

Valeurs seuils pour le rapport coût-efficacité en soins de santé - KCE
Valeurs seuils pour le rapport coût-efficacité en soins de santé - KCE
Valeurs seuils pour le rapport coût-efficacité en soins de santé - KCE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>KCE</strong> reports 100 ICER Thresholds 9<br />
2 ICERS AND ICER THRESHOLD VALUES<br />
2.1 GENERAL PRINCIPLES OF ECONOMIC EVALUATION IN<br />
HEALTH CARE<br />
Economic evaluation is <strong>de</strong>fined as the comparative analysis of alternative courses of<br />
action in terms of both their costs and consequ<strong>en</strong>ces. 2 In economic evaluation of health<br />
care interv<strong>en</strong>tions, ‘consequ<strong>en</strong>ces’ are most oft<strong>en</strong> interpreted as ‘health effects’ or<br />
‘health outcomes’. Both terms will be used interchangeably in this report.<br />
Only evaluations that compare two or more alternatives and consi<strong>de</strong>r both costs and<br />
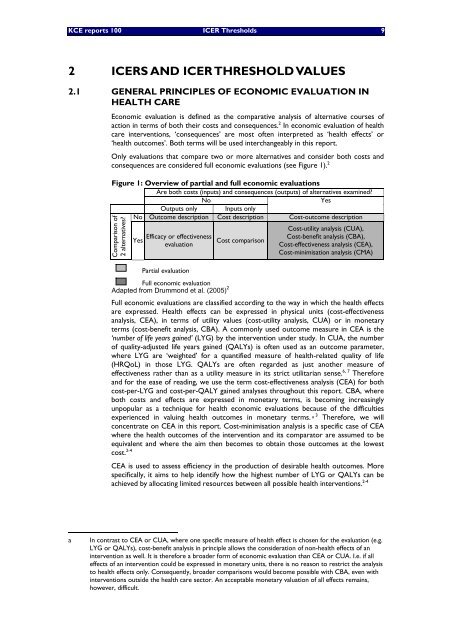
consequ<strong>en</strong>ces are consi<strong>de</strong>red full economic evaluations (see Figure 1). 2<br />
Figure 1: Overview of partial and full economic evaluations<br />
Are both costs (inputs) and consequ<strong>en</strong>ces (outputs) of alternatives examined?<br />
No<br />
Yes<br />
Outputs only Inputs only<br />
No Outcome <strong>de</strong>scription Cost <strong>de</strong>scription Cost-outcome <strong>de</strong>scription<br />
Cost-utility analysis (CUA),<br />
Efficacy or effectiv<strong>en</strong>ess<br />
Yes Cost comparison<br />
evaluation<br />
Cost-b<strong>en</strong>efit analysis (CBA),<br />
Cost-effectiv<strong>en</strong>ess analysis (CEA),<br />
Cost-minimisation analysis (CMA)<br />
Comparison of<br />
2 alternatives?<br />
Partial evaluation<br />
Adapted from Drummond et al. (2005) 2<br />
Full economic evaluation<br />
Full economic evaluations are classified according to the way in which the health effects<br />
are expressed. Health effects can be expressed in physical units (cost-effectiv<strong>en</strong>ess<br />
analysis, CEA), in terms of utility values (cost-utility analysis, CUA) or in monetary<br />
terms (cost-b<strong>en</strong>efit analysis, CBA). A commonly used outcome measure in CEA is the<br />
‘number of life years gained’ (LYG) by the interv<strong>en</strong>tion un<strong>de</strong>r study. In CUA, the number<br />
of quality-adjusted life years gained (QALYs) is oft<strong>en</strong> used as an outcome parameter,<br />
where LYG are ‘weighted’ for a quantified measure of health-related quality of life<br />
(HRQoL) in those LYG. QALYs are oft<strong>en</strong> regar<strong>de</strong>d as just another measure of<br />
effectiv<strong>en</strong>ess rather than as a utility measure in its strict utilitarian s<strong>en</strong>se. 6, 7 Therefore<br />
and for the ease of reading, we use the term cost-effectiv<strong>en</strong>ess analysis (CEA) for both<br />
cost-per-LYG and cost-per-QALY gained analyses throughout this report. CBA, where<br />
both costs and effects are expressed in monetary terms, is becoming increasingly<br />
unpopular as a technique for health economic evaluations because of the difficulties<br />
experi<strong>en</strong>ced in valuing health outcomes in monetary terms. a 3 Therefore, we will<br />
conc<strong>en</strong>trate on CEA in this report. Cost-minimisation analysis is a specific case of CEA<br />
where the health outcomes of the interv<strong>en</strong>tion and its comparator are assumed to be<br />
equiva<strong>le</strong>nt and where the aim th<strong>en</strong> becomes to obtain those outcomes at the lowest<br />
cost. 2-4<br />
CEA is used to assess effici<strong>en</strong>cy in the production of <strong>de</strong>sirab<strong>le</strong> health outcomes. More<br />
specifically, it aims to help id<strong>en</strong>tify how the highest number of LYG or QALYs can be<br />
achieved by allocating limited resources betwe<strong>en</strong> all possib<strong>le</strong> health interv<strong>en</strong>tions. 2-4<br />
a In contrast to CEA or CUA, where one specific measure of health effect is chos<strong>en</strong> for the evaluation (e.g.<br />
LYG or QALYs), cost-b<strong>en</strong>efit analysis in princip<strong>le</strong> allows the consi<strong>de</strong>ration of non-health effects of an<br />
interv<strong>en</strong>tion as well. It is therefore a broa<strong>de</strong>r form of economic evaluation than CEA or CUA. I.e. if all<br />
effects of an interv<strong>en</strong>tion could be expressed in monetary units, there is no reason to restrict the analysis<br />
to health effects only. Consequ<strong>en</strong>tly, broa<strong>de</strong>r comparisons would become possib<strong>le</strong> with CBA, ev<strong>en</strong> with<br />
interv<strong>en</strong>tions outsi<strong>de</strong> the health care sector. An acceptab<strong>le</strong> monetary valuation of all effects remains,<br />
however, difficult.














