2013 Employee Benefits Guidebook - Administration Home
2013 Employee Benefits Guidebook - Administration Home
2013 Employee Benefits Guidebook - Administration Home

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
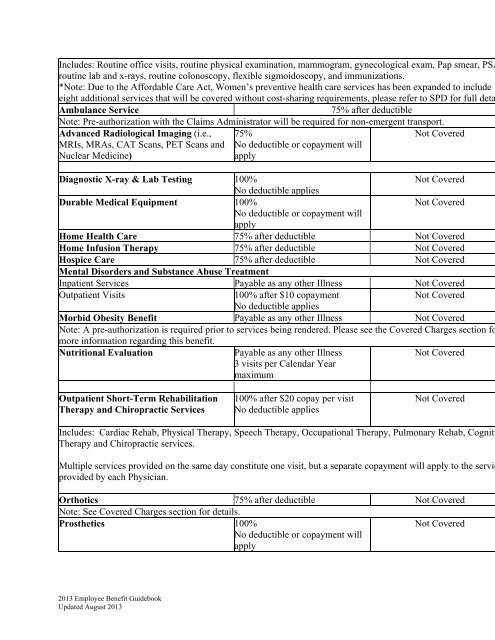
Includes: Routine office visits, routine physical examination, mammogram, gynecological exam, Pap smear, PSA<br />
eight additional services that will be covered without cost-sharing requirements, please refer to SPD for full deta<br />
routine lab and x-rays, routine colonoscopy, flexible sigmoidoscopy, and immunizations.<br />
*Note: Due to the Affordable Care Act, Women’s preventive health care services has been expanded to include<br />
Ambulance Service<br />
75% after deductible<br />
Note: Pre-authorization with the Claims Administrator will be required for non-emergent transport.<br />
Advanced Radiological Imaging (i.e.,<br />
MRIs, MRAs, CAT Scans, PET Scans and<br />
Nuclear Medicine)<br />
75%<br />
No deductible or copayment will<br />
apply<br />
Not Covered<br />
Note: A pre-authorization is required prior to services being rendered. Please see the Covered Charges section fo<br />
Diagnostic X-ray & Lab Testing 100%<br />
Not Covered<br />
No deductible applies<br />
Durable Medical Equipment 100%<br />
Not Covered<br />
No deductible or copayment will<br />
apply<br />
<strong>Home</strong> Health Care 75% after deductible Not Covered<br />
<strong>Home</strong> Infusion Therapy 75% after deductible Not Covered<br />
Hospice Care 75% after deductible Not Covered<br />
Mental Disorders and Substance Abuse Treatment<br />
Inpatient Services Payable as any other Illness Not Covered<br />
Outpatient Visits<br />
100% after $10 copayment<br />
Not Covered<br />
No deductible applies<br />
Morbid Obesity Benefit Payable as any other Illness Not Covered<br />
more information regarding this benefit.<br />
Nutritional Evaluation<br />
Payable as any other Illness<br />
3 visits per Calendar Year<br />
maximum<br />
Not Covered<br />
Outpatient Short-Term Rehabilitation<br />
Therapy and Chiropractic Services<br />
100% after $20 copay per visit<br />
No deductible applies<br />
Not Covered<br />
Includes: Cardiac Rehab, Physical Therapy, Speech Therapy, Occupational Therapy, Pulmonary Rehab, Cogniti<br />
Therapy and Chiropractic services.<br />
Multiple services provided on the same day constitute one visit, but a separate copayment will apply to the servic<br />
provided by each Physician.<br />
Orthotics 75% after deductible Not Covered<br />
Note: See Covered Charges section for details.<br />
Prosthetics 100%<br />
No deductible or copayment will<br />
apply<br />
Not Covered<br />
<strong>2013</strong> <strong>Employee</strong> Benefit <strong>Guidebook</strong><br />
Updated August <strong>2013</strong>