

Understanding Clinical Trial Design - Research Advocacy Network
Understanding Clinical Trial Design - Research Advocacy Network
Understanding Clinical Trial Design - Research Advocacy Network

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
30<br />
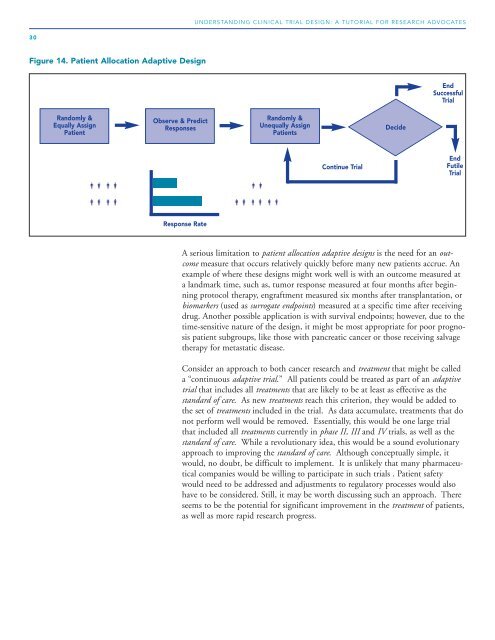
Figure 14. Patient Allocation Adaptive <strong>Design</strong><br />
Randomly &<br />
Equally Assign<br />
Patient<br />
Observe & Predict<br />
Responses<br />
Response Rate<br />
UNDERSTANDING CLINICAL TRIAL DESIGN: A TUTORIAL FOR RESEARCH ADVOCATES<br />
Randomly &<br />
Unequally Assign<br />
Patients<br />
Continue <strong>Trial</strong><br />
Decide<br />
End<br />
Successful<br />
<strong>Trial</strong><br />
End<br />
Futile<br />
<strong>Trial</strong><br />
A serious limitation to patient allocation adaptive designs is the need for an outcome<br />
measure that occurs relatively quickly before many new patients accrue. An<br />
example of where these designs might work well is with an outcome measured at<br />
a landmark time, such as, tumor response measured at four months after beginning<br />
protocol therapy, engraftment measured six months after transplantation, or<br />
biomarkers (used as surrogate endpoints) measured at a specific time after receiving<br />
drug. Another possible application is with survival endpoints; however, due to the<br />
time-sensitive nature of the design, it might be most appropriate for poor prognosis<br />
patient subgroups, like those with pancreatic cancer or those receiving salvage<br />
therapy for metastatic disease.<br />
Consider an approach to both cancer research and treatment that might be called<br />
a “continuous adaptive trial.” All patients could be treated as part of an adaptive<br />
trial that includes all treatments that are likely to be at least as effective as the<br />
standard of care. As new treatments reach this criterion, they would be added to<br />
the set of treatments included in the trial. As data accumulate, treatments that do<br />
not perform well would be removed. Essentially, this would be one large trial<br />
that included all treatments currently in phase II, III and IV trials, as well as the<br />
standard of care. While a revolutionary idea, this would be a sound evolutionary<br />
approach to improving the standard of care. Although conceptually simple, it<br />
would, no doubt, be difficult to implement. It is unlikely that many pharmaceutical<br />
companies would be willing to participate in such trials . Patient safety<br />
would need to be addressed and adjustments to regulatory processes would also<br />
have to be considered. Still, it may be worth discussing such an approach. There<br />
seems to be the potential for significant improvement in the treatment of patients,<br />
as well as more rapid research progress.