


Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Fasciculus gracilis<br />
Fasciculus cuneatus<br />
Posterior<br />
spinocerebellar<br />
tract<br />
Lat.<br />
corticospinal<br />
tract<br />
Lat.<br />
spinothalamic<br />
tract<br />
Anterior<br />
spinocerebellar<br />
tract<br />
Posterior<br />
horn<br />
Anterior<br />
horn<br />
Anterior white commissure<br />
Anterior corticospinal tract<br />
Spinal Cord 55<br />
Ipsilateral loss of fine touch, conscious<br />
proprioception, and vibratory sense<br />
from lower limb<br />
Loss of of fine touch, conscious<br />
proprioception, and vibratory sense<br />
from upper limb<br />
Ipsilateral segmental anesthesia<br />
and areflexia<br />
Ipsilateral lower limb<br />
dystaxia<br />
Ipsilateral spastic<br />
paresis with<br />
pyramidal signs<br />
Contralateral lower<br />
limb dystaxia<br />
Contralateral loss of<br />
pain and temperature<br />
sensation one segment<br />
below lesion<br />
Ipsilateral flaccid paralysis<br />
in affected myotomes<br />
Bilateral loss of pain and temperature<br />
sensation within dermatomes<br />
of involved segments<br />
Mild contralateral muscle weakness<br />
in proximal muscles<br />
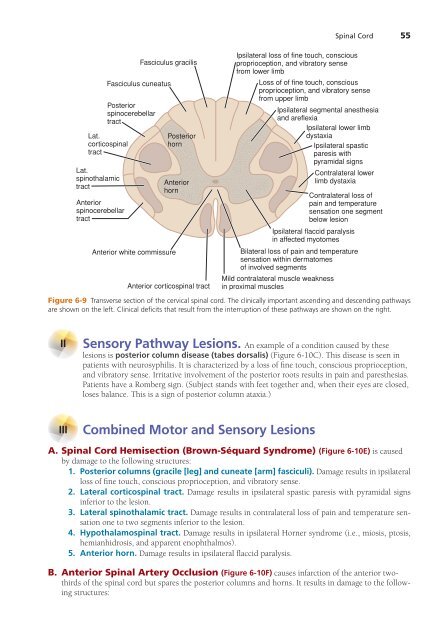
Figure 6-9 Transverse section of the cervical spinal cord. The clinically important ascending and descending pathways<br />
are shown on the left. Clinical deficits that result from the interruption of these pathways are shown on the right.<br />
II<br />
Sensory Pathway Lesions. An example of a condition caused by these<br />
lesions is posterior column disease (tabes dorsalis) (Figure 6-10C). This disease is seen in<br />
patients with neurosyphilis. It is characterized by a loss of fine touch, conscious proprioception,<br />
and vibratory sense. Irritative involvement of the posterior roots results in pain and paresthesias.<br />
Patients have a Romberg sign. (Subject stands with feet together and, when their eyes are closed,<br />
loses balance. This is a sign of posterior column ataxia.)<br />
III<br />
Combined Motor and Sensory Lesions<br />
A. Spinal Cord Hemisection (Brown-Séquard Syndrome) (Figure 6-10E) is caused<br />
by damage to the following structures:<br />
1. Posterior columns (gracile [leg] and cuneate [arm] fasciculi). Damage results in ipsilateral<br />
loss of fine touch, conscious proprioception, and vibratory sense.<br />
2. Lateral corticospinal tract. Damage results in ipsilateral spastic paresis with pyramidal signs<br />
inferior to the lesion.<br />
3. Lateral spinothalamic tract. Damage results in contralateral loss of pain and temperature sensation<br />
one to two segments inferior to the lesion.<br />
4. Hypothalamospinal tract. Damage results in ipsilateral Horner syndrome (i.e., miosis, ptosis,<br />
hemianhidrosis, and apparent enophthalmos).<br />
5. Anterior horn. Damage results in ipsilateral flaccid paralysis.<br />
B. Anterior Spinal Artery Occlusion (Figure 6-10F) causes infarction of the anterior twothirds<br />
of the spinal cord but spares the posterior columns and horns. It results in damage to the following<br />
structures: