LETTERSMid trimester biometric measurementsTo the Editor,We would like to br<strong>in</strong>g to the attention of youand your readers our article entitled Ultrasonicfetal size measurements <strong>in</strong> Brisbane that wasrecently published <strong>in</strong> the peer reviewed sisterjournal, <strong>Australasian</strong> Radiology 1 . This articleconstructed population specific charts of fetalbiometry <strong>for</strong> 11 to 41 weeks gestation <strong>in</strong> relationto known gestational age from a large populationof normal Australian pregnancies wherethe exam<strong>in</strong>ation was per<strong>for</strong>med to an Australianand New Zealand (ANZ) standard protocol byexperienced operators. Motivation <strong>in</strong>cluded thefact that overseas charts, up to 25 years old,are currently employed <strong>for</strong> many fetal parameterswith<strong>in</strong> ANZ 2,3 and that the development ofappropriate localised charts have been criticisedby some ultrasonic specialists and practitioners<strong>in</strong> Australia because of their suboptimalmethodological rigour 4 . To remedy this, we presentedmethodologically rigorous, current andpopulation appropriate biometric equations andtables of ultrasonic fetal measurement and 95%reference ranges <strong>for</strong> biparietal diameter (BPD),femur length (FL), abdom<strong>in</strong>al circumference(AC) and head circumference (HC).We believe that this dataset can be used togenerate valid reference centiles <strong>for</strong> fetal size.In most respects, it meets Altman and Chitty's 5,6and Nisbet and de Crespigny's 4,7 criteria <strong>for</strong> design and isreadily exportable <strong>for</strong> statistical analysis, also consistentwith Altman and Chitty's recommendations. It has theadvantage of be<strong>in</strong>g a very large sample collected from anentirely Australian population us<strong>in</strong>g a customized database,PacUser TM 8 . All exam<strong>in</strong>ations were per<strong>for</strong>med byvery experienced operators, yet none of the protocols <strong>for</strong>measurement are beyond the capacity of any sonographer.An attempt should be made by each sonographer to achievethe same rigor with each exam<strong>in</strong>ation. It is our belief thatneither fetal measurement nor gestational age should bedependent upon operator experience.In summary, we assert that the presented results are themost rigorously derived and applicable to the Australianpopulation. The result<strong>in</strong>g tables have been provided to theASUM Federal Council <strong>for</strong> their consideration with a viewto amend<strong>in</strong>g the current recommendations <strong>for</strong> fetal biometry.We would suggest that your readers <strong>in</strong>vestigate the useof these tables <strong>in</strong> their practice.We would also welcome readers to submit their deidentifieddatabases to us to <strong>in</strong>crease the sample sizeand to check the reliability of these equations.We would like to thank the sonographers <strong>in</strong>volved <strong>in</strong>this project <strong>for</strong> their excellent work: Ms Teresa Clapham,Ms Helen Gofton, Ms Julie Naylor, Mr Neil Pennell andMs Sue Williams.For further <strong>in</strong><strong>for</strong>mation about the methodology, thestatistical analysis, the results and equations, readers areencouraged to access the journal articles 1,9 or to contact DrGary Pritchard directly.14 ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2005 August; 8 (3)Table 1 Ultrasonic fetal measurement means and 95% reference <strong>in</strong>tervals (95% RI)by gestational age measured <strong>in</strong> weeks.Gestation BPD FL AC HC(weeks) mean (95%RI) mean (95% RI) mean (95% RI) mean (95% RI)11 21 (19, 23) 5 (2, 8) 53 (42, 63) 75 (66, 84)12 24 (21, 26) 8 (5, 11) 63 (52, 73) 85 (75, 94)13 26 (23, 29) 11 (8, 15) 73 (61, 84) 95 (84, 105)14 29 (26, 32) 14 (11, 18) 83 (71, 95) 105 (94, 116)15 32 (28, 35) 17 (14, 21) 94 (81, 106) 116 (104, 127)16 35 (31, 38) 20 (17, 24) 105 (92, 118) 126 (114, 139)17 38 (34, 41) 23 (20, 27) 116 (102, 130) 138 (125, 150)18 41 (36, 45) 26 (22, 30) 127 (112, 142) 149 (136, 162)19 44 (39, 48) 29 (25, 32) 138 (123, 154) 161 (147, 175)20 47 (42, 51) 31 (28, 35) 150 (133, 166) 172 (158, 187)21 50 (45, 55) 34 (30, 38) 161 (144, 178) 184 (169, 199)22 53 (48, 58) 37 (33, 41) 172 (154, 191) 195 (180, 211)23 56 (51, 61) 39 (35, 43) 184 (164, 203) 207 (190, 223)24 59 (54, 64) 42 (38, 46) 195 (175, 215) 218 (201, 235)25 62 (56, 68) 44 (40, 49) 206 (185, 228) 229 (212, 247)26 65 (59, 71) 47 (42, 51) 218 (195, 240) 240 (222, 259)27 68 (62, 74) 49 (45, 54) 229 (205, 252) 251 (232, 270)28 71 (65, 77) 51 (47, 56) 240 (215, 265) 261 (241, 281)29 74 (67, 80) 54 (49, 58) 251 (224, 277) 271 (250, 291)30 76 (70, 83) 56 (51, 61) 261 (234, 289) 280 (259, 301)31 79 (72, 85) 58 (53, 63) 272 (243, 301) 288 (267, 310)32 81 (74, 88) 60 (54, 65) 282 (252, 312) 297 (274, 319)33 83 (76, 90) 62 (56, 67) 292 (261, 324) 304 (281, 327)34 85 (78, 93) 63 (58, 69) 302 (269, 335) 311 (287, 334)35 87 (80, 95) 65 (59, 71) 312 (277, 347) 316 (292, 340)36 89 (81, 97) 67 (61, 73) 321 (285, 357) 321 (297, 346)37 90 (83, 98) 68 (62, 74) 330 (292, 368) 326 (300, 351)38 92 (84, 100) 70 (63, 76) 339 (300, 379) 329 (303, 355)39 93 (85, 101) 71 (64, 78) 348 (307, 389) 331 (305, 358)40 94 (85, 102) 72 (65, 79) 356 (313, 399) 332 (305, 359)41 94 (86, 102) 73 (66, 80) 364 (319, 406) 332 (305, 360)Prof Philip SchluterAuckland University of TechnologyDr Gary PritchardBrisbane <strong>Ultrasound</strong> <strong>for</strong> Women Email bufw@bigpond.comMs Margo Gill Brisbane <strong>Ultrasound</strong> <strong>for</strong> WomenReferences1 Schluter P, Pritchard G, Gill M. Ultrasonic fetal size measurements<strong>in</strong> Brisbane, Australia. Australas Radiol 2004; 48: 480-486.2 Westerway S, Davison A, Cowell S. Ultrasonic fetal measurements:new Australian standards <strong>for</strong> the new millennium. Aust N Z J ObstetGynaecol; 40 (3): 297–302.3 <strong>Australasian</strong> <strong>Society</strong> <strong>for</strong> <strong>Ultrasound</strong> <strong>in</strong> Medic<strong>in</strong>e. Statement on normalultrasonic fetal measurements. ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2001;4 (3): 28–31.4 Nisbet D, de Crespigny L. Policy Statement on normal ultrasonicfetal measurements. ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2002; 5 (4): 32.5 Altman D, Chitty L. Design and analysis of studies to derive chartsof fetal size. <strong>Ultrasound</strong> Obstet Gynecol 1993; 3 (6): 378–384.6 Altman D, Chitty L. Charts of fetal size: 1. Methodology. BJOG1994; 101: 29–34.7 Nisbet D, de Crespigny L. How should the ultrasound estimated duedate be calculated? ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2002; 5 (1): 20–21.8 Precise Accurate Convenient <strong>Ultrasound</strong> Exam<strong>in</strong>ation Report<strong>in</strong>g(Pacuser) [computer program]. Version 1. Brisbane: Pacuser, www.pacuser.com.au; 1993.9 Schluter P, Pritchard G, Gill M. Corrigendum: Ultrasonic fetal size measurements<strong>in</strong> Brisbane, Australia. Australas Radiol 2005; 49: 345.
