

Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw
Vol 41 # 3 September 2009 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
252<br />
Neurosarcoidosis as a First Presentation of Systemic Sarcoidosis: Case Report<br />
<strong>September</strong> <strong>2009</strong><br />
Fig. 5: Photomicrograph of a lymph node showing extensive<br />
hyalinization with little residual lymphoid tissue. In addition,<br />
there is a non-caseating granuloma consistent with sarcoidosis.<br />
included CXR, brain MRI, and gradual reduction of<br />
the steroid dose.<br />
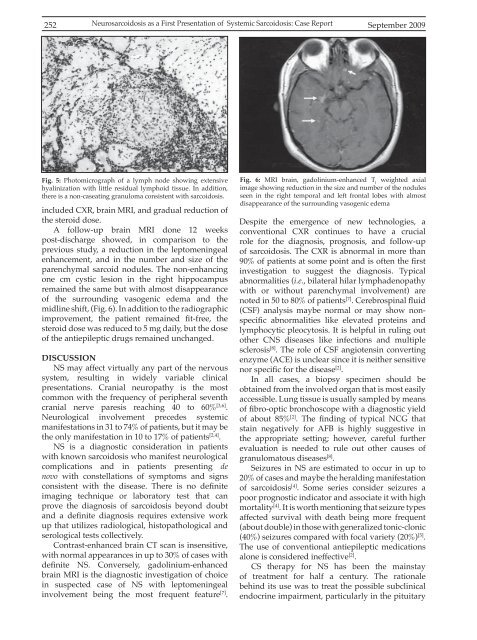
A follow-up brain MRI done 12 weeks<br />
post-discharge showed, in comparison to the<br />
previous study, a reduction in the leptomeningeal<br />
enhancement, and in the number and size of the<br />
parenchymal sarcoid nodules. The non-enhancing<br />
one cm cystic lesion in the right hippocampus<br />
remained the same but with almost disappearance<br />
of the surrounding vasogenic edema and the<br />
midline shift, (Fig. 6). In addition to the radiographic<br />
improvement, the patient remained fit-free, the<br />
steroid dose was reduced to 5 mg daily, but the dose<br />
of the antiepileptic drugs remained unchanged.<br />
DISCUSSION<br />
NS may affect virtually any part of the nervous<br />
system, resulting in widely variable clinical<br />
presentations. Cranial neuropathy is the most<br />
common with the frequency of peripheral seventh<br />
cranial nerve paresis reaching 40 to 60% [3,6] .<br />
Neurological involvement precedes systemic<br />
manifestations in 31 to 74% of patients, but it may be<br />
the only manifestation in 10 to 17% of patients [2,4] .<br />
NS is a diagnostic consideration in patients<br />
with known sarcoidosis who manifest neurological<br />
complications and in patients presenting de<br />
novo with constellations of symptoms and signs<br />
consistent with the disease. There is no definite<br />
imaging technique or laboratory test that can<br />
prove the diagnosis of sarcoidosis beyond doubt<br />
and a definite diagnosis requires extensive work<br />
up that utilizes radiological, histopathological and<br />
serological tests collectively.<br />
Contrast-enhanced brain CT scan is insensitive,<br />
with normal appearances in up to 30% of cases with<br />
definite NS. Conversely, gadolinium-enhanced<br />
brain MRI is the diagnostic investigation of choice<br />
in suspected case of NS with leptomeningeal<br />
involvement being the most frequent feature [7] .<br />
Fig. 6: MRI brain, gadolinium-enhanced T l<br />
weighted axial<br />
image showing reduction in the size and number of the nodules<br />
seen in the right temporal and left frontal lobes with almost<br />
disappearance of the surrounding vasogenic edema<br />
Despite the emergence of new technologies, a<br />
conventional CXR continues to have a crucial<br />
role for the diagnosis, prognosis, and follow-up<br />
of sarcoidosis. The CXR is abnormal in more than<br />
90% of patients at some point and is often the first<br />
investigation to suggest the diagnosis. Typical<br />
abnormalities (i.e., bilateral hilar lymphadenopathy<br />
with or without parenchymal involvement) are<br />
noted in 50 to 80% of patients [7] . Cerebrospinal fluid<br />
(CSF) analysis maybe normal or may show nonspecific<br />
abnormalities like elevated proteins and<br />
lymphocytic pleocytosis. It is helpful in ruling out<br />
other CNS diseases like infections and multiple<br />
sclerosis [8] . The role of CSF angiotensin converting<br />
enzyme (ACE) is unclear since it is neither sensitive<br />
nor specific for the disease [2] .<br />
In all cases, a biopsy specimen should be<br />
obtained from the involved <strong>org</strong>an that is most easily<br />
accessible. Lung tissue is usually sampled by means<br />
of fibro-optic bronchoscope with a diagnostic yield<br />
of about 85% [2] . The finding of typical NCG that<br />
stain negatively for AFB is highly suggestive in<br />
the appropriate setting; however, careful further<br />
evaluation is needed to rule out other causes of<br />
granulomatous diseases [8] .<br />
Seizures in NS are estimated to occur in up to<br />
20% of cases and maybe the heralding manifestation<br />
of sarcoidosis [4] . Some series consider seizures a<br />
poor prognostic indicator and associate it with high<br />
mortality [4] . It is worth mentioning that seizure types<br />
affected survival with death being more frequent<br />
(about double) in those with generalized tonic-clonic<br />
(40%) seizures compared with focal variety (20%) [5] .<br />
The use of conventional antiepileptic medications<br />
alone is considered ineffective [2] .<br />
CS therapy for NS has been the mainstay<br />
of treatment for half a century. The rationale<br />
behind its use was to treat the possible subclinical<br />
endocrine impairment, particularly in the pituitary













