

Volume 8 Issue 3 - Australasian Society for Ultrasound in Medicine
Volume 8 Issue 3 - Australasian Society for Ultrasound in Medicine
Volume 8 Issue 3 - Australasian Society for Ultrasound in Medicine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
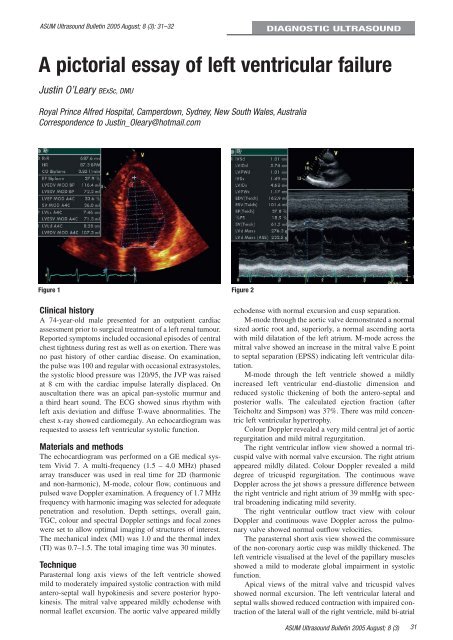
ASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2005 August; 8 (3): 31–32DIAGNOSTIC ULTRASOUNDA pictorial essay of left ventricular failureJust<strong>in</strong> O’Leary BExSc, DMURoyal Pr<strong>in</strong>ce Alfred Hospital, Camperdown, Sydney, New South Wales, AustraliaCorrespondence to Just<strong>in</strong>_Oleary@hotmail.comFigure 1 Figure 2Cl<strong>in</strong>ical historyA 74-year-old male presented <strong>for</strong> an outpatient cardiacassessment prior to surgical treatment of a left renal tumour.Reported symptoms <strong>in</strong>cluded occasional episodes of centralchest tightness dur<strong>in</strong>g rest as well as on exertion. There wasno past history of other cardiac disease. On exam<strong>in</strong>ation,the pulse was 100 and regular with occasional extrasystoles,the systolic blood pressure was 120/95, the JVP was raisedat 8 cm with the cardiac impulse laterally displaced. Onauscultation there was an apical pan-systolic murmur anda third heart sound. The ECG showed s<strong>in</strong>us rhythm withleft axis deviation and diffuse T-wave abnormalities. Thechest x-ray showed cardiomegaly. An echocardiogram wasrequested to assess left ventricular systolic function.Materials and methodsThe echocardiogram was per<strong>for</strong>med on a GE medical systemVivid 7. A multi-frequency (1.5 – 4.0 MHz) phasedarray transducer was used <strong>in</strong> real time <strong>for</strong> 2D (harmonicand non-harmonic), M-mode, colour flow, cont<strong>in</strong>uous andpulsed wave Doppler exam<strong>in</strong>ation. A frequency of 1.7 MHzfrequency with harmonic imag<strong>in</strong>g was selected <strong>for</strong> adequatepenetration and resolution. Depth sett<strong>in</strong>gs, overall ga<strong>in</strong>,TGC, colour and spectral Doppler sett<strong>in</strong>gs and focal zoneswere set to allow optimal imag<strong>in</strong>g of structures of <strong>in</strong>terest.The mechanical <strong>in</strong>dex (MI) was 1.0 and the thermal <strong>in</strong>dex(TI) was 0.7–1.5. The total imag<strong>in</strong>g time was 30 m<strong>in</strong>utes.TechniqueParasternal long axis views of the left ventricle showedmild to moderately impaired systolic contraction with mildantero-septal wall hypok<strong>in</strong>esis and severe posterior hypok<strong>in</strong>esis.The mitral valve appeared mildly echodense withnormal leaflet excursion. The aortic valve appeared mildlyechodense with normal excursion and cusp separation.M-mode through the aortic valve demonstrated a normalsized aortic root and, superiorly, a normal ascend<strong>in</strong>g aortawith mild dilatation of the left atrium. M-mode across themitral valve showed an <strong>in</strong>crease <strong>in</strong> the mitral valve E po<strong>in</strong>tto septal separation (EPSS) <strong>in</strong>dicat<strong>in</strong>g left ventricular dilatation.M-mode through the left ventricle showed a mildly<strong>in</strong>creased left ventricular end-diastolic dimension andreduced systolic thicken<strong>in</strong>g of both the antero-septal andposterior walls. The calculated ejection fraction (afterTeicholtz and Simpson) was 37%. There was mild concentricleft ventricular hypertrophy.Colour Doppler revealed a very mild central jet of aorticregurgitation and mild mitral regurgitation.The right ventricular <strong>in</strong>flow view showed a normal tricuspidvalve with normal valve excursion. The right atriumappeared mildly dilated. Colour Doppler revealed a milddegree of tricuspid regurgitation. The cont<strong>in</strong>uous waveDoppler across the jet shows a pressure difference betweenthe right ventricle and right atrium of 39 mmHg with spectralbroaden<strong>in</strong>g <strong>in</strong>dicat<strong>in</strong>g mild severity.The right ventricular outflow tract view with colourDoppler and cont<strong>in</strong>uous wave Doppler across the pulmonaryvalve showed normal outflow velocities.The parasternal short axis view showed the commissureof the non-coronary aortic cusp was mildly thickened. Theleft ventricle visualised at the level of the papillary musclesshowed a mild to moderate global impairment <strong>in</strong> systolicfunction.Apical views of the mitral valve and tricuspid valvesshowed normal excursion. The left ventricular lateral andseptal walls showed reduced contraction with impaired contractionof the lateral wall of the right ventricle, mild bi-atrialASUM <strong>Ultrasound</strong> Bullet<strong>in</strong> 2005 August; 8 (3)31













