Ground glass opacity on CT scanning of the chest: What does it mean?
Ground glass opacity on CT scanning of the chest: What does it mean?
Ground glass opacity on CT scanning of the chest: What does it mean?

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
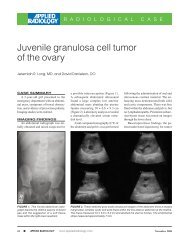
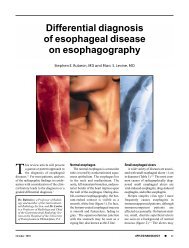
FIGURE 10. Br<strong>on</strong>chiol<strong>it</strong>is obl<strong>it</strong>erans organizing<br />
pneum<strong>on</strong>ia. Image is <strong>of</strong> a 50-year-old<br />
man w<strong>it</strong>h increasing shortness <strong>of</strong> breath after<br />
bilateral lung transplantati<strong>on</strong>. HR<strong>CT</strong> (1.0 mm<br />
collimati<strong>on</strong>) shows bilateral patchy areas <strong>of</strong><br />
GGO in both a br<strong>on</strong>chovascular and peripheral<br />
distributi<strong>on</strong>.<br />
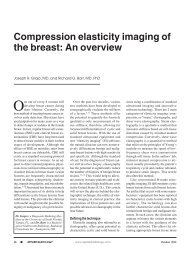
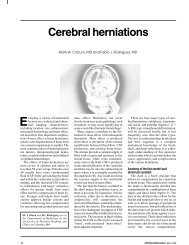
FIGURE 11. C<strong>on</strong>tusi<strong>on</strong>s. Image is <strong>of</strong> a 22year-old<br />
man involved in a motor vehicle accident.<br />
Helical <strong>CT</strong> scan (10 mm collimati<strong>on</strong>)<br />
shows bilateral areas <strong>of</strong> GGO and c<strong>on</strong>solidati<strong>on</strong><br />
in a typical peripheral n<strong>on</strong>-segmental distributi<strong>on</strong>.<br />
There are both posterior and anterior<br />
rib fractures adjacent to <strong>the</strong> s<strong>it</strong>es <strong>of</strong> c<strong>on</strong>tusi<strong>on</strong>.<br />
peripheral ring <strong>of</strong> hemorrhage or hemorrhagic<br />
infarcti<strong>on</strong> surrounding target<br />
lesi<strong>on</strong>s <strong>of</strong> pulm<strong>on</strong>ary aspergillosis (figure<br />
9). Several infectious and n<strong>on</strong>infectious<br />
causes <strong>of</strong> <strong>the</strong> <strong>CT</strong> halo sign have<br />
since been reported. 24 In most patients,<br />
hemorrhagic nodules can be distinguished<br />
from n<strong>on</strong>hemorrhagic nodules<br />
by <strong>the</strong> presence <strong>of</strong> a halo <strong>of</strong> GGO.<br />
Ano<strong>the</strong>r cause <strong>of</strong> focal GGO, or a<br />
nodule w<strong>it</strong>h a surrounding halo <strong>of</strong> GGO,<br />
is <strong>the</strong> post-biopsy pseudo nodule. These<br />
pseudo nodules have been described in<br />
Causes <strong>of</strong> a “halo” pattern <strong>of</strong><br />
GGO <strong>on</strong> <strong>CT</strong> <strong>scanning</strong><br />
• Invasive pulm<strong>on</strong>ary aspergillosis<br />
• Neoplasm, hemorrhagic<br />
• Post-biopsy pseudo nodule<br />
Table 4<br />
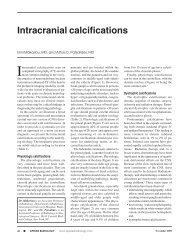
FIGURE 12. Desquamative interst<strong>it</strong>ial pneum<strong>on</strong><strong>it</strong>is.<br />
Image is <strong>of</strong> a 77-year-old man w<strong>it</strong>h a<br />
3-m<strong>on</strong>th history <strong>of</strong> increasing shortness <strong>of</strong><br />
breath. HR<strong>CT</strong> (1.5 mm collimati<strong>on</strong>) shows<br />
bilateral areas <strong>of</strong> GGO and c<strong>on</strong>solidati<strong>on</strong> in a<br />
peripheral distributi<strong>on</strong> w<strong>it</strong>hout evidence <strong>of</strong><br />
h<strong>on</strong>eycombing or tracti<strong>on</strong> br<strong>on</strong>chiectasis.<br />
patients who have underg<strong>on</strong>e lung transplantati<strong>on</strong><br />
and transbr<strong>on</strong>chial lung<br />
biopsy, 25 but <strong>the</strong>y may be seen in any<br />
patient after lung biopsy.<br />
A peripheral pattern <strong>of</strong> GGO—<br />
Processes that are known to result in a<br />
peripheral lung distributi<strong>on</strong> <strong>of</strong> GGO<br />
w<strong>it</strong>h HR<strong>CT</strong> <strong>scanning</strong> are listed in table<br />
5. This particular distributi<strong>on</strong> pattern<br />
can be very helpful in narrowing <strong>the</strong> differential<br />
diagnosis, especially when<br />
combined w<strong>it</strong>h o<strong>the</strong>r clinical data and<br />
associated <strong>CT</strong> scan findings.<br />
Br<strong>on</strong>chiol<strong>it</strong>is obl<strong>it</strong>erans organizing<br />
pneum<strong>on</strong>ia (BOOP) is a disease characterized<br />
histologically by <strong>the</strong> presence <strong>of</strong><br />
granulati<strong>on</strong> tissue plugs w<strong>it</strong>hin respiratory<br />
br<strong>on</strong>chioles and alveolar ducts, and<br />
organizing pneum<strong>on</strong>ia extending into<br />
<strong>the</strong> surrounding alveoli. 26 <strong>CT</strong> scans<br />
show patchy GGO (in 8 to 75% <strong>of</strong><br />
patients), nodules, or areas <strong>of</strong> c<strong>on</strong>solidati<strong>on</strong><br />
w<strong>it</strong>h a predominantly peripheral<br />
(50% <strong>of</strong> patients), bilateral, and n<strong>on</strong>segmental<br />
distributi<strong>on</strong> (figure 10). 27-29<br />
Collagen vascular diseases are multisystem<br />
disorders characterized by<br />
vascular changes, fibrosis, and inflammati<strong>on</strong><br />
<strong>of</strong> c<strong>on</strong>nective tissue. Specific<br />
diseases include progressive systemic<br />
sclerosis (scleroderma), systemic lupus<br />
ery<strong>the</strong>matosus, polymyos<strong>it</strong>is/dermatomyos<strong>it</strong>is,<br />
rheumatoid arthr<strong>it</strong>is, and Sjogren’s<br />
syndrome. GGO is seen <strong>on</strong> <strong>CT</strong><br />
<strong>scanning</strong> in 63 to 100% <strong>of</strong> <strong>the</strong>se<br />
patients, 30 and is a sign <strong>of</strong> active inflammati<strong>on</strong><br />
in <strong>the</strong> absence <strong>of</strong> significant h<strong>on</strong>eycombing,<br />
br<strong>on</strong>chiectasis, or o<strong>the</strong>r<br />
signs <strong>of</strong> lung fibrosis. 31<br />
Pulm<strong>on</strong>ary c<strong>on</strong>tusi<strong>on</strong> results from<br />
trauma to <strong>the</strong> <strong>chest</strong> wall and lung, w<strong>it</strong>h<br />
Causes <strong>of</strong> a peripheral pattern <strong>of</strong><br />
GGO <strong>on</strong> <strong>CT</strong> <strong>scanning</strong><br />
• Br<strong>on</strong>chiol<strong>it</strong>is obl<strong>it</strong>erans organizing<br />
pneum<strong>on</strong>ia (BOOP)<br />
• Collagen vascular disease<br />
• C<strong>on</strong>tusi<strong>on</strong><br />
• Desquamative interst<strong>it</strong>ial<br />
pneum<strong>on</strong><strong>it</strong>is<br />
• Drug toxic<strong>it</strong>y<br />
• Eosinophilic pneum<strong>on</strong>ia<br />
• Fibrosis<br />
• Sarcoidosis<br />
Table 5<br />
bleeding into <strong>the</strong> air spaces and lung<br />
