

Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>September</strong> <strong>2009</strong><br />
KUWAIT MEDICAL JOURNAL 237<br />
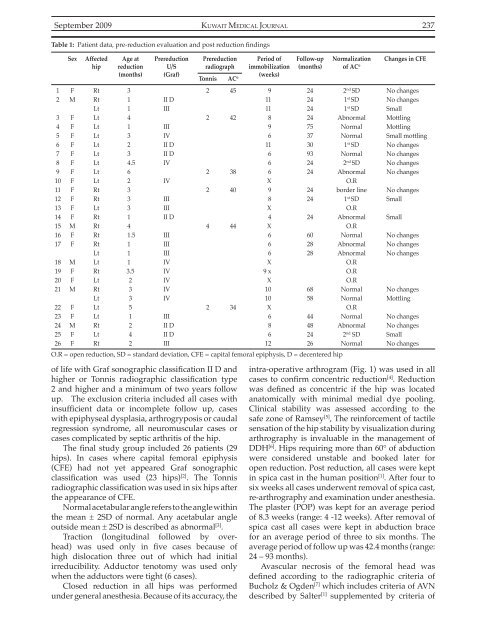
Table 1: Patient data, pre-reduction evaluation and post reduction findings<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
8<br />
9<br />
10<br />
11<br />
12<br />
13<br />
14<br />
15<br />
16<br />
17<br />
18<br />
19<br />
20<br />
21<br />
22<br />
23<br />
24<br />
25<br />
26<br />
Sex<br />
F<br />
M<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
F<br />
M<br />
F<br />
F<br />
M<br />
F<br />
F<br />
M<br />
F<br />
F<br />
M<br />
F<br />
F<br />
Affected<br />
hip<br />
Rt<br />
Rt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Lt<br />
Rt<br />
Rt<br />
Lt<br />
Rt<br />
Rt<br />
Rt<br />
Rt<br />
Lt<br />
Lt<br />
Rt<br />
Lt<br />
Rt<br />
Lt<br />
Lt<br />
Lt<br />
Rt<br />
Lt<br />
Rt<br />
Age at<br />
reduction<br />
(months)<br />
3<br />
1<br />
1<br />
4<br />
1<br />
3<br />
2<br />
3<br />
4.5<br />
6<br />
2<br />
3<br />
3<br />
3<br />
1<br />
4<br />
1.5<br />
1<br />
1<br />
1<br />
3.5<br />
2<br />
3<br />
3<br />
5<br />
1<br />
2<br />
4<br />
2<br />
Prereduction<br />
U/S<br />
(Graf)<br />
II D<br />
III<br />
III<br />
IV<br />
II D<br />
II D<br />
IV<br />
IV<br />
III<br />
III<br />
II D<br />
III<br />
III<br />
III<br />
IV<br />
IV<br />
IV<br />
IV<br />
IV<br />
III<br />
II D<br />
II D<br />
III<br />
Prereduction<br />
radiograph<br />
Tonnis<br />
AC o<br />
Period of<br />
immobilization<br />
(weeks)<br />
Follow-up<br />
(months)<br />
O.R = open reduction, SD = standard deviation, CFE = capital femoral epiphysis, D = decentered hip<br />
2<br />
2<br />
2<br />
2<br />
4<br />
2<br />
45<br />
42<br />
38<br />
40<br />
44<br />
34<br />
9<br />
11<br />
11<br />
8<br />
9<br />
6<br />
11<br />
6<br />
6<br />
6<br />
X<br />
9<br />
8<br />
X<br />
4<br />
X<br />
6<br />
6<br />
6<br />
X<br />
9 x<br />
X<br />
10<br />
10<br />
X<br />
6<br />
8<br />
6<br />
12<br />
24<br />
24<br />
24<br />
24<br />
75<br />
37<br />
30<br />
93<br />
24<br />
24<br />
24<br />
24<br />
24<br />
60<br />
28<br />
28<br />
68<br />
58<br />
44<br />
48<br />
24<br />
26<br />
Normalization<br />
of AC o<br />
2 nd SD<br />
1 st SD<br />
1 st SD<br />
Abnormal<br />
Normal<br />
Normal<br />
1 st SD<br />
Normal<br />
2 nd SD<br />
Abnormal<br />
O.R<br />
border line<br />
1 st SD<br />
O.R<br />
Abnormal<br />
O.R<br />
Normal<br />
Abnormal<br />
Abnormal<br />
O.R<br />
O.R<br />
O.R<br />
Normal<br />
Normal<br />
O.R<br />
Normal<br />
Abnormal<br />
2 nd SD<br />
Normal<br />
Changes in CFE<br />
No changes<br />
No changes<br />
Small<br />
Mottling<br />
Mottling<br />
Small mottling<br />
No changes<br />
No changes<br />
No changes<br />
No changes<br />
No changes<br />
Small<br />
Small<br />
No changes<br />
No changes<br />
No changes<br />
No changes<br />
Mottling<br />
No changes<br />
No changes<br />
Small<br />
No changes<br />
of life with Graf sonographic classification II D and<br />
higher or Tonnis radiographic classification type<br />
2 and higher and a minimum of two years follow<br />
up. The exclusion criteria included all cases with<br />
insufficient data or incomplete follow up, cases<br />
with epiphyseal dysplasia, arthrogryposis or caudal<br />
regression syndrome, all neuromuscular cases or<br />
cases complicated by septic arthritis of the hip.<br />
The final study group included 26 patients (29<br />
hips). In cases where capital femoral epiphysis<br />
(CFE) had not yet appeared Graf sonographic<br />
classification was used (23 hips) [2] . The Tonnis<br />
radiographic classification was used in six hips after<br />
the appearance of CFE.<br />
Normal acetabular angle refers to the angle within<br />
the mean ± 2SD of normal. Any acetabular angle<br />
outside mean ± 2SD is described as abnormal [3] .<br />
Traction (longitudinal followed by overhead)<br />
was used only in five cases because of<br />
high dislocation three out of which had initial<br />
irreducibility. Adductor tenotomy was used only<br />
when the adductors were tight (6 cases).<br />
Closed reduction in all hips was performed<br />
under general anesthesia. Because of its accuracy, the<br />
intra-operative arthrogram (Fig. 1) was used in all<br />
cases to confirm concentric reduction [4] . Reduction<br />
was defined as concentric if the hip was located<br />
anatomically with minimal medial dye pooling.<br />
Clinical stability was assessed according to the<br />
safe zone of Ramsey [5] , The reinforcement of tactile<br />
sensation of the hip stability by visualization during<br />
arthrography is invaluable in the management of<br />
DDH [6] . Hips requiring more than 60° of abduction<br />
were considered unstable and booked later for<br />
open reduction. Post reduction, all cases were kept<br />
in spica cast in the human position [1] . After four to<br />
six weeks all cases underwent removal of spica cast,<br />
re-arthrography and examination under anesthesia.<br />
The plaster (POP) was kept for an average period<br />
of 8.3 weeks (range: 4 -12 weeks). After removal of<br />
spica cast all cases were kept in abduction brace<br />
for an average period of three to six months. The<br />
average period of follow up was 42.4 months (range:<br />
24 – 93 months).<br />
Avascular necrosis of the femoral head was<br />
defined according to the radiographic criteria of<br />
Bucholz & Ogden [7] which includes criteria of AVN<br />
described by Salter [1] supplemented by criteria of













