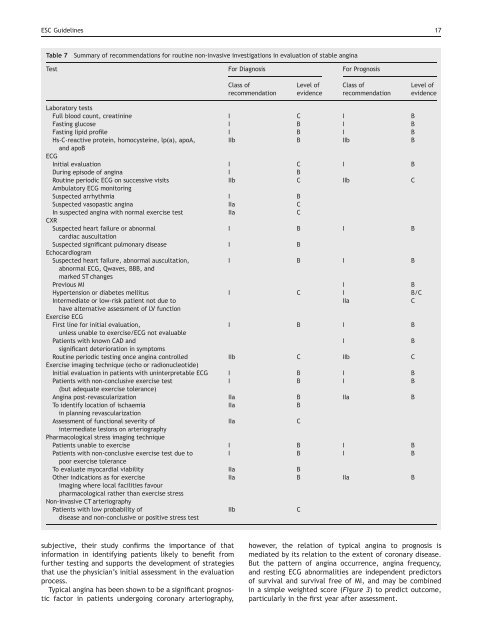
16 ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g>anti-anginal <strong>the</strong>rapy in stable cor<strong>on</strong>ary disease publishedsince 2000 are illustrated in Figure 1. The rate <strong>of</strong> cardiovasculardeath in <strong>the</strong> PEACE 252 study was less than 1% perannum, whereas in ‘high-risk’ populati<strong>on</strong>s such as in diabeticMICRO-HOPE 253 populati<strong>on</strong> and <strong>the</strong> IONA 254 populati<strong>on</strong> <strong>the</strong>annualized cardiovascular mortality rate was .2%. For <strong>the</strong>purposes <strong>of</strong> <strong>the</strong>se guidelines, unless qualified differently in<strong>the</strong> text, if an individual with angina is determined <strong>on</strong> <strong>the</strong>basis <strong>of</strong> a well validated risk predicti<strong>on</strong> model, to haveannual cardiovascular mortality <strong>of</strong> .2% that individual isdeemed high risk, whereas an annual cardiovascular mortality<strong>of</strong> ,1% is c<strong>on</strong>sidered low risk, and 1–2% intermediaterisk.The clinical evaluati<strong>on</strong>, <strong>the</strong> resp<strong>on</strong>se to stress testing,<strong>the</strong> quantificati<strong>on</strong> <strong>of</strong> ventricular functi<strong>on</strong>, and <strong>the</strong> extent<strong>of</strong> CAD are <strong>the</strong> four key pieces <strong>of</strong> informati<strong>on</strong> to stratifypatient’s risk. 66–68,124,255,256 However, not all patients willrequire invasive assessment <strong>of</strong> <strong>the</strong> cor<strong>on</strong>ary anatomy, particularlyif <strong>the</strong>ir clinical evaluati<strong>on</strong> and n<strong>on</strong>-invasivetesting establish that <strong>the</strong>y are in a low-risk group. The riskassessment hierarchy can be described as:(1) Risk stratificati<strong>on</strong> by clinical evaluati<strong>on</strong>(2) Risk stratificati<strong>on</strong> by resp<strong>on</strong>se to stress testing(3) Risk stratificati<strong>on</strong> by ventricular functi<strong>on</strong>(4) Risk stratificati<strong>on</strong> by cor<strong>on</strong>ary anatomyThe route through <strong>the</strong>se successive tests may not alwaysbe directly linear. For example in a patient with a highpre-test probability <strong>of</strong> disease, severe angina, and o<strong>the</strong>rhigh-risk clinical features such as signs <strong>of</strong> heart failure,may proceed directly from clinical evaluati<strong>on</strong> to cor<strong>on</strong>aryarteriography, with perfusi<strong>on</strong> scintigraphy afterwards toevaluate myocardial viability. However, risk stratificati<strong>on</strong>generally follows a pyramidal structure, with all patientsrequiring risk stratificati<strong>on</strong> by clinical evaluati<strong>on</strong> as <strong>the</strong>most basic requirement, proceeding in <strong>the</strong> majority to n<strong>on</strong>invasiveassessment <strong>of</strong> ischaemia and ventricular functi<strong>on</strong>,and finally cor<strong>on</strong>ary arteriography in a selected proporti<strong>on</strong>.A summary <strong>of</strong> <strong>the</strong> recommendati<strong>on</strong>s for <strong>the</strong> routine use <strong>of</strong>investigati<strong>on</strong>s in evaluati<strong>on</strong> <strong>of</strong> stable angina with corresp<strong>on</strong>dinglevels <strong>of</strong> evidence