

Guidelines on the Management of Stable Angina Pectoris ... - Cardio
Guidelines on the Management of Stable Angina Pectoris ... - Cardio
Guidelines on the Management of Stable Angina Pectoris ... - Cardio

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
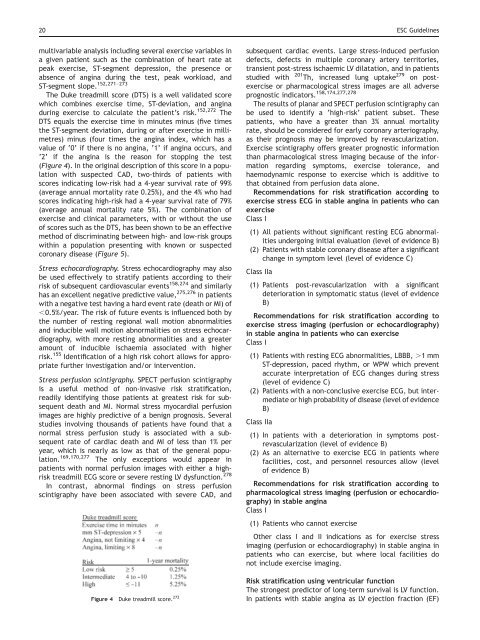
20 ESC <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g>multivariable analysis including several exercise variables ina given patient such as <strong>the</strong> combinati<strong>on</strong> <strong>of</strong> heart rate atpeak exercise, ST-segment depressi<strong>on</strong>, <strong>the</strong> presence orabsence <strong>of</strong> angina during <strong>the</strong> test, peak workload, andST-segment slope. 152,271–273The Duke treadmill score (DTS) is a well validated scorewhich combines exercise time, ST-deviati<strong>on</strong>, and anginaduring exercise to calculate <strong>the</strong> patient’s risk. 152,272 TheDTS equals <strong>the</strong> exercise time in minutes minus (five times<strong>the</strong> ST-segment deviati<strong>on</strong>, during or after exercise in millimetres)minus (four times <strong>the</strong> angina index, which has avalue <strong>of</strong> ‘0’ if <strong>the</strong>re is no angina, ‘1’ if angina occurs, and‘2’ if <strong>the</strong> angina is <strong>the</strong> reas<strong>on</strong> for stopping <strong>the</strong> test(Figure 4). In <strong>the</strong> original descripti<strong>on</strong> <strong>of</strong> this score in a populati<strong>on</strong>with suspected CAD, two-thirds <strong>of</strong> patients withscores indicating low-risk had a 4-year survival rate <strong>of</strong> 99%(average annual mortality rate 0.25%), and <strong>the</strong> 4% who hadscores indicating high-risk had a 4-year survival rate <strong>of</strong> 79%(average annual mortality rate 5%). The combinati<strong>on</strong> <strong>of</strong>exercise and clinical parameters, with or without <strong>the</strong> use<strong>of</strong> scores such as <strong>the</strong> DTS, has been shown to be an effectivemethod <strong>of</strong> discriminating between high- and low-risk groupswithin a populati<strong>on</strong> presenting with known or suspectedcor<strong>on</strong>ary disease (Figure 5).Stress echocardiography. Stress echocardiography may alsobe used effectively to stratify patients according to <strong>the</strong>irrisk <strong>of</strong> subsequent cardiovascular events 158,274 and similarlyhas an excellent negative predictive value, 275,276 in patientswith a negative test having a hard event rate (death or MI) <strong>of</strong>,0.5%/year. The risk <strong>of</strong> future events is influenced both by<strong>the</strong> number <strong>of</strong> resting regi<strong>on</strong>al wall moti<strong>on</strong> abnormalitiesand inducible wall moti<strong>on</strong> abnormalities <strong>on</strong> stress echocardiography,with more resting abnormalities and a greateramount <strong>of</strong> inducible ischaemia associated with higherrisk. 155 Identificati<strong>on</strong> <strong>of</strong> a high risk cohort allows for appropriatefur<strong>the</strong>r investigati<strong>on</strong> and/or interventi<strong>on</strong>.Stress perfusi<strong>on</strong> scintigraphy. SPECT perfusi<strong>on</strong> scintigraphyis a useful method <strong>of</strong> n<strong>on</strong>-invasive risk stratificati<strong>on</strong>,readily identifying those patients at greatest risk for subsequentdeath and MI. Normal stress myocardial perfusi<strong>on</strong>images are highly predictive <strong>of</strong> a benign prognosis. Severalstudies involving thousands <strong>of</strong> patients have found that anormal stress perfusi<strong>on</strong> study is associated with a subsequentrate <strong>of</strong> cardiac death and MI <strong>of</strong> less than 1% peryear, which is nearly as low as that <strong>of</strong> <strong>the</strong> general populati<strong>on</strong>.169,170,277 The <strong>on</strong>ly excepti<strong>on</strong>s would appear inpatients with normal perfusi<strong>on</strong> images with ei<strong>the</strong>r a highrisktreadmill ECG score or severe resting LV dysfuncti<strong>on</strong>. 