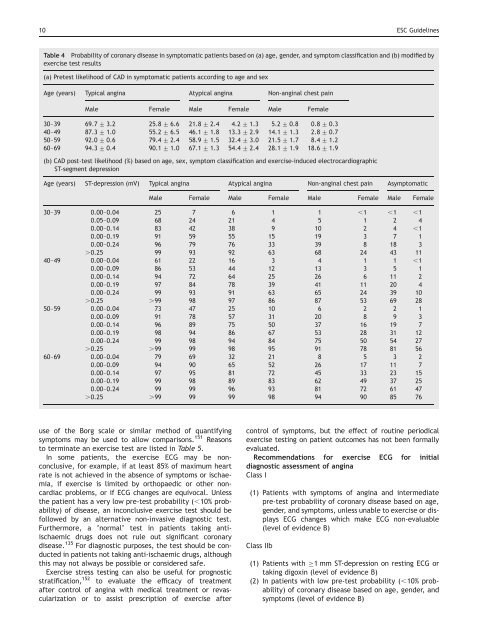
10 ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g>Table 4 Probability <strong>of</strong> cor<strong>on</strong>ary disease in symptomatic patients based <strong>on</strong> (a) age, gender, and symptom classificati<strong>on</strong> and (b) modified byexercise test results(a) Pretest likelihood <strong>of</strong> CAD in symptomatic patients according to age and sexAge (years) Typical angina Atypical angina N<strong>on</strong>-anginal chest painMale Female Male Female Male Female30–39 69.7 + 3.2 25.8 + 6.6 21.8 + 2.4 4.2 + 1.3 5.2 + 0.8 0.8 + 0.340–49 87.3 + 1.0 55.2 + 6.5 46.1 + 1.8 13.3 + 2.9 14.1 + 1.3 2.8 + 0.750–59 92.0 + 0.6 79.4 + 2.4 58.9 + 1.5 32.4 + 3.0 21.5 + 1.7 8.4 + 1.260–69 94.3 + 0.4 90.1 + 1.0 67.1 + 1.3 54.4 + 2.4 28.1 + 1.9 18.6 + 1.9(b) CAD post-test likelihood (%) based <strong>on</strong> age, sex, symptom classificati<strong>on</strong> and exercise-induced electrocardiographicST-segment depressi<strong>on</strong>Age (years) ST-depressi<strong>on</strong> (mV) Typical angina Atypical angina N<strong>on</strong>-anginal chest pain AsymptomaticMale Female Male Female Male Female Male Female30–39 0.00–0.04 25 7 6 1 1 ,1 ,1 ,10.05–0.09 68 24 21 4 5 1 2 40.00–0.14 83 42 38 9 10 2 4 ,10.00–0.19 91 59 55 15 19 3 7 10.00–0.24 96 79 76 33 39 8 18 3.0.25 99 93 92 63 68 24 43 1140–49 0.00–0.04 61 22 16 3 4 1 1 ,10.00–0.09 86 53 44 12 13 3 5 10.00–0.14 94 72 64 25 26 6 11 20.00–0.19 97 84 78 39 41 11 20 40.00–0.24 99 93 91 63 65 24 39 10.0.25 .99 98 97 86 87 53 69 2850–59 0.00–0.04 73 47 25 10 6 2 2 10.00–0.09 91 78 57 31 20 8 9 30.00–0.14 96 89 75 50 37 16 19 70.00–0.19 98 94 86 67 53 28 31 120.00–0.24 99 98 94 84 75 50 54 27.0.25 .99 99 98 95 91 78 81 5660–69 0.00–0.04 79 69 32 21 8 5 3 20.00–0.09 94 90 65 52 26 17 11 70.00–0.14 97 95 81 72 45 33 23 150.00–0.19 99 98 89 83 62 49 37 250.00–0.24 99 99 96 93 81 72 61 47.0.25 .99 99 99 98 94 90 85 76use <strong>of</strong> <strong>the</strong> Borg scale or similar method <strong>of</strong> quantifyingsymptoms may be used to allow comparis<strong>on</strong>s. 151 Reas<strong>on</strong>sto terminate an exercise test are listed in Table 5.In some patients, <strong>the</strong> exercise ECG may be n<strong>on</strong>c<strong>on</strong>clusive,for example, if at least 85% <strong>of</strong> maximum heartrate is not achieved in <strong>the</strong> absence <strong>of</strong> symptoms or ischaemia,if exercise is limited by orthopaedic or o<strong>the</strong>r n<strong>on</strong>cardiacproblems, or if ECG changes are equivocal. Unless<strong>the</strong> patient has a very low pre-test probability (,10% probability)<strong>of</strong> disease, an inc<strong>on</strong>clusive exercise test should befollowed by an alternative n<strong>on</strong>-invasive diagnostic test.Fur<strong>the</strong>rmore, a ’normal’ test in patients taking antiischaemicdrugs does not rule out significant cor<strong>on</strong>arydisease. 135 For diagnostic purposes, <strong>the</strong> test should be c<strong>on</strong>ductedin patients not taking anti-ischaemic drugs, althoughthis may not always be possible or c<strong>on</strong>sidered safe.Exercise stress testing can also be useful for prognosticstratificati<strong>on</strong>, 152 to evaluate <strong>the</strong> efficacy <strong>of</strong> treatmentafter c<strong>on</strong>trol <strong>of</strong> angina with medical treatment or revascularizati<strong>on</strong>or to assist prescripti<strong>on</strong> <strong>of</strong> exercise afterc<strong>on</strong>trol <strong>of</strong> symptoms, but <strong>the</strong> effect <strong>of</strong> routine periodicalexercise testing <strong>on</strong> patient outcomes has not been formallyevaluated.Recommendati<strong>on</strong>s for exercise ECG for initialdiagnostic assessment <strong>of</strong> anginaClass I(1) Patients with symptoms <strong>of</strong> angina and intermediatepre-test probability <strong>of</strong> cor<strong>on</strong>ary disease based <strong>on</strong> age,gender, and symptoms, unless unable to exercise or displaysECG changes which make ECG n<strong>on</strong>-evaluable(level <strong>of</strong> evidence B)Class IIb(1) Patients with 1 mm ST-depressi<strong>on</strong> <strong>on</strong> resting ECG ortaking digoxin (level <strong>of</strong> evidence B)(2) In patients with low pre-test probability (,10% probability)<strong>of</strong> cor<strong>on</strong>ary disease based <strong>on</strong> age, gender, andsymptoms (level <strong>of</strong> evidence B)
ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g> 11Table 5Reas<strong>on</strong>s to terminate <strong>the</strong> exercise stress testThe exercise stress test is terminated for <strong>on</strong>e <strong>of</strong> <strong>the</strong> followingreas<strong>on</strong>s† Symptom limitati<strong>on</strong>, e.g. pain, fatigue, dyspnoea, andclaudicati<strong>on</strong>† Combinati<strong>on</strong> <strong>of</strong> symptoms such as pain with significantST-changes† Safety reas<strong>on</strong>s such as <strong>the</strong> followingMarked ST-depressi<strong>on</strong> (.2 mm ST-depressi<strong>on</strong> can betaken as a relative indicati<strong>on</strong> for terminati<strong>on</strong> and4 mm as an absolute indicati<strong>on</strong> to stop <strong>the</strong> test)ST-elevati<strong>on</strong> 1 mmSignificant arrhythmiaSustained fall in systolic blood pressure .10 mmHgMarked hypertensi<strong>on</strong> (.250 mmHg systolic or .115 mmHgdiastolic)† Achievement <strong>of</strong> maximum predicted heart rate may also bea reas<strong>on</strong> to terminate <strong>the</strong> test in patients with excellentexercise tolerance who are not tired and at <strong>the</strong> discreti<strong>on</strong><strong>of</strong> <strong>the</strong> supervising physicianRecommendati<strong>on</strong>s for exercise ECG for routinere-assessment in patients with chr<strong>on</strong>ic stable anginaClass IIb(1) Routine periodic exercise ECG in <strong>the</strong> absence <strong>of</strong> clinicalchange (level <strong>of</strong> evidence C)Stress testing in combinati<strong>on</strong> with imagingThe most well established stress imaging techniques areechocardiography and perfusi<strong>on</strong> scintigraphy. Both may beused in combinati<strong>on</strong> with ei<strong>the</strong>r exercise stress or pharmacologicalstress, and many studies have been c<strong>on</strong>ductedevaluating <strong>the</strong>ir use in both prognostic and diagnosticassessment over <strong>the</strong> past two decades or more. Novelstress imaging techniques also include stress MRI, which,for logistical reas<strong>on</strong>s, is most frequently performed usingpharmacological ra<strong>the</strong>r than exercise stress.Stress imaging techniques have several advantages overc<strong>on</strong>venti<strong>on</strong>al exercise ECG testing including superior diagnosticperformance (Table 6) for <strong>the</strong> detecti<strong>on</strong> <strong>of</strong> obstructivecor<strong>on</strong>ary disease, <strong>the</strong> ability to quantify and localizeareas <strong>of</strong> ischaemia, and <strong>the</strong> ability to provide diagnosticinformati<strong>on</strong> in <strong>the</strong> presence <strong>of</strong> resting ECG abnormalitiesor inability <strong>of</strong> <strong>the</strong> patient to exercise. Stress imaging techniquesare <strong>of</strong>ten preferred in patients with previous PCI orcor<strong>on</strong>ary artery bypass grafting (CABG) because <strong>of</strong> itssuperior ability to localize ischaemia. In patients withangiographically c<strong>on</strong>firmed intermediate cor<strong>on</strong>ary lesi<strong>on</strong>s,evidence <strong>of</strong> anatomically appropriate ischaemia is predictive<strong>of</strong> future events, whereas a negative stress imagingtest can be used to define patients with a low cardiac riskwho can be reassured. 