Global Programme to Eliminate Lymphatic Filariasis ... - libdoc.who.int
Global Programme to Eliminate Lymphatic Filariasis ... - libdoc.who.int
Global Programme to Eliminate Lymphatic Filariasis ... - libdoc.who.int

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
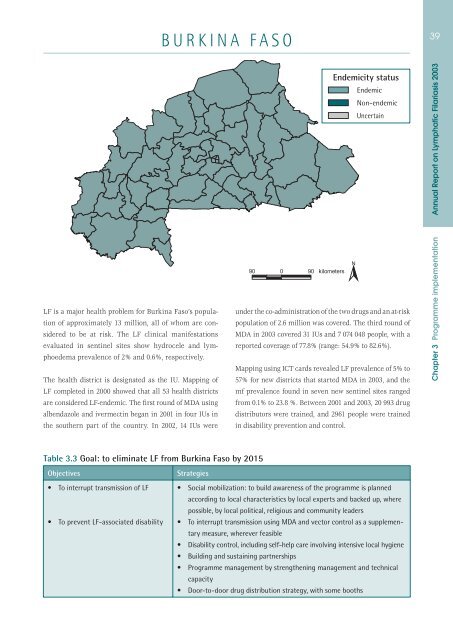
BURKINA FASO39Endemicity statusEndemicNon-endemicUncertainAnnual Report on <strong>Lymphatic</strong> <strong>Filariasis</strong> 2003LF is a major health problem for Burkina Faso’s populationof approximately 13 million, all of <strong>who</strong>m are considered<strong>to</strong> be at risk. The LF clinical manifestationsevaluated in sentinel sites show hydrocele and lymphoedemaprevalence of 2% and 0.6%, respectively.The health district is designated as the IU. Mapping ofLF completed in 2000 showed that all 53 health districtsare considered LF-endemic. The first round of MDA usingalbendazole and ivermectin began in 2001 in four IUs <strong>int</strong>he southern part of the country. In 2002, 14 IUs wereunder the co-administration of the two drugs and an at-riskpopulation of 2.6 million was covered. The third round ofMDA in 2003 covered 31 IUs and 7 074 048 people, with areported coverage of 77.8% (range: 54.9% <strong>to</strong> 82.6%).Mapping using ICT cards revealed LF prevalence of 5% <strong>to</strong>57% for new districts that started MDA in 2003, and themf prevalence found in seven new sentinel sites rangedfrom 0.1% <strong>to</strong> 23.8 %. Between 2001 and 2003, 20 993 drugdistribu<strong>to</strong>rs were trained, and 2961 people were trainedin disability prevention and control.Chapter 3 <strong>Programme</strong> implementationTable 3.3 Goal: <strong>to</strong> eliminate LF from Burkina Faso by 2015Objectives• To <strong>int</strong>errupt transmission of LF• To prevent LF-associated disabilityStrategies• Social mobilization: <strong>to</strong> build awareness of the programme is plannedaccording <strong>to</strong> local characteristics by local experts and backed up, wherepossible, by local political, religious and community leaders• To <strong>int</strong>errupt transmission using MDA and vec<strong>to</strong>r control as a supplementarymeasure, wherever feasible• Disability control, including self-help care involving <strong>int</strong>ensive local hygiene• Building and sustaining partnerships• <strong>Programme</strong> management by strengthening management and technicalcapacity• Door-<strong>to</strong>-door drug distribution strategy, with some booths