- Page 2 and 3:
ii2014 Practitioner and Provider Ma
- Page 4 and 5:
iv2014 Practitioner and Provider Ma
- Page 6 and 7:
vi2014 Practitioner and Provider Ma
- Page 8 and 9:
Nurse Advice Line .................
- Page 10 and 11:
Pharmacy Benefits .................
- Page 12 and 13:
Clearinghouses ....................
- Page 14 and 15:
Site Visits .......................
- Page 16:
Monitoring ........................
- Page 19 and 20:
Federally Funded Terminations .....
- Page 21 and 22:
Appendix A. Acronyms ..............
- Page 23 and 24:
1. Presbyterian Healthcare Services
- Page 25 and 26:
Presbyterian Healthcare Services(HS
- Page 27 and 28:
Presbyterian Healthcare ServicesReg
- Page 29 and 30:
Presbyterian Healthcare Services2.
- Page 31 and 32:
Provider Network Managementthis man
- Page 33 and 34:
Centennial Care Overview3. Primary
- Page 35 and 36:
Primary Care ProvidersClaims Activi
- Page 37 and 38:
Primary Care Providers4. Specialist
- Page 39 and 40:
SpecialistsOther Information for PC
- Page 41 and 42:
Specialists5. Preventive Health Car
- Page 43 and 44:
Preventive Health Care GuidelinesPr
- Page 45 and 46:
Preventive Health Care GuidelinesSe
- Page 47 and 48:
Care Coordination6. Care Coordinati
- Page 49 and 50:
Care CoordinationPresbyterian’s c
- Page 51 and 52:
Care Coordinationthe program. If th
- Page 53 and 54:
Care Coordinationdesignated family
- Page 55 and 56:
Care CoordinationFacilitate access
- Page 57 and 58:
Care CoordinationClinical Practice
- Page 59 and 60:
Care Coordinationformula, which is
- Page 61 and 62:
Care CoordinationAmerican Psychiatr
- Page 63 and 64:
Care Coordinationwithout obtaining
- Page 65 and 66:
Care CoordinationSpecialists as PCP
- Page 67 and 68:
Care Coordinationor when the member
- Page 69 and 70:
Care Coordination11. Prevention Scr
- Page 71 and 72:
Care CoordinationFollow-up plans or
- Page 73 and 74:
Care CoordinationPharmacy BenefitsP
- Page 75 and 76:
Care CoordinationThis page intentio
- Page 77 and 78:
Laboratory ServicesTriCore Contact
- Page 79 and 80:
Pharmacya multi-tier formulary stru
- Page 81 and 82:
Pharmacymedications. This multi-tie
- Page 83 and 84:
PharmacyCatastrophic coverage: Cove
- Page 85 and 86:
Pharmacywhich drugs are mandated th
- Page 87 and 88:
PharmacyThe drug must be accepted f
- Page 89 and 90:
PharmacyTypes of Pharmacy Prior Aut
- Page 91 and 92:
PharmacyThis page intentionally lef
- Page 93 and 94:
Behavioral Healthagreements, addend
- Page 95 and 96:
Behavioral HealthForm W-9Staff rost
- Page 97 and 98:
Behavioral Healthhttps://www.phs.or
- Page 99 and 100:
Behavioral HealthAn initial PCP con
- Page 101 and 102:
Behavioral HealthAccess StandardsMe
- Page 103 and 104:
Behavioral HealthThere is no charge
- Page 105 and 106:
Behavioral HealthThis page intentio
- Page 107 and 108:
Long-Term Carean individual provide
- Page 109 and 110:
Long-Term Careavailable services, a
- Page 111 and 112:
Long-Term Carethe agent to members
- Page 113 and 114:
Long-Term Carecare at the right tim
- Page 115 and 116:
Long-Term Careplanning process, and
- Page 117 and 118:
Long-Term Carebudget plan are suffi
- Page 119 and 120:
Long-Term CareOrganizationsFor the
- Page 121 and 122:
Home HealthPresbyterian’s credent
- Page 123 and 124:
Home HealthPresbyterian Medicaid me
- Page 125 and 126:
Home Healththese services. Services
- Page 127 and 128:
Home Healthfor review will be submi
- Page 129 and 130:
Home HealthPatient Care Conferences
- Page 131 and 132:
Home HealthThis page intentionally
- Page 133 and 134:
Quality Improvement ProgramNational
- Page 135 and 136:
Quality Improvement Programcomplian
- Page 137 and 138:
Quality Improvement Programresults
- Page 139 and 140:
Quality Improvement Programrespect
- Page 141 and 142:
Quality Improvement ProgramPresbyte
- Page 143 and 144:
Quality Improvement ProgramNCQA ori
- Page 145 and 146:
Quality Improvement ProgramThis pag
- Page 147 and 148:
Health Insurance Portability and Ac
- Page 149 and 150:
Health Insurance Portability and Ac
- Page 151 and 152:
Legalabove, nor from any recourse a
- Page 153 and 154:
Legalagreement with Presbyterian fo
- Page 155 and 156:
Legaltransactions (federal, state,
- Page 157 and 158:
Legalcontractual relationship with
- Page 159 and 160:
Legalcomply with all state and fede
- Page 161 and 162:
Legalany such program during the te
- Page 163 and 164:
LegalPrompt Pay by PresbyterianPres
- Page 165 and 166:
Legal15. Fraud, Waste, and Abuse15.