related to diagnosis and prognosis,is presented in Table 7, and an algorithm for <strong>the</strong> initialevaluati<strong>on</strong> <strong>of</strong> patients presenting with clinical symptomssuggestive <strong>of</strong> angina is depicted in Figure 2.Risk stratificati<strong>on</strong> using clinical evaluati<strong>on</strong>The clinical history and physical examinati<strong>on</strong> can providevery important prognostic informati<strong>on</strong>. ECG can be c<strong>on</strong>venientlyincorporated in risk stratificati<strong>on</strong> at this level,and <strong>the</strong> results <strong>of</strong> <strong>the</strong> laboratory tests discussed in <strong>the</strong> previoussecti<strong>on</strong> may modify risk estimati<strong>on</strong> fur<strong>the</strong>r. Diabetes,hypertensi<strong>on</strong>, current smoking, and elevated total cholesterol(untreated or elevated despite treatment) have beenshown to be predictive <strong>of</strong> adverse outcome in patientswith stable angina or o<strong>the</strong>r populati<strong>on</strong>s with established cor<strong>on</strong>arydisease. 56,58,257–259 Increasing age is an importantfactor to c<strong>on</strong>sider, as are prior MI, 66,123 symptoms andsigns <strong>of</strong> heart failure, 66,123,124 and <strong>the</strong> pattern <strong>of</strong> occurrence(recent <strong>on</strong>set or progressive), and severity <strong>of</strong> angina,particularly if unresp<strong>on</strong>sive to <strong>the</strong>rapy. 255,260Pryor et al. 261 studied a total <strong>of</strong> 1030 c<strong>on</strong>secutive outpatientsreferred to n<strong>on</strong>-invasive testing for suspectedCAD; <strong>the</strong> informati<strong>on</strong> from <strong>the</strong> initial history, physical examinati<strong>on</strong>,ECG, and chest radiograph was used to predict cor<strong>on</strong>aryanatomy, i.e. <strong>the</strong> likelihood <strong>of</strong> any significant cor<strong>on</strong>arydisease, severe disease, and significant left main (LM)disease and to estimate 3 years survival. These estimateswere compared with those based <strong>on</strong> treadmill testing.Compared with <strong>the</strong> treadmill exercise test, initialevaluati<strong>on</strong> was slightly better able to distinguish patientswith or without CAD and was similar in <strong>the</strong> ability toidentify patients at increased risk for dying or with anatomicallysevere disease. Although much <strong>of</strong> <strong>the</strong> informati<strong>on</strong>obtained by physicians during <strong>the</strong> initial assessment isFigure 1 <strong>Cardio</strong>vascular mortality and myocardial infarcti<strong>on</strong> in c<strong>on</strong>temporary trials <strong>of</strong> stable cor<strong>on</strong>ary disease or angina: CAMELOT, 467 PEACE, 252 ACTION, 493EUROPA, 461 HOPE, 460 IONA, 254 and MICRO-HOPE. 253
ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g> 17Table 7Summary <strong>of</strong> recommendati<strong>on</strong>s for routine n<strong>on</strong>-invasive investigati<strong>on</strong>s in evaluati<strong>on</strong> <strong>of</strong> stable anginaTest For Diagnosis For PrognosisClass <strong>of</strong>recommendati<strong>on</strong>Level <strong>of</strong>evidenceClass <strong>of</strong>recommendati<strong>on</strong>Level <strong>of</strong>evidenceLaboratory testsFull blood count, creatinine I C I BFasting glucose I B I BFasting lipid