General Practice BILLING GUIDE - British Columbia Medical ...
General Practice BILLING GUIDE - British Columbia Medical ...
General Practice BILLING GUIDE - British Columbia Medical ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
APPENDIX i FORMS FOR THE GPSC INITIATIVES<br />
Chronic Disease Management<br />
E/2<br />
BRITISH<br />
COLUMBIA<br />
MEDICAL<br />
ASSOCIATION<br />
SUMMARY OF <strong>GUIDE</strong>LINE<br />
Guideline Effective Date: November 1, 2003<br />
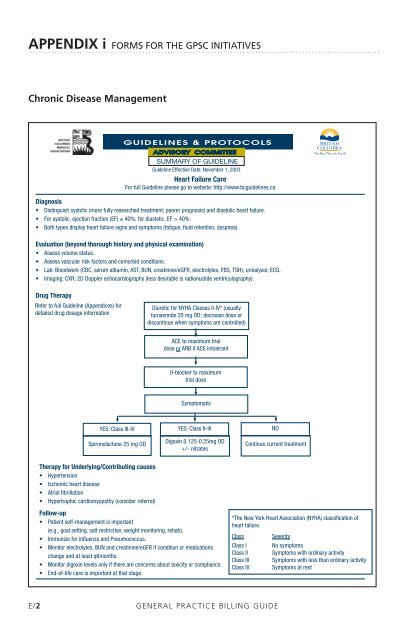
Heart Failure Care<br />
For full Guideline please go to website: http://www.bcguidelines.ca<br />
Diagnosis<br />
• Distinguish systolic (more fully researched treatment; poorer prognosis) and diastolic heart failure.<br />
• For systolic, ejection fraction (EF) ≤ 40%; for diastolic, EF > 40%.<br />
• Both types display heart failure signs and symptoms (fatigue, fluid retention, dyspnea).<br />
Evaluation (beyond thorough history and physical examination)<br />
• Assess volume status.<br />
• Assess vascular risk factors and comorbid conditions.<br />
• Lab: Bloodwork (CBC, serum albumin, AST, BUN, creatinine/eGFR, electrolytes, FBS, TSH); urinalysis; ECG.<br />
• Imaging: CXR; 2D Doppler echocardiography (less desirable is radionuclide ventriculography).<br />
Drug Therapy<br />
Refer to full Guideline (Appendices) for<br />
detailed drug dosage information<br />
YES: Class III-IV<br />
Spironolactone 25 mg OD<br />
Therapy for Underlying/Contributing causes<br />
• Hypertension<br />
• Ischemic heart disease<br />
• Atrial fibrillation<br />
• Hypertrophic cardiomyopathy (consider referral)<br />
Diuretic for NYHA Classes II-IV* (usually<br />
furosemide 20 mg OD; decrease dose or<br />
discontinue when symptoms are controlled)<br />
ACE to maximum trial<br />
dose or ARB if ACE intolerant<br />
ß-blocker to maximum<br />
trial dose<br />
Symptomatic<br />
YES: Class II-Ill<br />
Digoxin 0.125-0.25mg OD<br />
+/- nitrates<br />
Follow-up<br />
• Patient self-management is important<br />
(e.g., goal setting, salt restriction, weight monitoring, rehab).<br />
• Immunize for influenza and Pneumococcus.<br />
• Monitor electrolytes, BUN and creatinine/eGFR if condition or medications<br />
change and at least q6months.<br />
• Monitor digoxin levels only if there are concerns about toxicity or compliance.<br />
• End-of-life care is important at that stage.<br />
Continue current treatment<br />
GENERAL PRACTICE <strong>BILLING</strong> <strong>GUIDE</strong><br />
NO<br />
*The New York Heart Association (NYHA) classification of<br />
heart failure.<br />
Class Severity<br />
Class I No symptoms<br />
Class II Symptoms with ordinary activity<br />
Class III Symptoms with less than ordinary activity<br />
Class IV Symptoms at rest