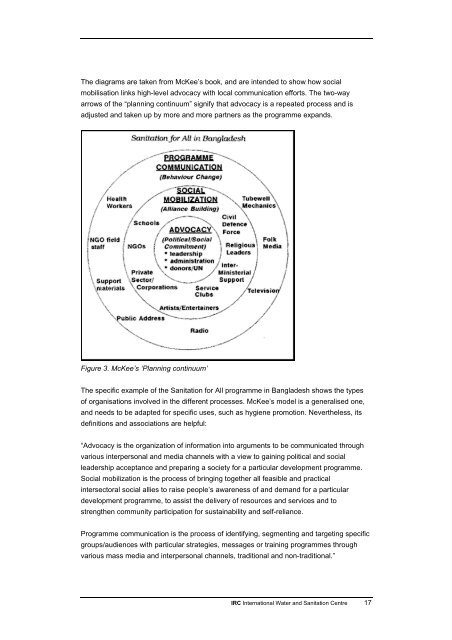
According to this model, an individual will take up a new practice when he or she believesthat the practice has sufficient benefits – health or otherwise – <strong>and</strong> considers thesebenefits important. He or she may then develop a positive attitude to the change. Positiveor negative influence, or subjective norms, from others in the person’s environment whoare important to him or her, will also influence their decision to try the new practice.Table 1: BASNEF Model. The model was first described by John Hutley in 1993.InfluencesActions neededBeliefs, Attitudes(individual)Culture, values, traditions,mass media, education,experiencesCommunicationprogrammes to modifybeliefs <strong>and</strong> valuesSubjective NormsCommunication directed atFamily, community, social(community)persons in family <strong>and</strong>network, culture, social change,community who havepower structure, peer pressureinfluenceEnabling Factors (intersectoral)Income/poverty, sanitationservices, women's status,inequalities, employment,agricultureProgrammes to improveincome, sanitation provision,situation of women, housing,skill trainingSkills, time <strong>and</strong> means (“enabling factors”) are also required to take up the practice. Whenthe new practice is then actually found to have immediate benefits – a cleanerenvironment, less hardship, recognition from respected others – it is most likely to becontinued. Improved health is seldom such an immediate benefit. It is therefore often not amajor reason why the new practice is adopted, although when asked people will often givethis reason as they know that this is the expected answer.In his 220-page book published in 1992 <strong>and</strong> reprinted with updates in 1993, Neill McKeepresents a model that seeks to address what he calls the “anthropologist’s dilemma”. Theconcern is that directing people’s own beliefs towards practices favoured by the “socialmarketer” may be seen as manipulative <strong>and</strong> even reinforcing mistaken beliefs. Headdresses too the problem that, although participatory processes can be designed not tofavour the better off, they may well favour the better participators, who can then directinvestments towards their own priorities. McKee is provocative <strong>and</strong> challenging with viewsalso on the costs of participation through lost opportunities for productive activities. Hismodel (see Figure 3) links Advocacy, Social Mobilization <strong>and</strong> Programme Communicationin a three-circle “planning continuum”. The aim is to combine the benefits of participatoryprocesses to achieve local behaviour change with advocacy <strong>and</strong> communication tools tomobilise all stakeholders for replication of success <strong>and</strong> regular repetition of advocacymessages to keep political leadership on board. For anyone wanting to design a full-scalehygiene promotion programme covering a big area, Chapter 5 of McKee’s book is astimulating pointer to the critical issues that need to be addressed.16 <strong>Hygiene</strong> promotion
The diagrams are taken from McKee’s book, <strong>and</strong> are intended to show how socialmobilisation links high-level advocacy with local communication efforts. The two-wayarrows of the “planning continuum” signify that advocacy is a repeated process <strong>and</strong> isadjusted <strong>and</strong> taken up by more <strong>and</strong> more partners as the programme exp<strong>and</strong>s.Figure 3. McKee’s ‘Planning continuum’The specific example of the <strong>Sanitation</strong> for All programme in Bangladesh shows the typesof organisations involved in the different processes. McKee’s model is a generalised