pr<strong>of</strong>ile I B I BHs-C-reactive protein, homocysteine, lp(a), apoA,IIb B IIb Band apoBECGInitial evaluati<strong>on</strong> I C I BDuring episode <strong>of</strong> angina I BRoutine periodic ECG <strong>on</strong> successive visits IIb C IIb CAmbulatory ECG m<strong>on</strong>itoringSuspected arrhythmia I BSuspected vasopastic angina IIa CIn suspected angina with normal exercise test IIa CCXRSuspected heart failure or abnormalI B I Bcardiac auscultati<strong>on</strong>Suspected significant pulm<strong>on</strong>ary disease I BEchocardiogramSuspected heart failure, abnormal auscultati<strong>on</strong>,I B I Babnormal ECG, Qwaves, BBB, andmarked ST changesPrevious MI I BHypertensi<strong>on</strong> or diabetes mellitus I C I B/CIntermediate or low-risk patient not due toIIaChave alternative assessment <strong>of</strong> LV functi<strong>on</strong>Exercise ECGFirst line for initial evaluati<strong>on</strong>,I B I Bunless unable to exercise/ECG not evaluablePatients with known CAD andIBsignificant deteriorati<strong>on</strong> in symptomsRoutine periodic testing <strong>on</strong>ce angina c<strong>on</strong>trolled IIb C IIb CExercise imaging technique (echo or radi<strong>on</strong>ucleotide)Initial evaluati<strong>on</strong> in patients with uninterpretable ECG I B I BPatients with n<strong>on</strong>-c<strong>on</strong>clusive exercise testI B I B(but adequate exercise tolerance)<strong>Angina</strong> post-revascularizati<strong>on</strong> IIa B IIa BTo identify locati<strong>on</strong> <strong>of</strong> ischaemiaIIaBin planning revascularizati<strong>on</strong>Assessment <strong>of</strong> functi<strong>on</strong>al severity <strong>of</strong>IIaCintermediate lesi<strong>on</strong>s <strong>on</strong> arteriographyPharmacological stress imaging techniquePatients unable to exercise I B I BPatients with n<strong>on</strong>-c<strong>on</strong>clusive exercise test due toI B I Bpoor exercise toleranceTo evaluate myocardial viability IIa BO<strong>the</strong>r indicati<strong>on</strong>s as for exerciseIIa B IIa Bimaging where local facilities favourpharmacological ra<strong>the</strong>r than exercise stressN<strong>on</strong>-invasive CT arteriographyPatients with low probability <strong>of</strong>disease and n<strong>on</strong>-c<strong>on</strong>clusive or positive stress testIIbCsubjective, <strong>the</strong>ir study c<strong>on</strong>firms <strong>the</strong> importance <strong>of</strong> thatinformati<strong>on</strong> in identifying patients likely to benefit fromfur<strong>the</strong>r testing and supports <strong>the</strong> development <strong>of</strong> strategiesthat use <strong>the</strong> physician’s initial assessment in <strong>the</strong> evaluati<strong>on</strong>process.Typical angina has been shown to be a significant prognosticfactor in patients undergoing cor<strong>on</strong>ary arteriography,however, <strong>the</strong> relati<strong>on</strong> <strong>of</strong> typical angina to prognosis ismediated by its relati<strong>on</strong> to <strong>the</strong> extent <strong>of</strong> cor<strong>on</strong>ary disease.But <strong>the</strong> pattern <strong>of</strong> angina occurrence, angina frequency,and resting ECG abnormalities are independent predictors<strong>of</strong> survival and survival free <strong>of</strong> MI, and may be combinedin a simple weighted score (Figure 3) to predict outcome,particularly in <strong>the</strong> first year after assessment.