

Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
228<br />
Blunt and Penetrating Thoracic Trauma: Management Strategy and Short-Term Outcome<br />
<strong>September</strong> <strong>2009</strong><br />
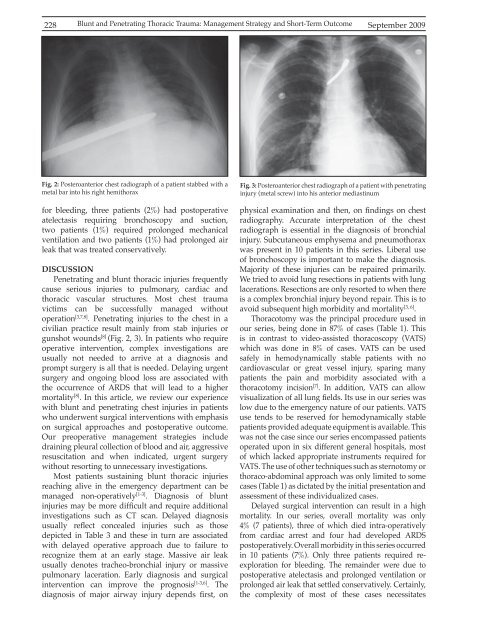
Fig. 2: Posteroanterior chest radiograph of a patient stabbed with a<br />
metal bar into his right hemithorax<br />
for bleeding, three patients (2%) had postoperative<br />
atelectasis requiring bronchoscopy and suction,<br />
two patients (1%) required prolonged mechanical<br />
ventilation and two patients (1%) had prolonged air<br />
leak that was treated conservatively.<br />
DISCUSSION<br />
Penetrating and blunt thoracic injuries frequently<br />
cause serious injuries to pulmonary, cardiac and<br />
thoracic vascular structures. Most chest trauma<br />
victims can be successfully managed without<br />
operation [3,7,8] . Penetrating injuries to the chest in a<br />
civilian practice result mainly from stab injuries or<br />
gunshot wounds [8] (Fig. 2, 3). In patients who require<br />
operative intervention, complex investigations are<br />
usually not needed to arrive at a diagnosis and<br />
prompt surgery is all that is needed. Delaying urgent<br />
surgery and ongoing blood loss are associated with<br />
the occurrence of ARDS that will lead to a higher<br />
mortality [8] . In this article, we review our experience<br />
with blunt and penetrating chest injuries in patients<br />
who underwent surgical interventions with emphasis<br />
on surgical approaches and postoperative outcome.<br />
Our preoperative management strategies include<br />
draining pleural collection of blood and air, aggressive<br />
resuscitation and when indicated, urgent surgery<br />
without resorting to unnecessary investigations.<br />
Most patients sustaining blunt thoracic injuries<br />
reaching alive in the emergency department can be<br />
managed non-operatively [1-3] . Diagnosis of blunt<br />
injuries may be more difficult and require additional<br />
investigations such as CT scan. Delayed diagnosis<br />
usually reflect concealed injuries such as those<br />
depicted in Table 3 and these in turn are associated<br />
with delayed operative approach due to failure to<br />
recognize them at an early stage. Massive air leak<br />
usually denotes tracheo-bronchial injury or massive<br />
pulmonary laceration. Early diagnosis and surgical<br />
intervention can improve the prognosis [1-3,6] . The<br />
diagnosis of major airway injury depends first, on<br />
Fig. 3: Posteroanterior chest radiograph of a patient with penetrating<br />
injury (metal screw) into his anterior mediastinum<br />
physical examination and then, on findings on chest<br />
radiography. Accurate interpretation of the chest<br />
radiograph is essential in the diagnosis of bronchial<br />
injury. Subcutaneous emphysema and pneumothorax<br />
was present in 10 patients in this series. Liberal use<br />
of bronchoscopy is important to make the diagnosis.<br />
Majority of these injuries can be repaired primarily.<br />
We tried to avoid lung resections in patients with lung<br />
lacerations. Resections are only resorted to when there<br />
is a complex bronchial injury beyond repair. This is to<br />
avoid subsequent high morbidity and mortality [3, 6] .<br />
Thoracotomy was the principal procedure used in<br />
our series, being done in 87% of cases (Table 1). This<br />
is in contrast to video-assisted thoracoscopy (VATS)<br />
which was done in 8% of cases. VATS can be used<br />
safely in hemodynamically stable patients with no<br />
cardiovascular or great vessel injury, sparing many<br />
patients the pain and morbidity associated with a<br />
thoracotomy incision [7] . In addition, VATS can allow<br />
visualization of all lung fields. Its use in our series was<br />
low due to the emergency nature of our patients. VATS<br />
use tends to be reserved for hemodynamically stable<br />
patients provided adequate equipment is available. This<br />
was not the case since our series encompassed patients<br />
operated upon in six different general hospitals, most<br />
of which lacked appropriate instruments required for<br />
VATS. The use of other techniques such as sternotomy or<br />
thoraco-abdominal approach was only limited to some<br />
cases (Table 1) as dictated by the initial presentation and<br />
assessment of these individualized cases.<br />
Delayed surgical intervention can result in a high<br />
mortality. In our series, overall mortality was only<br />
4% (7 patients), three of which died intra-operatively<br />
from cardiac arrest and four had developed ARDS<br />
postoperatively. Overall morbidity in this series occurred<br />
in 10 patients (7%). Only three patients required reexploration<br />
for bleeding. The remainder were due to<br />
postoperative atelectasis and prolonged ventilation or<br />
prolonged air leak that settled conservatively. Certainly,<br />
the complexity of most of these cases necessitates