one,<strong>and</strong> needs to be adapted for specific uses, such as hygiene promotion. Nevertheless, itsdefinitions <strong>and</strong> associations are helpful:“Advocacy is the organization of information into arguments to be communicated throughvarious interpersonal <strong>and</strong> media channels with a view to gaining political <strong>and</strong> socialleadership acceptance <strong>and</strong> preparing a society for a particular development programme.Social mobilization is the process of bringing together all feasible <strong>and</strong> practicalintersectoral social allies to raise people’s awareness of <strong>and</strong> dem<strong>and</strong> for a particulardevelopment programme, to assist the delivery of resources <strong>and</strong> services <strong>and</strong> tostrengthen community participation for sustainability <strong>and</strong> self-reliance.Programme communication is the process of identifying, segmenting <strong>and</strong> targeting specificgroups/audiences with particular strategies, messages or training programmes throughvarious mass media <strong>and</strong> interpersonal channels, traditional <strong>and</strong> non-traditional.”<strong>IRC</strong> <strong>International</strong> <strong>Water</strong> <strong>and</strong> <strong>Sanitation</strong> <strong>Centre</strong> 17
- Page 2: Please note that the TOPs are a web
- Page 7 and 8: 1. Hygiene PromotionWhat do you kno
- Page 9 and 10: 2. Why hygiene promotion matters2.1
- Page 11 and 12: • The costs of inaction can be hi
- Page 13 and 14: 3. Learning from experiences and re
- Page 15 and 16: • Hygiene Improvement Framework (
- Page 17: groups, and facilitators of partici
- Page 21 and 22: • Food, utensils and food prepara
- Page 23 and 24: Guides for developing hygiene promo
- Page 25 and 26: • What may prevent this change in
- Page 27 and 28: areas, slabs and sanplats for latri
- Page 29 and 30: often not taken seriously and their
- Page 31 and 32: IIIIIIIVVInputsProcOutpEffectiImpae
- Page 33 and 34: over for reasons of hierarchy, e.g.
- Page 35 and 36: 5. Case studiesOn the following pag
- Page 37 and 38: The Project recognises the importan
- Page 39 and 40: almost all cases been exceeded, as
- Page 41 and 42: skin diseases, HIV/AIDS and tubercu
- Page 43 and 44: understanding of the importance of
- Page 45 and 46: councils (JSCs) are associations of
- Page 47 and 48: o through a schools programme, with
- Page 49 and 50: outputs and outcomes are focused mo
- Page 51 and 52: Harvey, Eric, Shadrack Dau, Alana P
- Page 53 and 54: programmes more effective. The obje
- Page 55 and 56: scale. Comparison is on approach, l
- Page 57 and 58: Hygiene Behaviour Network, in Globa
- Page 59 and 60: WHO - World Health Organizationhttp
- Page 61 and 62: Tel: (703) 247-8730Fax: (703) 243-9
- Page 63 and 64: Manila, PhilippinesTel: +632 911-57
- Page 65 and 66: TOP Courses and conferencesCREPA, B
- Page 67 and 68: TOP ReferencesBoot, Marieke T. and
- Page 69 and 70:
TOP Quiz on Hygiene PromotionTry it
- Page 71 and 72:
Question 4All the interventions wil
- Page 73 and 74:
Then you may decide that this paper
- Page 75 and 76:
Appendix 1. Hygiene promotion manua
- Page 77 and 78:
2. Target specific audiences.These
- Page 79 and 80:
Appendix 4. WASH facts and figures1
- Page 81 and 82:
Research)18: (IHE Newsletter, Janua
- Page 83 and 84:
Appendix 6. Preventive measuresMeas
- Page 85 and 86:
Appendix 8. Some key objectives for
- Page 87 and 88:
Appendix 9. Participatory tools and
- Page 89 and 90:
Appendix 10. The PHAST approachFor
- Page 91 and 92:
Planning techniques are used to sim
- Page 93 and 94:
While sensitive topics are often be
- Page 95:
About IRCIRC facilitates the sharin