interst<strong>it</strong>ium. Generally, <strong>the</strong> cause is a<br />
compressi<strong>on</strong> injury w<strong>it</strong>h significant<br />
kinetic energy absorpti<strong>on</strong> adjacent to <strong>the</strong><br />
s<strong>it</strong>e <strong>of</strong> <strong>chest</strong> wall injury. The <strong>CT</strong> scan<br />
appearance <strong>of</strong> lung c<strong>on</strong>tusi<strong>on</strong> is that <strong>of</strong><br />
ill-defined areas <strong>of</strong> GGO, c<strong>on</strong>solidati<strong>on</strong>,<br />
or both, usually w<strong>it</strong>h a peripheral, n<strong>on</strong>anatomic<br />
distributi<strong>on</strong> (figure 11). 32,33<br />
Desquamative interst<strong>it</strong>ial pneum<strong>on</strong><strong>it</strong>is<br />
is characterized by alveolar filling w<strong>it</strong>h<br />
macrophages. The HR<strong>CT</strong> scan findings<br />
c<strong>on</strong>sist <strong>of</strong> GGO w<strong>it</strong>h a lower lung z<strong>on</strong>e<br />
(73%) and a peripheral (59%) predominant<br />
distributi<strong>on</strong> (figure 12). Usual interst<strong>it</strong>ial<br />
pneum<strong>on</strong><strong>it</strong>is, or idiopathic<br />
pulm<strong>on</strong>ary fibrosis, results in a similar<br />
distributi<strong>on</strong> <strong>of</strong> GGO <strong>on</strong> <strong>CT</strong> <strong>scanning</strong> but<br />
typically w<strong>it</strong>h more areas <strong>of</strong> h<strong>on</strong>eycombing<br />
and tracti<strong>on</strong> br<strong>on</strong>chiectasis<br />
(figure 13).<br />
Pulm<strong>on</strong>ary toxic<strong>it</strong>y has been associated<br />
w<strong>it</strong>h numerous drugs and a variety<br />
<strong>of</strong> radiographic and <strong>CT</strong> patterns. <strong>CT</strong><br />
<strong>scanning</strong> shows nodular areas <strong>of</strong> GGO<br />
and c<strong>on</strong>solidati<strong>on</strong>, <strong>of</strong>ten w<strong>it</strong>h a peripheral<br />
distributi<strong>on</strong>. 35,36<br />
Pulm<strong>on</strong>ary eosinophilia occurs w<strong>it</strong>h a<br />
variety <strong>of</strong> c<strong>on</strong>d<strong>it</strong>i<strong>on</strong>s or diseases, or can<br />
be idiopathic. Chr<strong>on</strong>ic idiopathic<br />
eosinophilic pneum<strong>on</strong>ia is characterized<br />
by multiple dense areas <strong>of</strong> <str<strong>on</strong>g>opac<strong>it</strong>y</str<strong>on</strong>g> <strong>on</strong><br />
<strong>chest</strong> radiographs and <strong>CT</strong> scans. In <strong>on</strong>e<br />
study <strong>of</strong> patients w<strong>it</strong>h chr<strong>on</strong>ic<br />
eosinophilic pneum<strong>on</strong>ia, <strong>the</strong> most comm<strong>on</strong><br />
HR<strong>CT</strong> finding was GGO, usually<br />
adjacent to areas <strong>of</strong> c<strong>on</strong>solidati<strong>on</strong>, w<strong>it</strong>h<br />
a peripheral distributi<strong>on</strong>. 37 Acute idiopathic<br />
eosinophilic pneum<strong>on</strong>ia is characterized<br />
by diffuse GGO and<br />
micr<strong>on</strong>odules <strong>on</strong> <strong>chest</strong> radiographs and<br />
<strong>CT</strong> scans, <strong>of</strong>ten in a br<strong>on</strong>chovascular<br />
distributi<strong>on</strong>. 38<br />
20 APPLIED RADIOLOGY, December 1998