technologies, designs <strong>and</strong> local maintenance, management <strong>and</strong> financing arrangements.Users need to underst<strong>and</strong> the implications of each choice in terms of costs, durability,feasibility <strong>and</strong> the benefits <strong>and</strong> limitations for socio-economic development <strong>and</strong> health.Local capacities for maintenance <strong>and</strong> management must be developed. Only wheninfrastructure is well chosen, maintained <strong>and</strong> managed from the perspective of the differentuser groups can hygienic use be promoted.Poor drainage at water points creates new health hazardsIt is critical that promotion of better personal hygiene should not increase the health risksfrom other related sources. There is, for example, the danger that encouraging people tobathe at water points may lead to stagnant water pools. They provide breeding grounds formosquitoes that transmit malaria, filariasis <strong>and</strong> dengue. In semi-arid areas of India, thenumber of cases of filariasis multiplied when piped water supplies were installed withoutproper drainage <strong>and</strong> drainage management (Wijk, 1998). In the case of malaria, those whohave not yet built up their resistance (young children) or have lost it (e.g. HIV-infectedwomen <strong>and</strong> men <strong>and</strong> the elderly) run the greatest risks. In Africa, one in four childhooddeaths is attributed to malaria. The point here is not that bathing at water points should bebanned; it is that the water points should be designed to permit bathing, with appropriatedrainage of the wash water. Gender considerations are important too. A project orcommunity rule that simply forbids women from washing at water points for fear ofdrainage makes no sense when it means that the women have to carry all water forwashing <strong>and</strong> bathing home (where drainage may be inadequate anyway, so the same risksapply).The important lessons are that hygiene promotion cannot replace participation of thedifferent user groups in the planning <strong>and</strong> design of community water supply <strong>and</strong> sanitationprojects <strong>and</strong> that to obtain the optimum benefits from good hygiene, improved hardwarehas to reach all households in the community. Keeping up coverage is as important forhealth <strong>and</strong> economic reasons as it is a matter of social necessity.EHP has introduced a conceptual framework for ensuring that hardware, software <strong>and</strong> theright enabling environment are combined in WSH programmes. This <strong>Hygiene</strong> ImprovementFramework, illustrated in the next paragraph, was the topic for an electronic conference inMarch 2002.<strong>Hygiene</strong> Improvement FrameworkField studies have demonstrated that water supply, sanitation <strong>and</strong> hygiene can each be aneffective means to prevent diarrhoea. These studies point to two conclusions. First,improved water quality <strong>and</strong> quantity prevent diarrhoea, but excreta disposal <strong>and</strong>h<strong>and</strong>washing also have a significant impact. Second, interventions aimed at hygiene suchas h<strong>and</strong>washing can have as big an impact in preventing diarrhoeal diseases as hardware.For those interested it is available in word as well as a .pdf:• <strong>Hygiene</strong> Improvement Framework (Word file - 987KB)(http://www.ehproject.org/pubs/globalhealth/hif-bw.doc)12 <strong>Hygiene</strong> promotion
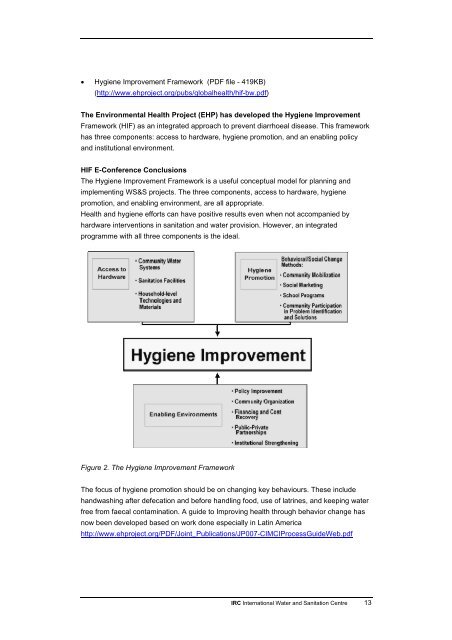