- Page 167 and 168:
Fraud, Waste, and Abuseas the time
- Page 169 and 170:
Fraud, Waste, and AbuseAll document
- Page 171 and 172:
Fraud, Waste, and AbuseVerifying th
- Page 173 and 174:
Fraud, Waste, and AbuseHistorically
- Page 175 and 176:
Fraud, Waste, and Abuseis violated
- Page 177 and 178:
Fraud, Waste, and AbuseIs informed
- Page 179 and 180:
Fraud, Waste, and Abuse16. Credenti
- Page 181 and 182:
Credentialing and RecredentialingPr
- Page 183 and 184:
Credentialing and RecredentialingNe
- Page 185 and 186:
Credentialing and Recredentialing17
- Page 187 and 188:
e-BusinessFill out the form on the
- Page 189 and 190:
e-BusinessSign Up for this Free Ser
- Page 191 and 192:
e-BusinessClearinghouse Contact Inf
- Page 193 and 194:
e-Business18. Claims and Payment18.
- Page 195 and 196:
Claims and Paymentsubmission. Claim
- Page 197 and 198:
Claims and PaymentSpecify the origi
- Page 199 and 200:
Claims and Paymentrequiring a leadi
- Page 201 and 202:
Claims and PaymentPlease note that
- Page 203 and 204:
Claims and PaymentPresbyterian is r
- Page 205 and 206:
Claims and Paymentnot made a recove
- Page 207 and 208:
Claims and PaymentAcceptable docume
- Page 209 and 210:
Claims and Paymentallowing provider
- Page 211 and 212:
Claims and PaymentNational Correct
- Page 213 and 214:
Claims and Payment19. Presbyterian
- Page 215 and 216:
Presbyterian Customer Service Cente
- Page 217 and 218:
Presbyterian Customer Service Cente
- Page 219 and 220:
Presbyterian Customer Service Cente
- Page 221 and 222:
Presbyterian Customer Service Cente
- Page 223 and 224:
Presbyterian Customer Service Cente
- Page 225 and 226:
Presbyterian Customer Service Cente
- Page 227 and 228:
Appeals and Grievances20. Appeals a
- Page 229 and 230:
Appeals and GrievancesMember Appeal
- Page 231 and 232: Appendix A. AcronymsAppendix A. Acr
- Page 233 and 234: Appendix A. AcronymsHMOHRAHSDHealth
- Page 235 and 236: Appendix A. AcronymsWWEDIWorkgroup
- Page 237 and 238: Appendix B: DefinitionsAppendix B.
- Page 239 and 240: Appendix B. DefinitionsTerm Definit
- Page 241 and 242: Appendix B. DefinitionsTerm Definit
- Page 243 and 244: Appendix B. DefinitionsTerm Definit
- Page 245 and 246: Appendix B. DefinitionsTerm Definit
- Page 247 and 248: Appendix C. WebsitesAppendix C. Web
- Page 249 and 250: Appendix C. WebsitesWebsitesNameCul
- Page 251 and 252: Appendix C. WebsitesWebsitesNameMem
- Page 253 and 254: Appendix C. WebsitesWebsitesNameWED
- Page 255 and 256: Appendix C. WebsitesAppendix D. Pho
- Page 257 and 258: Appendix D. Phone NumbersPhone Numb
- Page 259 and 260: Appendix B: Business Associate Agre
- Page 261 and 262: Appendix E. Business Associate Agre
- Page 263 and 264: Appendix E. Business Associate Agre
- Page 265 and 266: Appendix F. Prior Authorization Gui
- Page 267 and 268: Appendix F. Prior Authorization Gui
- Page 269 and 270: Appendix F. Prior Authorization Gui
- Page 271 and 272: Appendix F. Prior Authorization Gui
- Page 273 and 274: Appendix F. Prior Authorization Gui
- Page 275 and 276: Appendix F. Prior Authorization Gui
- Page 277 and 278: Appendix F. Prior Authorization Gui
- Page 279 and 280: Appendix G. Alternative BenefitsG.
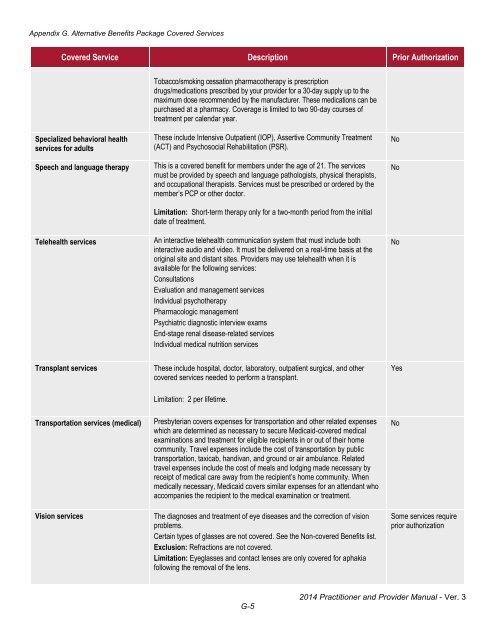
- Page 281: Appendix G. Alternative Benefits Pa
- Page 285: Appendix G. Alternative Benefits Pa