9%(1/98) 1.0% 3.1%(16/515) 3.1% 3.4%OPProportion <strong>of</strong> outpatient appo<strong>in</strong>tments atwhich one or more exams requestedExam <strong>of</strong> same type at next outpatientappo<strong>in</strong>tment - proportion <strong>of</strong> outpatientappo<strong>in</strong>tments with exam(s)01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/2005n/an/an/an/a9
AppendicesAPPENDIX 13.1 - CPOE and PACS, secondary outcomes, between-TrustcomparisonShad<strong>in</strong>g represents <strong>the</strong> ‘<strong>in</strong>tervention’ Trusts.Secondary outcomes Period Trust 1 Trust 2 Trust 3 Trust 4Mean length <strong>of</strong> stay (days), exclud<strong>in</strong>g daycases20002001-20022003-20055.966.005.677.186.936.665.025.114.736.817.197.11Day cases as proportion <strong>of</strong> admitted patients20002001-20022003-200541.1%40.4%45.4%31.8%33.7%37.2%41.4%42.0%48.4%32.3%30.1%35.0%IPActual to <strong>in</strong>tended day cases (proportion <strong>of</strong><strong>in</strong>tended day cases admitted overnight)Emergency re-admission (with<strong>in</strong> 28 days)20002001-20022003-200520002001-20022003-2005no dataavailable2.8%3.4%4.1%12.0%10.0%6.2%2.8%2.8%4.2%5.3%4.5%4.3%2.4%2.4%3.1%6.6%6.0%3.6%4.3%4.5%5.8%Deaths20002001-20022003-20052.0%1.8%1.7%1.8%2.1%2.1%1.3%1.5%1.1%2.2%2.3%1.9%Mean time-to-death (days)20002001-20022003-200521.223.123.514.814.615.813.213.914.517.517.718.4OPAttendance (proportion attend<strong>in</strong>g)Outcome (proportion discharged)20002001-20022003-200520002001-20022003-200585.8%85.5%86.0%61.1%61.9%63.7%80.1%80.0%82.3%no dataavailable89.0%90.1%91.1%45.3%51.9%55.4%81.9%82.7%83.4%46.7%46.4%43.3%10
AppendicesAPPENDIX 13.2 - CPOE, secondary outcomes, with<strong>in</strong>-Trust comparisonShad<strong>in</strong>g represents <strong>the</strong> ‘<strong>in</strong>tervention’ specialties.Secondary outcomes Period ObstetricsAll o<strong>the</strong>rspecialtiesMean length <strong>of</strong> stay (days), exclud<strong>in</strong>g day cases20002001-20022003-20052.882.802.496.666.696.37Day cases as proportion <strong>of</strong> admitted patients20002001-20022003-200526.3%28.5%22.0%43.6%42.4%48.7%IPActual to <strong>in</strong>tended day cases (proportion <strong>of</strong> <strong>in</strong>tended day casesadmitted overnight)Emergency re-admission (with<strong>in</strong> 28 days)20002001-20022003-200520002001-20022003-2005n/an/an/a3.3%4.0%4.7%Deaths20002001-20022003-2005n/a2.3%2.2%2.0%Mean time-to-death (days)20002001-20022003-2005n/a21.223.123.5OPAttendance (proportion attend<strong>in</strong>g)Outcome (proportion discharged)20002001-20022003-200520002001-20022003-200590.4%89.7%87.3%74.1%76.1%80.7%85.4%85.1%85.9%59.1%59.6%60.9%11
AppendicesAPPENDIX 13.3 - PACS, secondary outcomes, with<strong>in</strong>-Trust comparisonNo shad<strong>in</strong>g, because <strong>the</strong> ‘<strong>in</strong>tervention’ specialties depended on <strong>the</strong> time period / comparisonconsidered (see Methods for quantitative elements <strong>of</strong> <strong>the</strong> study).Secondary outcomesPeriodTrauma &OrthopaedicsAll o<strong>the</strong>rspecialtiesMean length <strong>of</strong> stay (days), exclud<strong>in</strong>g day cases01/2000-11/200112/2001-10/200211/2002-12/20059.079.717.996.607.086.99Day cases as proportion <strong>of</strong> admitted patients01/2000-11/200112/2001-10/200211/2002-12/200534.4%32.2%49.4%31.2%29.5%31.9%IPActual to <strong>in</strong>tended day cases (proportion <strong>of</strong> <strong>in</strong>tended daycases admitted overnight)Emergency re-admission (with<strong>in</strong> 28 days)01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/20056.3%8.1%3.5%3.1%3.4%5.5%6.5%5.3%3.8%4.4%4.9%5.8%Deaths01/2000-11/200112/2001-10/200211/2002-12/20051.0%1.4%0.7%2.4%2.4%2.2%Mean time-to-death (days)01/2000-11/200112/2001-10/200211/2002-12/200530.124.025.617.515.717.9OPAttendance (proportion attend<strong>in</strong>g)Outcome (proportion discharged)01/2000-11/200112/2001-10/200211/2002-12/200501/2000-11/200112/2001-10/200211/2002-12/200584.1%84.7%85.7%55.7%56.6%56.2%81.9%82.7%83.0%44.6%44.3%40.5%12
DisclaimerThis report presents <strong>in</strong>dependent research commissioned by <strong>the</strong> NationalInstitute for Health Research (NIHR). The views and op<strong>in</strong>ions expressed byauthors <strong>in</strong> this publication are those <strong>of</strong> <strong>the</strong> authors and do not necessarily reflectthose <strong>of</strong> <strong>the</strong> <strong>NHS</strong>, <strong>the</strong> NIHR, <strong>the</strong> NIHR SDO programme or <strong>the</strong> Department <strong>of</strong>Health. The views and op<strong>in</strong>ions expressed by <strong>the</strong> <strong>in</strong>terviewees <strong>in</strong> this publicationare those <strong>of</strong> <strong>the</strong> <strong>in</strong>terviewees and do not necessarily reflect those <strong>of</strong> <strong>the</strong> authors,those <strong>of</strong> <strong>the</strong> <strong>NHS</strong>, <strong>the</strong> NIHR, <strong>the</strong> NIHR SDO programme or <strong>the</strong> Department <strong>of</strong>HealthAddendumThis document was published by <strong>the</strong> National Coord<strong>in</strong>at<strong>in</strong>g Centre for <strong>the</strong>Service Delivery and Organisation (NCCSDO) research programme, managedby <strong>the</strong> London School <strong>of</strong> Hygiene & Tropical Medic<strong>in</strong>e.The management <strong>of</strong> <strong>the</strong> Service Delivery and Organisation (SDO) programmehas now transferred to <strong>the</strong> National Institute for Health Research <strong>Evaluation</strong>s,Trials and Studies Coord<strong>in</strong>at<strong>in</strong>g Centre (<strong>NETSCC</strong>) based at <strong>the</strong> University <strong>of</strong>Southampton. Prior to April 2009, <strong>NETSCC</strong> had no <strong>in</strong>volvement <strong>in</strong> <strong>the</strong>commission<strong>in</strong>g or production <strong>of</strong> this document and <strong>the</strong>refore we may not be ableto comment on <strong>the</strong> background or technical detail <strong>of</strong> this document. Should youhave any queries please contact sdo@southampton.ac.uk.