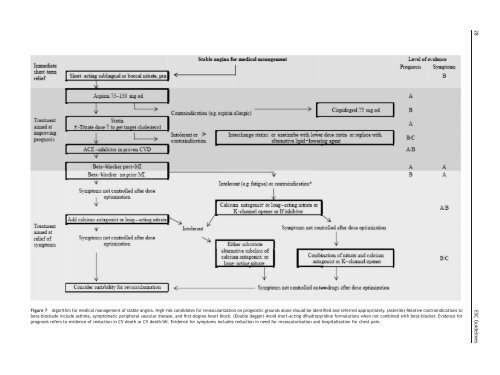
Figure 7 Algorithm for medical management <strong>of</strong> stable angina. High-risk candidates for revascularizati<strong>on</strong> <strong>on</strong> prognostic grounds al<strong>on</strong>e should be identified and referred appropriately. (Asterisk) Relative c<strong>on</strong>traindicati<strong>on</strong>s tobeta-blockade include asthma, symptomatic peripheral vascular disease, and first-degree heart block. (Double dagger) Avoid short-acting dihydropyridine formulati<strong>on</strong>s when not combined with beta-blocker. Evidence forprognosis refers to evidence <strong>of</strong> reducti<strong>on</strong> in CV death or CV death/MI. Evidence for symptoms includes reducti<strong>on</strong> in need for revascularizati<strong>on</strong> and hospitalizati<strong>on</strong> for chest pain.28 ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g>
ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g> 29risk. In additi<strong>on</strong>, COX-2 inhibiti<strong>on</strong> increases <strong>the</strong> risk <strong>of</strong> sufferingstroke, heart failure, and hypertensi<strong>on</strong>. 399 The use<strong>of</strong> unopposed COX-2 inhibiti<strong>on</strong> (i.e. without effective simultaneousplatelet COX-1 inhibiti<strong>on</strong>) should thus be avoided inpatients with stable angina pectoris.N<strong>on</strong>-selective, reversible COX inhibitors (NSAIDs) caninhibit thromboxane producti<strong>on</strong> and platelet aggregati<strong>on</strong>,400,401 as dem<strong>on</strong>strated for naproxen. 402 However, <strong>the</strong>reversible NSAIDs rarely inhibit thromboxane producti<strong>on</strong> aseffectively as aspirin, 385 and it has been shown that ,5%residual COX-1 activity in platelets is sufficient to sustainfull platelet aggregati<strong>on</strong>. 403 <strong>Cardio</strong>protective effects <strong>of</strong>naproxen treatment have been discussed, 404–407 but <strong>the</strong>balance <strong>of</strong> evidence indicates that also n<strong>on</strong>-selectiveNSAIDs may increase <strong>the</strong> risk <strong>of</strong> cardiovascular complicati<strong>on</strong>s.396 It is recommended to primarily use paracetamol.If NSAIDs are needed, <strong>the</strong>y should be used in <strong>the</strong> lowesteffective doses and for <strong>the</strong> shortest possible durati<strong>on</strong>. Awarning has also recently been issued by <strong>the</strong> FDA fornaproxen. 408 NSAID treatment should, when this is indicatedfor o<strong>the</strong>r reas<strong>on</strong>s, be combined with low-dose aspirin toassure effective platelet inhibiti<strong>on</strong> in patients with stableangina pectoris. In such circumstances, ibupr<strong>of</strong>en shouldbe avoided, as this NSAID prevents aspirin from irreversiblyacetylating <strong>the</strong> COX-1 enzyme <strong>of</strong> platelets, as maynaproxen. 409,410 Dicl<strong>of</strong>enac is a relatively COX2-selectiveNSAID and, <strong>the</strong>refore, a poor platelet inhibitor, but doesnot interfere with <strong>the</strong> antiplatelet effects <strong>of</strong> aspirin andmay be used in combinati<strong>on</strong> with aspirin. 411Clopidogrel. Clopidogrel and ticlopidine are thienopyridineswhich act as n<strong>on</strong>-competitive ADP receptor antag<strong>on</strong>ists andwhich have antithrombotic effects similar to aspirin. 385Ticlopidine efficacy has mainly been documented in strokeand PCI 385,387 and has been replaced by clopidogrel due to<strong>the</strong> risk <strong>of</strong> neutropenia and thrombocytopenia and moresymptomatic side-effects with ticlopidine. The main studydocumenting clopidogrel use in stable CAD is CAPRIE, 412which included three equally large groups <strong>of</strong> patients withprevious MI, previous stroke, or peripheral vascular disease(PVD). 412 When compared with aspirin 325 mg/day, whichmay be less effective than 75 mg/day (see Figure 7 inCollaborative Meta-analysis <strong>of</strong> Randomized Trials 387 ), clopidogrel75 mg/day was slightly more effective (ARR 0.51%per year; P ¼ 0.043) in preventing cardiovascular complicati<strong>on</strong>sin high-risk patients. 412 When comparing outcomesin <strong>the</strong> three subgroups <strong>of</strong> patients enrolled in CAPRIE, <strong>the</strong>benefit with clopidogrel appeared in <strong>the</strong> PVD subgroup<strong>on</strong>ly. 412 Gastrointestinal haemorrhage was <strong>on</strong>ly slightly lesscomm<strong>on</strong> with clopidogrel compared with aspirin treatment(1.99 vs. 2.66% during 1.9 years <strong>of</strong> treatment), despite <strong>the</strong>relatively high aspirin dose. 412 The benefit <strong>of</strong> clopidogrelmay have been over-estimated because <strong>the</strong> dose <strong>of</strong> aspirinwith which it was compared (325 mg) may not be <strong>the</strong> mosteffective dose. The CAPRIE study did not include patientswith aspirin intolerance, and we do not know <strong>the</strong> risk <strong>of</strong> gastrointestinalbleeding during clopidogrel compared withplacebo treatment. Clopidogrel is more expensive thanaspirin, but may be c<strong>on</strong>sidered in aspirin-intolerant patientswith significant risks <strong>of</strong> arterial thrombosis. Gastrointestinalintolerance may, however, be handled differently (discussedsubsequently). After cor<strong>on</strong>ary stenting, an acute cor<strong>on</strong>arysyndrome, or an ST-elevati<strong>on</strong> MI, clopidogrel may becombined with aspirin during a finite period <strong>of</strong> time, butcombinati<strong>on</strong> <strong>the</strong>rapy is currently not warranted in stableangina pectoris. Clopidogrel treatment increases <strong>the</strong> risk<strong>of</strong> severe bleeding in c<strong>on</strong>necti<strong>on</strong> with CABG surgery. 