Clinical Examination of Farm Animals - CYF MEDICAL DISTRIBUTION
Clinical Examination of Farm Animals - CYF MEDICAL DISTRIBUTION
Clinical Examination of Farm Animals - CYF MEDICAL DISTRIBUTION

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Clinical</strong> <strong>Examination</strong> <strong>of</strong> the Gastrointestinal System<br />
examination is usually limited to cattle over 12<br />
months <strong>of</strong> age and, to avoid creating a pneumorectum<br />
and tenesmus which may confuse abdominal<br />
auscultation and percussion, is the last part <strong>of</strong> the<br />
clinical examination.<br />
Rectal examination <strong>of</strong> the gastrointestinal tract can<br />
be used to detect a viscus which is displaced or enlarged.<br />
The rectal examination is particularly useful<br />
in palpating a grossly distended rumen, caecal dilatation<br />
and torsion, gut tie, and intestinal intussusception.<br />
The gas or fluid content <strong>of</strong> the abnormal viscus<br />
can be assessed. Indicators <strong>of</strong> peritonitis such as adhesions<br />
and a sandy grating sensation may be palpable.<br />
The quantity and composition <strong>of</strong> the faeces can<br />
be assessed.<br />
Method<br />
<strong>Examination</strong> per rectum requires care and patience<br />
with good restraint. It is best performed in the<br />
standing animal, although it is possible in the recumbent<br />
animal. In the recumbent animal the<br />
abdominal contents are displaced caudally, which<br />
makes palpation difficult unless the animal is placed<br />
in lateral recumbency. The safety <strong>of</strong> the operator<br />
should be considered if the animal is likely to<br />
rise. Fingernails should be short and well manicured;<br />
watches and rings should be removed; the gloved<br />
hand should be well lubricated. The tail has to be elevated<br />
to enable access to the rectum. It is likely that a<br />
rectal prolapse will have been detected before this<br />
point in the examination, either by observation or by<br />
the presence <strong>of</strong> tenesmus. However, on raising the<br />
tail a rectal prolapse will present with inflamed oedematous<br />
rectal mucosa protruding through the anus.<br />
The rectal examination proceeds by coning the fingers<br />
and gently pushing through the anal sphincter.<br />
Sometimes a small rotatory movement <strong>of</strong> the hand<br />
helps to facilitate entry. Palpation is performed with<br />
the open hand. If the rectum is full <strong>of</strong> faeces, manual<br />
evacuation <strong>of</strong> the faeces will be required. This must<br />
be done slowly and carefully to avoid the entry <strong>of</strong> air<br />
into the rectum. If air is allowed to enter the rectum<br />
the wall may balloon and make palpation <strong>of</strong> internal<br />
structures impossible. Gentle backwards stroking <strong>of</strong><br />
the ventral rectal mucosa may facilitate a peristaltic<br />
wave which may decompress the rectum so that<br />
palpation can continue. Peristaltic waves should be<br />
allowed to pass over the arm and active palpation<br />
suspended. If blood is seen on the glove, bleeding <strong>of</strong><br />
the mucosa may be suggested and the examination<br />
should be curtailed.<br />
The rectal examination<br />
The contents <strong>of</strong> the posterior abdomen should be<br />
checked in a set order to avoid missing any organ. The<br />
examination area may be divided into quadrants or<br />
conducted by body system. Alternatively, a combination<br />
<strong>of</strong> both approaches can be used. Each quadrant<br />
examination area is palpated and the organs present<br />
assesed or noted if unexpectedly absent. Under normal<br />
conditions the omasum, abomasum and liver<br />
cannot be felt. Parts <strong>of</strong> the small intestine and large<br />
intestine can be felt but are not discrete structures.<br />
In the normal animal it is possible to palpate the<br />
caudal surface <strong>of</strong> the dorsal sac <strong>of</strong> the rumen to the<br />
left <strong>of</strong> the pelvic brim. The degree <strong>of</strong> filling and nature<br />
<strong>of</strong> the contents should be assessed. In vagal indigestion<br />
the rumen is <strong>of</strong>ten packed with undigested<br />
fibre. The absence <strong>of</strong> the dorsal sac usually indicates<br />
a collapsed dorsal sac. A left displaced abomasum<br />
cannot be felt per rectum unless the gas-filled viscus<br />
is displaced very high and caudal in the left flank,<br />
which is exceptional. A right displaced and/or<br />
dilated abomasum may be felt at arm’s length laterally<br />
on the right as a tense gas-filled viscus. Intussusceptions<br />
usually occur at the ileocaecal junction. The<br />
invagination <strong>of</strong> one part <strong>of</strong> the intestine into another<br />
can sometimes be felt as a large hard sausage-like<br />
structure on the right. A distended caecum can be<br />
palpated on the right as a tense gas-filled sausageshaped<br />
balloon with the blind end caudally. If displacement<br />
has also occurred, the blind end <strong>of</strong> the<br />
caecum may have been rotated cranially out <strong>of</strong> reach.<br />
In gut tie a tense band may be felt ensnaring the intestine<br />
on the right side. This is caused by peritoneal<br />
adhesion <strong>of</strong> the remnant <strong>of</strong> the spermatic cord following<br />
castration. Abdominal masses, such as the<br />
large focal fat deposits in fat necrosis, may be palpated.<br />
Thickening <strong>of</strong> the intestine may be detected in<br />
Johne’s disease, but this is highly subjective. Nonspecific<br />
referred pain or focal pain responses may be<br />
elicited on rectal examination. Referred pain may<br />
arise from a peritonitis or traumatic reticulitis. Focal<br />
pain may be provoked on palpation <strong>of</strong> an intussus-<br />
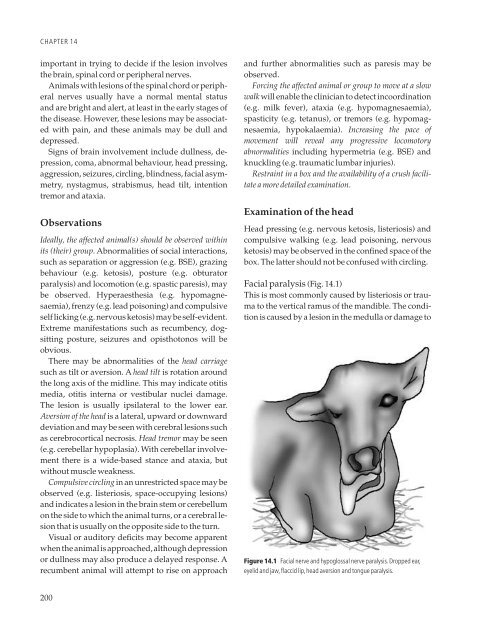
97