278In c<strong>on</strong>trast, abnormal findings <strong>on</strong> stress perfusi<strong>on</strong>scintigraphy have been associated with severe CAD, andFigure 4 Duke treadmill score. 272subsequent cardiac events. Large stress-induced perfusi<strong>on</strong>defects, defects in multiple cor<strong>on</strong>ary artery territories,transient post-stress ischaemic LV dilatati<strong>on</strong>, and in patientsstudied with 201 Th, increased lung uptake 279 <strong>on</strong> postexerciseor pharmacological stress images are all adverseprognostic indicators. 158,174,277,278The results <strong>of</strong> planar and SPECT perfusi<strong>on</strong> scintigraphy canbe used to identify a ‘high-risk’ patient subset. Thesepatients, who have a greater than 3% annual mortalityrate, should be c<strong>on</strong>sidered for early cor<strong>on</strong>ary arteriography,as <strong>the</strong>ir prognosis may be improved by revascularizati<strong>on</strong>.Exercise scintigraphy <strong>of</strong>fers greater prognostic informati<strong>on</strong>than pharmacological stress imaging because <strong>of</strong> <strong>the</strong> informati<strong>on</strong>regarding symptoms, exercise tolerance, andhaemodynamic resp<strong>on</strong>se to exercise which is additive tothat obtained from perfusi<strong>on</strong> data al<strong>on</strong>e.Recommendati<strong>on</strong>s for risk stratificati<strong>on</strong> according toexercise stress ECG in stable angina in patients who canexerciseClass I(1) All patients without significant resting ECG abnormalitiesundergoing initial evaluati<strong>on</strong> (level <strong>of</strong> evidence B)(2) Patients with stable cor<strong>on</strong>ary disease after a significantchange in symptom level (level <strong>of</strong> evidence C)Class IIa(1) Patients post-revascularizati<strong>on</strong> with a significantdeteriorati<strong>on</strong> in symptomatic status (level <strong>of</strong> evidenceB)Recommendati<strong>on</strong>s for risk stratificati<strong>on</strong> according toexercise stress imaging (perfusi<strong>on</strong> or echocardiography)in stable angina in patients who can exerciseClass I(1) Patients with resting ECG abnormalities, LBBB, .1 mmST-depressi<strong>on</strong>, paced rhythm, or WPW which preventaccurate interpretati<strong>on</strong> <strong>of</strong> ECG changes during stress(level <strong>of</strong> evidence C)(2) Patients with a n<strong>on</strong>-c<strong>on</strong>clusive exercise ECG, but intermediateor high probability <strong>of</strong> disease (level <strong>of</strong> evidenceB)Class IIa(1) In patients with a deteriorati<strong>on</strong> in symptoms postrevascularizati<strong>on</strong>(level <strong>of</strong> evidence B)(2) As an alternative to exercise ECG in patients wherefacilities, cost, and pers<strong>on</strong>nel resources allow (level<strong>of</strong> evidence B)Recommendati<strong>on</strong>s for risk stratificati<strong>on</strong> according topharmacological stress imaging (perfusi<strong>on</strong> or echocardiography)in stable anginaClass I(1) Patients who cannot exerciseO<strong>the</strong>r class I and II indicati<strong>on</strong>s as for exercise stressimaging (perfusi<strong>on</strong> or echocardiography) in stable angina inpatients who can exercise, but where local facilities d<strong>on</strong>ot include exercise imaging.Risk stratificati<strong>on</strong> using ventricular functi<strong>on</strong>The str<strong>on</strong>gest predictor <strong>of</strong> l<strong>on</strong>g-term survival is LV functi<strong>on</strong>.In patients with stable angina as LV ejecti<strong>on</strong> fracti<strong>on</strong> (EF)