413One much discussed reas<strong>on</strong> for variability <strong>of</strong> antiplateletresp<strong>on</strong>ses to clopidogrel is drug–drug interacti<strong>on</strong>s, as clopidogrelforms its active metabolite(s) via CYP3A4-mediatedmetabolism. A study by Lau et al. 414 showed that atorvastatin,but not pravastatin, dose-dependently inhibited <strong>the</strong>effect <strong>of</strong> clopidogrel <strong>on</strong> ADP-mediated platelet activati<strong>on</strong>.The study also showed <strong>the</strong> expected interacti<strong>on</strong>s betweenclopidogrel and antibiotics that inhibit (erythromycin andtroleandomycin) or induce (rifampicin) CYP3A4. 414 Ano<strong>the</strong>rstudy with clopidogrel maintenance treatment found nointeracti<strong>on</strong> with low-dose atorvastatin (10 mg daily) treatment.415 The short-term effects <strong>of</strong> a 300 mg loading dose<strong>of</strong> clopidogrel in c<strong>on</strong>necti<strong>on</strong> with PCI may 416 or may not 417be attenuated by co-treatment with lipophilic statins (atorvastatin,simvastatin, and lovastatin). The effects <strong>of</strong> a600 mg loading dose appear to be unaffected by treatmentwith atorvastatin or simvastatin. 418,419 Observati<strong>on</strong>al posthoc analyses <strong>of</strong> outcomes am<strong>on</strong>g patients receiving maintenanceco-treatment with clopidogrel and interacting statinhave not shown differences in outcome, but <strong>the</strong>re are noproperly designed prospective studies that address <strong>the</strong>issue. Data from <strong>the</strong> large GRACE registry indicate thatstatin treatment has additi<strong>on</strong>al benefit to those <strong>of</strong> clopidogreltreatment, as might be expected. 420 Thus, <strong>the</strong> literature <strong>on</strong>statin–clopidogrel interacti<strong>on</strong>s is inc<strong>on</strong>sistent, and <strong>the</strong>importance <strong>of</strong> interacti<strong>on</strong>s between maintenance <strong>the</strong>rapywith lipophilic statins and clopidogrel is at present not known.Antiplatelet <strong>the</strong>rapy in patients with gastrointestinalintolerance to aspirin. Gastrointestinal haemorrhages mayincrease with any antiplatelet treatment, but <strong>the</strong> size <strong>of</strong>this effect with clopidogrel is not known in <strong>the</strong> absence <strong>of</strong>data from placebo-c<strong>on</strong>trolled trials. It has been speculatedthat antiplatelet treatment interferes with <strong>the</strong> normalwound healing process which limits <strong>the</strong> progressi<strong>on</strong> <strong>of</strong> subclinicaland ra<strong>the</strong>r comm<strong>on</strong> (2% per m<strong>on</strong>th without anytreatment) gastric erosi<strong>on</strong>s, due to reduced release <strong>of</strong> plateletstored growth factors such as VEGF. 421 In additi<strong>on</strong>, aspirincauses dose-related gastric mucosal damage which mayincrease <strong>the</strong> incidence and severity <strong>of</strong> erosi<strong>on</strong>s. Upper gastrointestinalbleeding due to aspirin or NSAID <strong>the</strong>rapy maybe alleviated by inhibiting gastric acid secreti<strong>on</strong>.Eradicati<strong>on</strong> <strong>of</strong> Helicobacter pylori infecti<strong>on</strong>, if present,also reduces <strong>the</strong> risk <strong>of</strong> aspirin-related gastorintestinalbleeding. 422Am<strong>on</strong>g <strong>the</strong> different acid reducing <strong>the</strong>rapies available,prot<strong>on</strong> pump inibitor (PPI) treatment has been best documented.Thus, 30 mg/day <strong>of</strong> lansoprazole reduced <strong>the</strong>recurrence <strong>of</strong> ulcer complicati<strong>on</strong>s from 14.8% in <strong>the</strong>placebo group to 1.6% (P ¼ 0.008) during a 12-m<strong>on</strong>thfollow-up <strong>of</strong> gastroduodenal ulcer patients treated with100 mg aspirin after H. pylori eradicati<strong>on</strong>. 423 A recentstudy showed that <strong>the</strong> additi<strong>on</strong> <strong>of</strong> a PPI (esomeprazole40 mg/day) to aspirin (80 mg/day) was better than switchingto clopidogrel for <strong>the</strong> preventi<strong>on</strong> <strong>of</strong> recurrent ulcer bleedingin patients with ulcers and vascular disease. 424Dipyridamole and anticoagulants. Dipyridamole is not recommendedfor antithrombotic treatment in stable anginadue to poor antithrombotic efficacy 387 and <strong>the</strong> risk <strong>of</strong>