Global Tuberculosis Control 2010 - Florida Department of Health
Global Tuberculosis Control 2010 - Florida Department of Health
Global Tuberculosis Control 2010 - Florida Department of Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
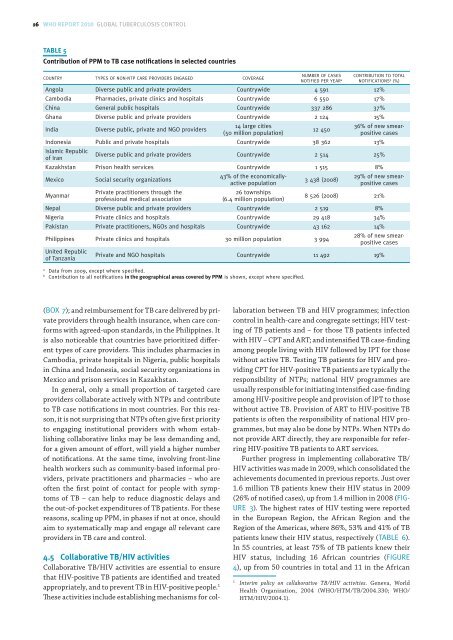
(); and reimbursement for TB care delivered by private<br />
providers through health insurance, when care conforms<br />
with agreed-upon standards, in the Philippines. It<br />
is also noticeable that countries have prioritized different<br />
types <strong>of</strong> care providers. This includes pharmacies in<br />
Cambodia, private hospitals in Nigeria, public hospitals<br />
in China and Indonesia, social security organizations in<br />
Mexico and prison services in Kazakhstan.<br />
In general, only a small proportion <strong>of</strong> targeted care<br />
providers collaborate actively with NTPs and contribute<br />
to TB case notifications in most countries. For this reason,<br />
it is not surprising that NTPs <strong>of</strong>ten give first priority<br />
to engaging institutional providers with whom establishing<br />
collaborative links may be less demanding and,<br />
for a given amount <strong>of</strong> effort, will yield a higher number<br />
<strong>of</strong> notifications. At the same time, involving front-line<br />
health workers such as community-based informal providers,<br />
private practitioners and pharmacies – who are<br />
<strong>of</strong>ten the first point <strong>of</strong> contact for people with symptoms<br />
<strong>of</strong> TB – can help to reduce diagnostic delays and<br />
the out-<strong>of</strong>-pocket expenditures <strong>of</strong> TB patients. For these<br />
reasons, scaling up PPM, in phases if not at once, should<br />
aim to systematically map and engage all relevant care<br />
providers in TB care and control.<br />
<br />
Collaborative TB/HIV activities are essential to ensure<br />
that HIV-positive TB patients are identified and treated<br />
appropriately, and to prevent TB in HIV-positive people. 1<br />
These activities include establishing mechanisms for col-<br />
laboration between TB and HIV programmes; infection<br />
control in health-care and congregate settings; HIV testing<br />
<strong>of</strong> TB patients and – for those TB patients infected<br />
with HIV – CPT and ART; and intensified TB case-finding<br />
among people living with HIV followed by IPT for those<br />
without active TB. Testing TB patients for HIV and providing<br />
CPT for HIV-positive TB patients are typically the<br />
responsibility <strong>of</strong> NTPs; national HIV programmes are<br />
usually responsible for initiating intensified case-finding<br />
among HIV-positive people and provision <strong>of</strong> IPT to those<br />
without active TB. Provision <strong>of</strong> ART to HIV-positive TB<br />
patients is <strong>of</strong>ten the responsibility <strong>of</strong> national HIV programmes,<br />
but may also be done by NTPs. When NTPs do<br />
not provide ART directly, they are responsible for referring<br />
HIV-positive TB patients to ART services.<br />
Further progress in implementing collaborative TB/<br />
HIV activities was made in 2009, which consolidated the<br />
achievements documented in previous reports. Just over<br />
1.6 million TB patients knew their HIV status in 2009<br />
(26% <strong>of</strong> notified cases), up from 1.4 million in 2008 (<br />
). The highest rates <strong>of</strong> HIV testing were reported<br />
in the European Region, the African Region and the<br />
Region <strong>of</strong> the Americas, where 86%, 53% and 41% <strong>of</strong> TB<br />
patients knew their HIV status, respectively ().<br />
In 55 countries, at least 75% <strong>of</strong> TB patients knew their<br />
HIV status, including 16 African countries (<br />
), up from 50 countries in total and 11 in the African<br />
1<br />
Interim policy on collaborative TB/HIV activities. Geneva, World<br />
<strong>Health</strong> Organization, 2004 (WHO/HTM/TB/2004.330; WHO/<br />
HTM/HIV/2004.1).