• <strong>Hygiene</strong> Improvement Framework (PDF file - 419KB)(http://www.ehproject.org/pubs/globalhealth/hif-bw.pdf)The Environmental Health Project (EHP) has developed the <strong>Hygiene</strong> ImprovementFramework (HIF) as an integrated approach to prevent diarrhoeal disease. This frameworkhas three components: access to hardware, hygiene promotion, <strong>and</strong> an enabling policy<strong>and</strong> institutional environment.HIF E-Conference ConclusionsThe <strong>Hygiene</strong> Improvement Framework is a useful conceptual model for planning <strong>and</strong>implementing WS&S projects. The three components, access to hardware, hygienepromotion, <strong>and</strong> enabling environment, are all appropriate.Health <strong>and</strong> hygiene efforts can have positive results even when not accompanied byhardware interventions in sanitation <strong>and</strong> water provision. However, an integratedprogramme with all three components is the ideal.Figure 2. The <strong>Hygiene</strong> Improvement FrameworkThe focus of hygiene promotion should be on changing key behaviours. These includeh<strong>and</strong>washing after defecation <strong>and</strong> before h<strong>and</strong>ling food, use of latrines, <strong>and</strong> keeping waterfree from faecal contamination. A guide to Improving health through behavior change hasnow been developed based on work done especially in Latin Americahttp://www.ehproject.org/PDF/Joint_Publications/JP007-CIMCIProcessGuideWeb.pdf<strong>IRC</strong> <strong>International</strong> <strong>Water</strong> <strong>and</strong> <strong>Sanitation</strong> <strong>Centre</strong> 13
- Page 2: Please note that the TOPs are a web
- Page 7 and 8: 1. Hygiene PromotionWhat do you kno
- Page 9 and 10: 2. Why hygiene promotion matters2.1
- Page 11 and 12: • The costs of inaction can be hi
- Page 13: 3. Learning from experiences and re
- Page 17 and 18: groups, and facilitators of partici
- Page 19 and 20: The diagrams are taken from McKee
- Page 21 and 22: • Food, utensils and food prepara
- Page 23 and 24: Guides for developing hygiene promo
- Page 25 and 26: • What may prevent this change in
- Page 27 and 28: areas, slabs and sanplats for latri
- Page 29 and 30: often not taken seriously and their
- Page 31 and 32: IIIIIIIVVInputsProcOutpEffectiImpae
- Page 33 and 34: over for reasons of hierarchy, e.g.
- Page 35 and 36: 5. Case studiesOn the following pag
- Page 37 and 38: The Project recognises the importan
- Page 39 and 40: almost all cases been exceeded, as
- Page 41 and 42: skin diseases, HIV/AIDS and tubercu
- Page 43 and 44: understanding of the importance of
- Page 45 and 46: councils (JSCs) are associations of
- Page 47 and 48: o through a schools programme, with
- Page 49 and 50: outputs and outcomes are focused mo
- Page 51 and 52: Harvey, Eric, Shadrack Dau, Alana P
- Page 53 and 54: programmes more effective. The obje
- Page 55 and 56: scale. Comparison is on approach, l
- Page 57 and 58: Hygiene Behaviour Network, in Globa
- Page 59 and 60: WHO - World Health Organizationhttp
- Page 61 and 62: Tel: (703) 247-8730Fax: (703) 243-9
- Page 63 and 64: Manila, PhilippinesTel: +632 911-57
- Page 65 and 66:
TOP Courses and conferencesCREPA, B
- Page 67 and 68:
TOP ReferencesBoot, Marieke T. and
- Page 69 and 70:
TOP Quiz on Hygiene PromotionTry it
- Page 71 and 72:
Question 4All the interventions wil
- Page 73 and 74:
Then you may decide that this paper
- Page 75 and 76:
Appendix 1. Hygiene promotion manua
- Page 77 and 78:
2. Target specific audiences.These
- Page 79 and 80:
Appendix 4. WASH facts and figures1
- Page 81 and 82:
Research)18: (IHE Newsletter, Janua
- Page 83 and 84:
Appendix 6. Preventive measuresMeas
- Page 85 and 86:
Appendix 8. Some key objectives for
- Page 87 and 88:
Appendix 9. Participatory tools and
- Page 89 and 90:
Appendix 10. The PHAST approachFor
- Page 91 and 92:
Planning techniques are used to sim
- Page 93 and 94:
While sensitive topics are often be
- Page 95:
About IRCIRC facilitates the sharin