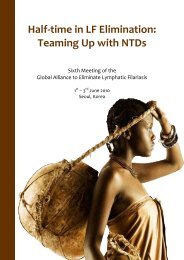
106Annual Report on <strong>Lymphatic</strong> <strong>Filariasis</strong> 2003WALLIS AND FUTUNAOnly Wallis Island is LF-endemic. Wallis and Futunahave a long his<strong>to</strong>ry of vec<strong>to</strong>r control and organizedannual MDAs using DEC alone from 1978 <strong>to</strong> 1987. TheCFA prevalence before MDA was 1% in Wallis. The firstMDA round with the co-administration of DEC plusalbendazole started in 2002, with a reported coverageFigure 3.179 LF at-risk populationof 60.2%. In 2003, 14 600 people were targeted with areported coverage of 63.4%. The distribution strategychosen was booth distribution through schools, offices,shops and village meeting places. Technical support wasprovided by WHO and the Louis Malardé Institute.Figure 3.180 Geographical coverageChapter 3 <strong>Programme</strong> implementationPopulation in millions0.020.010.00Total pop.0.014 MAt-risk pop.0.014 M% of at-risk population covered1007550250100 10020022003Figure 3.181 MDA reported coverageFigure 3.182 IUs with reported coverage >65%100100100 10090808060%%704063.46060.2205020022003020022003
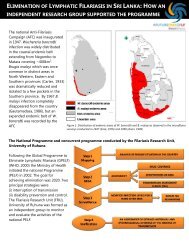
107SOUTH ASIA PROGRAMMEREVIEW GROUP(FORMERLY INDIAN SUBCONTINENT PRG)South Asia PRG consists of five countries — Bangladesh,India, Maldives, Nepal and Sri Lanka — and harbours60% of the world’s LF burden. Both India and Sri Lankahave had filariasis control programmes in place for over50 years. Transition <strong>to</strong> an annual, single-dose MDA strategywas relatively easy and put in<strong>to</strong> operation between1997 and 1998.Sri Lanka, with its efficient health infrastructure and aformidable 50 000-strong volunteer force, has been able<strong>to</strong> target its entire endemic population of 9.8 millionduring the past three years. There was a reported coverageof over 80% in the MDA campaigns of 2002 and2003. An independent assessment of coverage carriedout on 4000 individuals from all eight IUs revealed that79% of the targeted population received the tablets butthat only 71% had taken them. Compliance is thus about10–15% less than the reported figures.India has a major problem, with 450 million people atrisk. MDA campaigns scaled up <strong>to</strong> coverage of 59.5 millionpeople in 2002: 23.8 million were given DEC plusalbendazole and 35.7 million were given DEC only. India’songoing research study on the comparative efficacy ofDEC plus albendazole versus DEC alone has shown sofar that there is no significant difference between thetwo regimens. However, a final review will determinewhat strategy India will use in the future. In the meantime,the population under DEC plus albendazole willnot increase; scaling up will be effected with DEC alone.Because of financial and other constra<strong>int</strong>s, no scaling upoccurred in 2003.In 2001, Bangladesh began MDA in a district of 800 000people and has shown a modest scaling up <strong>to</strong> 4.2 millionin 2002 and 6.8 million between 2003 and 2004. Thedistrict has a sound primary health care infrastructurewhich has made it possible <strong>to</strong> carry out house-<strong>to</strong>-housetreatment and achieve over 80% coverage.Nepal, after a few teething problems, started its MDAprogramme in one district with a 500 000 populationand achieved a coverage of 83%. Nepal plans <strong>to</strong> scale up<strong>to</strong> 4.2 million in 2004.In the Maldives, only eight of the 200 islands are LFendemicand the mf prevalence has been below 1%. Asthese surveys were carried out in 1995, the ministry ofhealth has planned <strong>to</strong> carry out another survey of all theendemic islands in 2004 and <strong>to</strong> implement MDA if mfprevalence is over 1% in any of the islands.Bangladesh, Nepal and Sri Lanka have attributed theirachievement of over 80% coverage <strong>to</strong> two key fac<strong>to</strong>rs: agood health infrastructure and vigorous social mobilization.All three countries carried out a comprehensiveCOMBI programme in the weeks prior <strong>to</strong> MDA. A greatdeal of effort was put in<strong>to</strong> the COMBI exercise, includingappropriate training and orientation programmes forhealth staff at all levels and for volunteers. Of course, theCOMBI programme has been costly; it has been funded bythe Liverpool LF Support Centre, WHO, USAID and others.Sustainability of the programme as MDA is scaled upis bound <strong>to</strong> be difficult. The country teams have realizedthat some of the COMBI components have shown verypromising results while others are probably not reachingenough people. For example, use of microphones <strong>to</strong>address the community is ranked as one of the best <strong>to</strong>olsfor social mobilization; in contrast, messages on televisionare probably ineffective. It should therefore be possible<strong>to</strong> cut costs by retaining only the components thateach country feels are worth using. Country teams mustbe cautioned, however, that reducing COMBI componentsshould only be done in consultation with social scientists.One of the major constra<strong>int</strong>s <strong>to</strong> scaling up MDA is inadequatefinancial resources. In spite of substantial contributionsby the various ministries of health, the Liverpool LFSupport Centre, WHO, the World Bank, USAID, AusAIDand others, countries such as Bangladesh and Nepal arefinding it very difficult <strong>to</strong> expand their programmes.Unless some sustainable solution is found it will be impossible<strong>to</strong> attain the targets that have been set.Although much attention has been paid <strong>to</strong> MDA, thesame concern has not been shown <strong>to</strong> the prevention andcontrol of LF-associated disability. So far, filariasis clinicshave been used on an ad hoc basis <strong>to</strong> treat clinicalfilariasis and <strong>to</strong> impart health education on preventionAnnual Report on <strong>Lymphatic</strong> <strong>Filariasis</strong> 2003Chapter 3 <strong>Programme</strong> implementation