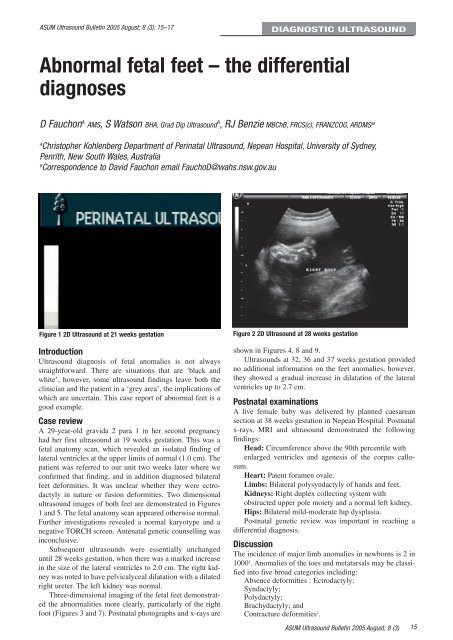
ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2005 August; 8 (3): 15–17DIAGNOSTIC ULTRASOUNDAbnormal fetal feet – the differentialdiagnosesD Fauchon A AMS, S Watson BHA, Grad Dip <strong>Ultrasound</strong> A , RJ Benzie MBChB, FRCS(c), FRANZCOG, ARDMS ABAChristopher Kohlenberg Department of Per<strong>in</strong>atal <strong>Ultrasound</strong>, Nepean Hospital, University of Sydney,Penrith, New South Wales, AustraliaBCorrespondence to David Fauchon email FauchoD@wahs.nsw.gov.auFigure 1 2D <strong>Ultrasound</strong> at 21 weeks gestationIntroduction<strong>Ultrasound</strong> diagnosis of fetal anomalies is not alwaysstraight<strong>for</strong>ward. There are situations that are ‘black andwhite’, however, some ultrasound f<strong>in</strong>d<strong>in</strong>gs leave both thecl<strong>in</strong>ician and the patient <strong>in</strong> a ‘grey area’, the implications ofwhich are uncerta<strong>in</strong>. This case report of abnormal feet is agood example.Case reviewA 29-year-old gravida 2 para 1 <strong>in</strong> her second pregnancyhad her first ultrasound at 19 weeks gestation. This was afetal anatomy scan, which revealed an isolated f<strong>in</strong>d<strong>in</strong>g oflateral ventricles at the upper limits of normal (1.0 cm). Thepatient was referred to our unit two weeks later where weconfirmed that f<strong>in</strong>d<strong>in</strong>g, and <strong>in</strong> addition diagnosed bilateralfeet de<strong>for</strong>mities. It was unclear whether they were ectrodactyly<strong>in</strong> nature or fusion de<strong>for</strong>mities. Two dimensionalultrasound images of both feet are demonstrated <strong>in</strong> Figures1 and 5. The fetal anatomy scan appeared otherwise normal.Further <strong>in</strong>vestigations revealed a normal karyotype and anegative TORCH screen. Antenatal genetic counsell<strong>in</strong>g was<strong>in</strong>conclusive.Subsequent ultrasounds were essentially unchangeduntil 28 weeks gestation, when there was a marked <strong>in</strong>crease<strong>in</strong> the size of the lateral ventricles to 2.0 cm. The right kidneywas noted to have pelvicalyceal dilatation with a dilatedright ureter. The left kidney was normal.Three-dimensional imag<strong>in</strong>g of the fetal feet demonstratedthe abnormalities more clearly, particularly of the rightfoot (Figures 3 and 7). Postnatal photographs and x-rays areFigure 2 2D <strong>Ultrasound</strong> at 28 weeks gestationshown <strong>in</strong> Figures 4, 8 and 9.<strong>Ultrasound</strong>s at 32, 36 and 37 weeks gestation providedno additional <strong>in</strong><strong>for</strong>mation on the feet anomalies, however,they showed a gradual <strong>in</strong>crease <strong>in</strong> dilatation of the lateralventricles up to 2.7 cm.Postnatal exam<strong>in</strong>ationsA live female baby was delivered by planned caesareansection at 38 weeks gestation <strong>in</strong> Nepean Hospital. Postnatalx-rays, MRI and ultrasound demonstrated the follow<strong>in</strong>gf<strong>in</strong>d<strong>in</strong>gs:Head: Circumference above the 90th percentile withenlarged ventricles and agenesis of the corpus callosum.Heart: Patent <strong>for</strong>amen ovale.Limbs: Bilateral polysyndactyly of hands and feet.Kidneys: Right duplex collect<strong>in</strong>g system withobstructed upper pole moiety and a normal left kidney.Hips: Bilateral mild-moderate hip dysplasia.Postnatal genetic review was important <strong>in</strong> reach<strong>in</strong>g adifferential diagnosis.DiscussionThe <strong>in</strong>cidence of major limb anomalies <strong>in</strong> newborns is 2 <strong>in</strong>1000 1 . Anomalies of the toes and metatarsals may be classified<strong>in</strong>to five broad categories <strong>in</strong>clud<strong>in</strong>g:Absence de<strong>for</strong>mities : Ectrodactyly;Syndactyly;Polydactyly;Brachydactyly; andContracture de<strong>for</strong>mities 2 .ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2005 August; 8 (3)15