153Exercise testing with echocardiography. Exercise stressechocardiography has been developed as an alternative to‘classical’ exercise testing with ECG and as an additi<strong>on</strong>alinvestigati<strong>on</strong> to establish <strong>the</strong> presence or locati<strong>on</strong> andextent <strong>of</strong> myocardial ischaemia during stress. A restingechocardiogram is acquired before a symptom-limitedexercise test is performed, most frequently using a bicycleergometer, with fur<strong>the</strong>r images acquired where possibleTable 6 Summary <strong>of</strong> test characteristics for investigati<strong>on</strong>s usedin <strong>the</strong> diagnosis <strong>of</strong> stable anginaDiagnosis <strong>of</strong> CADSensitivity(%)Specificity(%)Exercise ECG 68 77Exercise echo 80–85 84–86Exercise myocardial perfusi<strong>on</strong> 85–90 70–75Dobutamine stress echo 40–100 62–100Vasodilator stress echo 56–92 87–100Vasodilator stress myocardial perfusi<strong>on</strong> 83–94 64–90during each stage <strong>of</strong> exercise and at peak exercise. Thismay be technically challenging. 154 Reported sensitivitiesand specificities for <strong>the</strong> detecti<strong>on</strong> <strong>of</strong> significant cor<strong>on</strong>arydisease are within a similar range to those described forexercise stress perfusi<strong>on</strong> scintigraphy, sensitivity 53–93%specificity 70–100%, although stress echo tends to be lesssensitive and more specific than stress perfusi<strong>on</strong> scintigraphy.Depending <strong>on</strong> <strong>the</strong> meta-analysis, overall sensitivityand specificity <strong>of</strong> exercise echocardiography are reportedas 80–85 and 84–86%. 155–158 Recent improvements intechnology include improvements in endocardial borderdefiniti<strong>on</strong> with <strong>the</strong> use <strong>of</strong> c<strong>on</strong>trast agents to facilitateidentificati<strong>on</strong> <strong>of</strong> regi<strong>on</strong>al wall moti<strong>on</strong> abnormalities, and<strong>the</strong> use <strong>of</strong> injectable agents to image myocardialperfusi<strong>on</strong>. 159–161 Advances in tissue Doppler and strain rateimaging are even more promising.Tissue Doppler imaging allows regi<strong>on</strong>al quantificati<strong>on</strong> <strong>of</strong>myocardial moti<strong>on</strong> (velocity), and strain and strain rateimaging allow determinati<strong>on</strong> <strong>of</strong> regi<strong>on</strong>al deformati<strong>on</strong>,strain being <strong>the</strong> difference in velocity between adjacentregi<strong>on</strong>s and strain rate being <strong>the</strong> difference per unitlength. Tissue Doppler imaging 162,163 and strain rateimaging 164,165 have improved <strong>the</strong> diagnostic performance<strong>of</strong> stress echocardiography 166 improving <strong>the</strong> capability <strong>of</strong>echocardiography to detect ischaemia earlier in <strong>the</strong> ischaemiccascade. 166,167 Because <strong>of</strong> <strong>the</strong> quantitative nature <strong>of</strong><strong>the</strong> techniques, inter-operator variability and subjectivityin interpretati<strong>on</strong> <strong>of</strong> <strong>the</strong> results are also reduced. Hence,tissue Doppler and strain rate imaging are expected tocomplement current echocardiographic techniques forischaemia detecti<strong>on</strong> and improve <strong>the</strong> accuracy and reproducibility<strong>of</strong> stress echocardiography in <strong>the</strong> broader clinicalsetting. There is also some evidence that tissue Dopplerimaging may improve <strong>the</strong> prognostic utility <strong>of</strong> stressechocardiography. 168Exercise testing with myocardial perfusi<strong>on</strong> scintigraphy.201 Th and 99m Tc radiopharmaceuticals are <strong>the</strong> most comm<strong>on</strong>lyused tracers, employed with single phot<strong>on</strong> emissi<strong>on</strong>computed tomography (SPECT) in associati<strong>on</strong> with asymptom-limited exercise test <strong>on</strong> ei<strong>the</strong>r a bicycle ergometeror a treadmill. Although multiple-view planar images werefirst employed for myocardial perfusi<strong>on</strong> scintigraphy, <strong>the</strong>yhave been largely replaced by SPECT, which is superiorfrom <strong>the</strong> standpoint <strong>of</strong> localizati<strong>on</strong>, quantificati<strong>on</strong>, andimage quality. Regardless <strong>of</strong> <strong>the</strong> radiopharmaceutical used,SPECT perfusi<strong>on</strong> scintigraphy is performed to produce